

Abstract
Objective. The prevalence of organ complications in scleroderma (systemic sclerosis; SSc) varies by definition used. This study was done to determine the frequency of several features of SSc.
Methods. A search of Medline-Ovid/Embase, PubMed, and Scopus databases from 1980 to November 30, 2011, was conducted to identify relevant articles with at least 50 patients with SSc extracting prevalence of each organ complication. Study quality was assessed using the STROBE (Strengthening The Reporting of OBservational studies in Epidemiology) checklist. Pooled prevalence was calculated using the random effects method. Heterogeneity was quantified using I2.
Results. A total of 5916 articles were identified (913 from Medline-Ovid/Embase, 1009 from PubMed, and 3994 from Scopus); 5665 were excluded, leaving 251 articles for full-text review, with 69 included. Where available, frequencies were also included from the Canadian Scleroderma Research Group. Many severe complications in SSc occur about 15% of the time, including cardiac involvement (15%, 95% CI 6–24), diastolic dysfunction (16%, 95% CI 14–17), estimated pulmonary artery pressure > 40 mm Hg (18%, 95% CI 14–21), pulmonary arterial hypertension by right heart catheterization (15%, 95% CI 12–17), forced vital capacity (FVC) < 70% predicted (15%, 95% CI 12–17), FVC < 80% predicted (17%, 95% CI 12–21), myositis (13%, 95% CI 10–17), inflammatory arthritis (12%, 95% CI 9–16), Sjögren overlap (13%, 95% CI 10–16), and digital ulcers (DU; 15%, 95% CI 10–20); and 15% of DU have complications (amputations 12%, 95% CI 8–16, and hospitalizations 13%, 95% CI 6–21). Scleroderma renal crisis is uncommon but occurs in almost 15% (12%, 95% CI 5–19) of cases of disseminated cutaneous SSc. There is no 15% rule within skin and gastrointestinal tract for SSc.
Conclusion. The “15%” rule for frequency of significant organ involvement in SSc is helpful.
Systemic sclerosis (SSc; scleroderma) is a systemic autoimmune connective tissue disease characterized by autoimmunity, vascular malfunction and inflammation, and fibrosis. Disease subsets can be classified into limited (lcSSc) and diffuse (dcSSc) cutaneous SSc1. Patients with dcSSc usually have more complications2,3. Steen and Medsger reported the prevalence of severe organ complication in dcSSc using the Pittsburgh Scleroderma Databank4. Many other SSc studies from different cohorts have also reported the prevalence of organ complications using different definitions. Our goal was to promote awareness of the prevalence of important organ involvement in SSc to facilitate appropriate screening and investigation. We used a metaanalysis of the published literature, where available, to define the frequency of severe organ complications of SSc and to construct a broad, easily remembered rule to help clinicians remember those frequencies.
MATERIALS AND METHODS
Identification of studies and study population
A comprehensive literature search of the Medline-Ovid/Embase, PubMed, and Scopus databases was conducted, each from 1980 [when the preliminary American College of Rheumatology (ACR) classification criteria for SSc were published] to November 30, 2011. We looked for English-language research articles for adult SSc using the following search terms: scleroderma and systemic sclerosis. We searched for organ complications using the following search terms:
-
Kidney: malignant arterial hypertension, rapidly progressive renal failure, kidney failure, acute kidney/renal failure, glomerulonephritis, scleroderma renal crisis (SRC).
-
Heart: cardiomyopathy, heart failure, ventricular dysfunction, heart block, heart muscle conduction disturbance, myocarditis, pericarditis, pericardial effusion.
-
Pulmonary hypertension: pulmonary hypertension (PH), pulmonary arterial hypertension (PAH).
-
Lung: interstitial lung disease (ILD), pulmonary fibrosis, restrictive lung disease, lung function test, lung fibrosis, spirometry.
-
Gastrointestinal (GI) system: malabsorption, hyperalimentation, intestinal pseudoobstruction, malnutrition, bacterial overgrowth.
-
Muscle: myopathy, myositis, muscle weakness, muscle disease, skeletal muscle/myopathy, polymyositis.
-
Joint: arthritis/chronic arthritis, synovitis, arthropathy, joint erosion.
-
Digital ulcer or ischemic complications: digital ulcer (DU), digital necrosis, digital gangrene, digital loss, digital amputation.
-
Skin: modified Rodnan skin score (mRSS), skin involvement, skin score. Sjögren syndrome (SS).
