

To the Editor:
The etiology of systemic sclerosis (SSc) remains elusive, but microangiopathy is considered to be significantly associated with disease pathophysiology1.
Morphological microvascular studies in patients with SSc use nailfold videocapillaroscopy (NVC) to examine the papillary capillaries in the nail bed, which run with their major axis parallel to the skin surface2 (Figure 1a). Cutaneous telangiectases (TA) are small enlarged end vessels, mainly permanent dilatation of postcapillary venules of the subpapillary plexus3. They are readily visible; nevertheless, few studies have focused on cutaneous TA4.

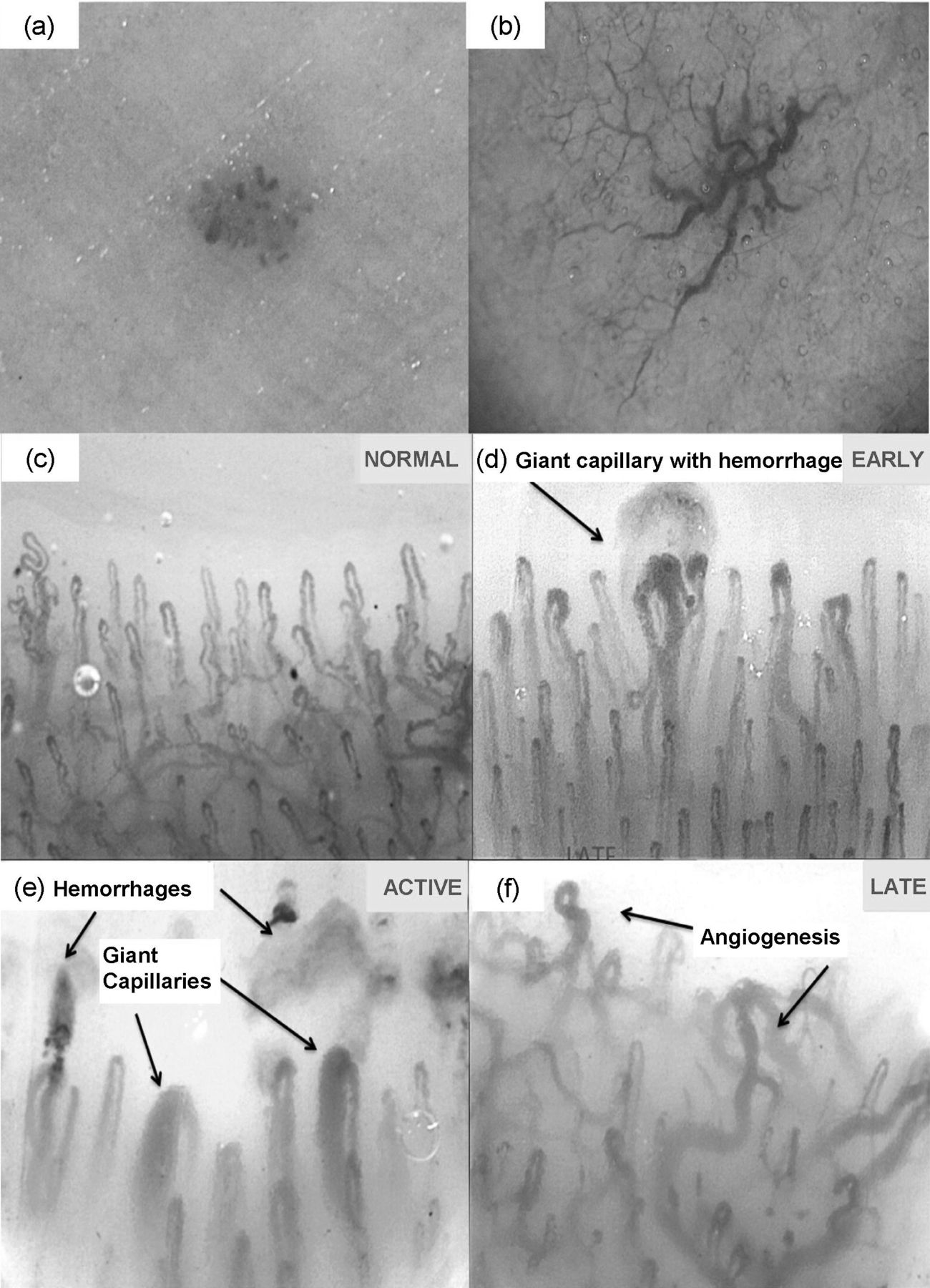
Dermoscopic spot (a) and reticular (b) telangiectases (TA) patterns are detected by using dermoscopy (DC). Nailfold papillary capillaries run parallel to the skin surface (c); in systemic sclerosis (SSc) their profile is altered and nailfold videocapillaroscopy (NVC) detects scleroderma pattern as early (d), active (e), and late (f) (200× magnification). In the other sites of the body (face, hands, chest), microvascular abnormalities may be revealed as TA (40× magnification; DB-Dermo Mips Leica AG).
Dermoscopy (DC) is a noninvasive technique used in the early diagnosis of melanoma5 and nonmelanoma skin cancers, as well as inflammatory skin disorders (psoriasis, lichen planus, seborrheic dermatitis)6. The vascular structures of these conditions are detectable by DC, which has also provided data similar to NVC images commonly used in the study of nailfold capillaries in connective tissue diseases7.
In our study, DC was used to better appreciate vascular features of TA on selected anatomic sites (e.g., face, chest, hands, forearms) and to provide a morphological description of altered skin microcirculation in patients with SSc from a novel perspective. Using this approach, capillaries perpendicular to the skin, as well as the deeper portions of cutaneous microcirculation, usually not visible, become visible as they appear similar to TA.
DC patterns were investigated from 31 women with SSc (median age 55 yrs, median disease duration 8 yrs) showing skin TA and grouped into limited (lSSc) and diffuse (dSSc) SSc-subtypes, according to clinical classification. They were investigated for antinuclear antibody (ANA) and specific antibodies, i.e., anticentromere (ACA) and antitopoisomerase (ATA), using standard immunofluorescence and ELISA methods. Patients were all women because of the high prevalence of this disease in this sex.
Two main DC patterns were found (25×/40× magnifications): a spot pattern (uniform rounded patches) and a reticular pattern (a reticular network; Figure 1a, 1b); they correspond to what Maricq, et al labelled as punctate and “mini-spider” using NVC on several areas of cutis and, more recently, others described clinically as matted and stellate TA, respectively8,9.
Based on the prevalence of one pattern to the other, a DC index was created, with ≥ 1 indicating that the reticular DC pattern exceeds the spot pattern. The index was computed by calculating the difference between the number of reticular and spot DC lesions observed in each patient: briefly, an index > 0 indicated that the reticular lesions outnumber the spot lesions.