Studies were included if they provided numerical data (numbers and/or percentages) of the incidence and/or prevalence of the clinical manifestations of interest; and if they provided a definition of or stratified severity for each complication (described below). Studies were excluded if they were case reports/case series, had fewer than 50 patients with SSc, or were review articles. If more than 1 identified study used the same or overlap study population at the same period, the most recent or larger sample-size study was included. If publications from the same group reported different manifestations, each publication was used for nonredundant items. Two reviewers (CM and JP) separately included reports using the inclusion and exclusion criteria. If there was disagreement, the full reports were reviewed and agreement was achieved by consensus.
Severe organ complications included the following:
-
Kidney: documented SRC as defined by new-onset malignant arterial hypertension and/or rapidly progressive glomerulonephritis with serum creatinine rising by at least 20% of baseline with/without microangiopathic hemolytic anemia occurring in both the dcSSc subset and SSc in total. SRC was often defined by the authors of each report.
-
Heart: documented cardiomyopathy with a decrease in left ventricular ejection fraction (LVEF) by echocardiography; symptoms of congestive heart failure; left diastolic dysfunction by echocardiography; arrhythmia attributable to scleroderma heart disease requiring treatment; and symptomatic pericarditis or moderate to large pericardial effusion.
-
PH and PAH: PH was defined by Doppler echocardiography providing estimated systolic (sPAP) or mean pulmonary artery pressure (mPAP). We stratified PH according to the cutoff level of sPAP or mPAP used by each study. PAH was defined by right heart catheterization (RHC).
-
Lung: documented restrictive lung disease using percentage of predicted FVC (FVC % predicted) or total lung capacity (TLC % predicted) by standard pulmonary function testing (PFT). The severity of restriction was classified by FVC % predicted or TLC % predicted used by each study. We did not include ILD defined solely by chest radiograph because it is common in SSc, including asymptomatic patients.
-
GI system: clinically documented malabsorption syndrome, repeated episodes of intestinal pseudoobstruction, or severe GI problems requiring hyperalimentation. Gastroesophageal reflux and dysphagia were not included because they were thought to be very common. We also did not include bacterial overgrowth syndrome because most studies defined this by a variety of tests but it is often a clinical diagnosis in patients with SSc.
-
Muscle: clinically documented (proximal, symmetrical) muscle weakness; proximal muscle weakness with elevated creatine kinase, electromyographic testing (EMG), and muscle biopsy evidence of inflammatory myositis, fulfilling or not fulfilling the Bohan and Peter criteria for myositis5,6, i.e., dermatomyositis (DM)/polymyositis (PM).
-
Arthritis: clinically documented arthritis or synovitis using the swollen joint count (SJC) with/without the tender joint count (TJC) and those with inflammatory arthritis who had erosions on radiographs, which is a subset population. We did not include inflammatory arthritis defined solely by radiographs or ultrasound.
-
Digital ulcer or ischemic complications: clinically documented digital ischemic vasculopathy as prevalent digital ulcer (a loss of continuity of epithelial coverage that can be denuded or covered by a scab or necrotic tissue); current gangrene, necrosis anywhere on the digit, and complications including amputation (autoamputation or surgical) or hospitalization due to digital ulcers. Digital pits/scars and Raynaud’s phenomenon (RP) were not included because they are extremely frequent in SSc.
-
Skin: documented mRSS above various levels and classified to the cutoff levels according to each study definition.
-
SS: documented by fulfilling any standard criteria for diagnosis of SS. The frequency of overlap of SSc with SS was studied. We did not include sicca symptoms with SSc because they have a variety of classification definitions and tests that are not readily pooled.
Study population from the Canadian Scleroderma Research Group (CSRG)
We also studied the prevalence of each organ complication in the database of the CSRG if the data were not currently in the published literature. The CSRG is a multicenter, prospective national registry of adult SSc across Canada. Clinical and laboratory data are collected annually in a comprehensive database of subjects enrolled between August 2004 and April 2010 who fulfilled preliminary ACR (formerly the American Rheumatism Association) criteria for the classification of SSc (scleroderma); or who were diagnosed by their rheumatologist as having SSc. They were included if the prevalence of organ complications was provided. The following CSRG definitions of organ complication were used, because they were predefined and were the same as in other databases where possible. Renal: SRC was recorded from a physician-completed form. Heart: cardiomyopathy was defined as LVEF ≤ 45% by standard echocardiography; conduction system abnormalities were defined as any conduction abnormalities or arrhythmias on electrocardiography; we had no specific information on symptoms of congestive heart failure, and there was no routine reporting of left ventricular diastolic dysfunction by echocardiography; pericarditis was defined as at least moderate pericardial effusion by standard echocardiography; PH was defined with a surrogate: sPAP ≥ 45 mm Hg by standard echocardiography or diagnosis of PAH. Lung: pulmonary restriction was defined by FVC < 70% predicted on PFT. GI system: hyperalimentation and intestinal pseudoobstruction were recorded from the physician-completed standardized forms. Muscle: proximal limb girdle muscle weakness was recorded from physical examination using a score ≤ 4 based on 5-point Likert scale; EMG and muscle biopsies are not provided in the registry. Arthritis was defined clinically as SJC ≥ 1 and TJC ≥ 1. The CSRG database does not include joint radiographs. Digital ulcers and ischemic complications: current digital ulcer(s)/gangrene/amputation were recorded from physical examination (anywhere on the digit), which was recorded at each visit. Skin: The mRSS was recorded. SS was defined by patient questionnaires about sicca symptoms; SS information, such as labial biopsy results, was not recorded.
Data extraction
Data extraction was performed by 1 investigator (CM). The following data were extracted from each study: first author, year of publication, location of study; study design; sample size; and prevalence in number and/or percentage of each organ complication. The prevalence of various organ involvements was extracted from studies, and forest plots were constructed. The CSRG data did not necessarily contain identical definitions, or in some cases, any data for certain outcomes. In addition, if publications from the CSRG database were available, then they were used and the prevalence was not recalculated from the updated database (because the former were papers published in peer-reviewed journals). If publications used distinctively different definitions of a certain organ, the rates were not pooled, resulting in some plots of different definitions of organ involvement. For instance, estimates were not pooled for various FVC cutoff values, and echocardiographic estimates of PH were not pooled with RHC-proven PAH.
Quality assessment
Study quality was assessed by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for cohort, case-control, and cross-sectional studies7,8. The STROBE checklist consists of 22 items: 18 items are common to all 3 study designs and 4 items (6a/6b, 12d, 14c, 15) are specific to cohort, case-control, or cross-sectional studies. The maximum score varies based on the number of applicable items on the checklist. Two items on the checklist (12e and 16c) pertain to statistical methods (12e describes any sensitivity analysis of the main results; 16c is scored where the relative risk is translated into absolute risk for a meaningful time period) so these items were not relevant to all the articles. One item applied only to matched studies (6b), and another only to cohort studies (14c). The maximum attainable score was 32. The purpose of STROBE is not to give a quality score but to ensure clear presentation of reporting.
Statistical analysis
Proportions were pooled with a random effects model9. A random effects model was used because it assumes that true frequencies from the individual studies have a probability distribution, and it assigns a more balanced weight to each study. Forest plots were created to estimate prevalence with 95% CI. The I-square (I2) statistic was used to quantify the magnitude of heterogeneity (i.e., mild 0–30%, moderate 31%–50%, high > 50%), tau-square was the square-root of the between-study variance, and p value was for Cochran’s Q statistic, the classic measure of heterogeneity. Publication bias was determined using funnel plots.
RESULTS
Search results
The literature search identified 5916 potentially relevant articles that were screened for eligibility. A total of 5665 articles were excluded. There were 173 repeated citations among the search terms and/or different databases. Two articles were identified by hand-searching key references. Eleven further articles were excluded: 9 used the same study population at the same period or at least contained the same patients as part of single-center, national, or multinational databases, 1 article selectively collected data on SSc patients with digital ulcers, and 1 had a different definition for organ involvement, yielding 69 articles included in the metaanalysis (Figure 1).

The search strategy. SSc: systemic sclerosis.
Description of studies included
Characteristics of the 69 articles included in the metaanalysis are shown in Table 1. The studies incorporated data for SSc patients from different locations: North America4,12,17,26,27,34,43,58,60,70,76,77, South America16,53, Europe10,11,14,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,47,48,49,50,51,52,57,59,61,62,63,66,68,69,71, Africa55, Asia13,24,25,38,46,54,56,64,65,67,74, and Australia15,44,45,75. Eighty-five percent of the pooled study population from 69 articles were women. The mean age of patients with SSc (at cohort entry or first diagnosis) from 69 articles was 51.7 years (range 29.4–60.5 yrs) and mean disease duration from onset of first non-Raynaud’s symptoms to study period was 8.8 years (range 0.8–15 yrs). The attainable maximum score was 32 for the STROBE checklist and mean score of the 69 articles was 24.9 (range 17–31).
Characteristics of 69 articles included in the metaanalysis.