We then investigated whether there was a relationship between the DC patterns of TA, NVC patterns (early, active, late)2 (Figure 1d, 1e, 1f), SSc clinical subtypes, and severity of disease (modified Medsger’s index; Table 1). In a logistic regression analysis, a DC index ≥ 1 compared to an index ≤ 0 was found to be strongly associated with dSSc (adjusted OR 5.9, 95% CI 0.9–38.5, p = 0.06) and with the late NVC pattern (adjusted OR 13.2, 95% CI 1.7–102.8, p = 0.01), independent of other variables shown in Table 1.
Percentage of patients in each level of each variable of interest within clinical subtype of scleroderma (SSc) and nailfold videocapillaroscopy (NCV) pattern.
DC patterns of TA are related to the architecture of the cutaneous microcirculation under both normal and altered conditions10. The upper horizontal plexus occupies the papillary dermis and the most superficial part of reticular dermis, following an undulating path. Arterioles and accompanying venules join to each other forming a vascular network. From this tangled horizontal plexus, hairpin capillaries rise perpendicularly into the dermal papillae.
Hairpin capillaries run with the major axis parallel to the skin surface2 (Figure 1c) at the nailfold sites and at the mucous membranes, although they have a perpendicular array at other skin sites10. Thus, combining dermoscopic with NVC analysis would allow a more complete vision of SSc microangiopathy. This consists of progressive alteration and rarefaction of papillary capillaries (early, active NVC patterns) and further altered microvessels, ultimately leading to avascular areas (late NVC pattern). In SSc microangiopathy TA occur, consisting of ectasia of subpapillary plexus, detectable by DC, especially in dSSc TA.
We present for the first time preliminary cross-sectional data investigating in vivo SSc TA by ultrastructural, 3-dimensional, and qualitative descriptions of dilated postcapillary venules mainly in horizontal plexus10 and in papillary dermis2,3.
According to our results, DC is able to better identify alterations of the horizontal microvascular plexus (reticular DC TA pattern corresponds to the late NVC pattern) in patients with advanced SSc, whereas NVC allows the early detection of the papillary microvascular damage (early/active NVC pattern) only partially recognized by DC (spot DC TA pattern).
The index here, obtained by the qualitative DC analysis, may represent a potential clinical marker of disease severity, correlating with the other quantitative studies9. Further, it links the excess of reticular TA to diffuse dSSc and late NVC pattern. Indeed, patients with a positive DC index show a 6-fold risk of dSSc occurrence and a 13-fold risk of late NVC pattern occurrence (compared to patients with an index ≤ 0).
This is the first study using dermoscopy to evaluate abnormalities of cutaneous microvessels in SSc TA and to investigate their relationship with NVC patterns.








{kind=link}