Frequency of complications in CSRG cohort
There were 1145 SSc patients included from August 18, 2004, to April 27, 2010 (duration of total followup 5 years, 8 months); data were available for analysis from 1043 of these patients according to their disease subset, either lcSSc or dcSSc. Eighty-six percent were women, with mean age 55.4 years and disease duration from onset of first non-Raynaud’s symptoms to baseline visit of 11.0 years. Thirty-eight percent had dcSSc, of whom 117 (10.6% of total) had early dcSSc (< 3 yrs since onset). Frequency of each organ complication in the CSRG cohort is shown in Table 2.
Frequency of organ complications in systemic sclerosis (SSc) from the Canadian Scleroderma Research Group (CSRG).
Analysis
Forest plots were calculated to provide pooled OR estimates (Figure 2) for frequencies of several organs. Frequencies of organ complications in SSc and the dcSSc subset are shown in Table 3: it can be seen that many clinically relevant organ complications occurred in 15% of patients with SSc. For cardiac involvement we had 2 additional categories other than predefined organ system involvement, which were a combination of various cardiac complications in SSc (congestive heart failure, symptomatic pericarditis, symptomatic arrhythmia, and cardiomyopathy, as described above) and within the dcSSc subset, because that is how they were reported in the literature. We did not have pooled prevalence of skin involvement, because there were not at least 2 studies that used the same cutoff level for skin sclerosis by the mRSS.


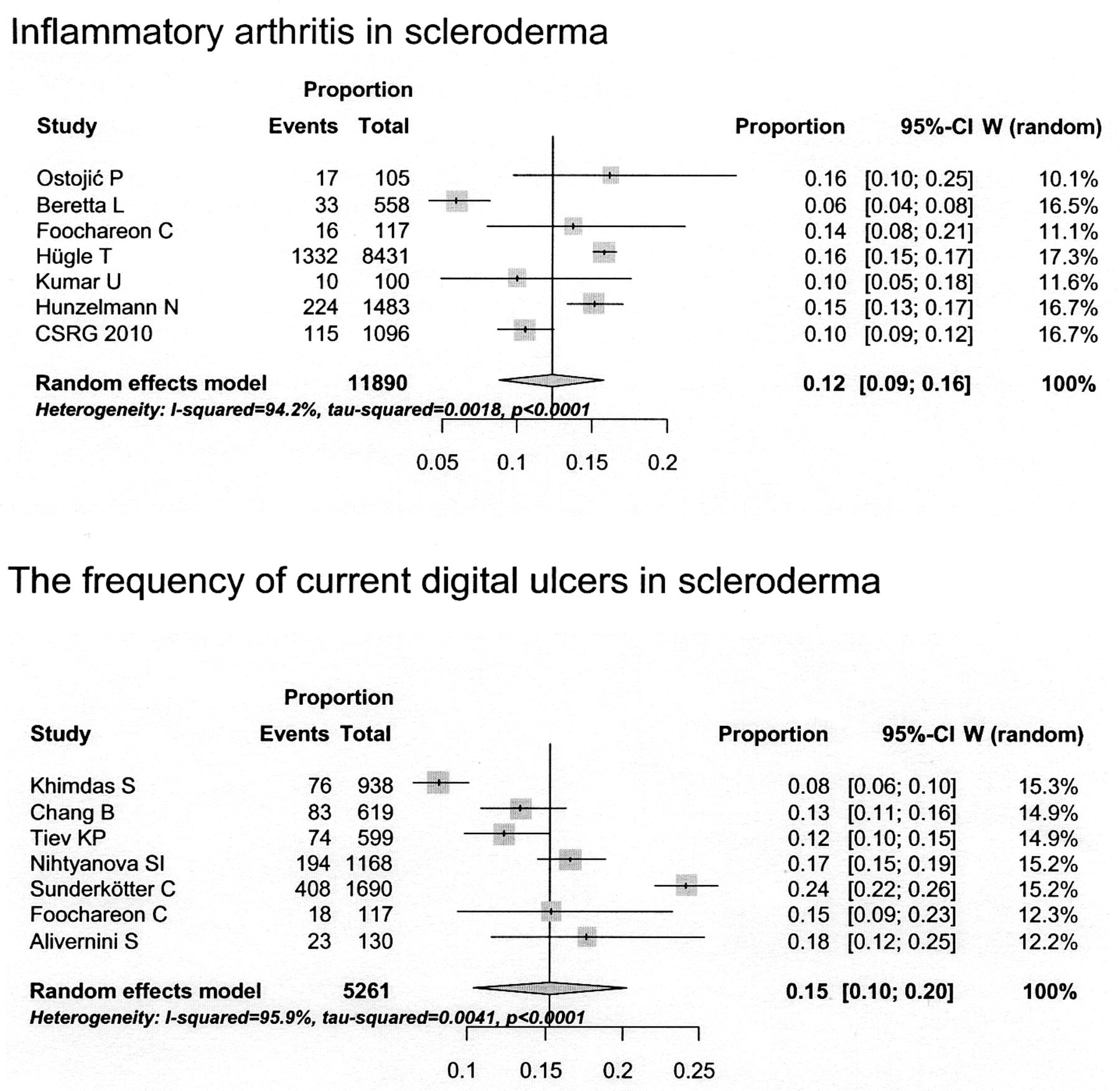
Forest plots of some organ complications in scleroderma.
Summary of frequency of organ complications in systemic sclerosis (SSc).
DISCUSSION
This systematic review reports the prevalence of severe organ complications in patients with SSc, except those very common in SSc such as RP, gastroesophageal reflux disease (GERD), dysphagia, and skin involvement. Data from the CSRG were used because it is a large national database with well-defined complications. Although some definitions of organ involvement were not standardized, we compared studies with similar definitions.
The frequency of organ involvement might change over time by both disease duration and year of publication. This may be true for SRC, which could be decreasing over time. The studies in our metaanalysis included patients with SRC in the period before use of angiotensin-converting enzyme inhibitors and afterward. Small cohorts were not included because their estimates of prevalence of organ involvement would potentially have a large degree of variability. We tried to exclude studies that contained the same patients.
Most organ involvement occurred in about 15% of cases, within the 95% CI. These included pooled data for severe cardiac involvement (congestive heart failure or symptomatic pericarditis, symptomatic arrhythmia, and cardiomyopathy) in both dcSSc and SSc, diastolic dysfunction, symptomatic arrhythmias or conduction abnormalities, and PH, as well as PAH, pulmonary restriction by various definitions of FVC (as a surrogate for ILD), myositis, arthritis, prevalent DU, complicated ulcers ever, and SS. The estimated prevalence of PAH in SSc defined by RHC was 15% (95% CI 12%–17%). When different studies were combined, the prevalence of PH by echocardiography in SSc was 14% (95% CI 8%–20%), prevalence by sPAP > 35 mm Hg was 14% (95% CI 9%–19%), and prevalence by sPAP > 40 or 45 mm Hg was 18% (95% CI 14%–21%). Considering FVC % predicted, the prevalence of FVC % predicted < 80% or 70% was 15% (i.e., for mild restrictive changes), but for very severe pulmonary restriction (FVC % predicted < 50%) the 15% rule did not apply.
SRC in the dcSSc subset was 12% (95% CI 5%–19%), with a wide CI including 15%. Organ involvement that did not meet the 15% criterion included SRC in SSc (3%, 95% CI 3%–4%), cardiomyopathy in SSc (3%, 95% CI 1%–6%), symptomatic congestive heart failure in SSc (5%, 95% CI 1%–9%), symptomatic pericarditis or moderate to large pericardial effusion in SSc (3%, 95% CI 1%–5%), FVC % predicted < 50% in SSc (8%, 95% CI 4%–13%), TLC % predicted < 80% in SSc (23%, 95% CI 22%–25%), malabsorption, intestinal pseudoobstruction and/or severe GI problems requiring hyperalimentation in SSc (5%, 95% CI 3%–6%), proximal muscle weakness (24%, 95% CI 17%–30%), radiographic erosions in those with clinical arthritis in SSc (9%, 95% CI 4%–14%), and digital gangrene in SSc (2%, 95% CI 1%–3%). The estimated prevalence of 15% does not apply to RP, GERD, and skin involvement by various mRSS cutoff scores (which we did not include in the analyses). The estimated prevalence of 15% for significant organ involvement in SSc is not a universal rule, but can help clinicians to be aware of the frequency of several complications of SSc.
A random effects model was used to pool the studies. However, differences in features of the study population in each cohort, such as ethnicity78,79,80, geography78, socioeconomic status79,80, disease subtype, disease duration, environmental factors, variable definitions of organ involvement, and other unknown factors/potential confounders, resulted in clinical heterogeneity of most of the pooled studies. Cohorts from Japan, India, and Thailand had lower age at disease onset compared to those from Europe and North America. Asian cohorts also had more pulmonary complications78 and fewer digital ulcers26. Chinese patients experienced less SRC but more myositis compared to Europeans27. Pulmonary fibrosis occurred more often and was more severe in African Americans compared to whites79,80, and they had pulmonary hypertension at a younger age81. Hispanics and African Americans had more diffuse skin involvement, digital ulcers, lower FVC % predicted, and poorer socioeconomic status than whites82,83. Patients with less high school completion were reported to have more arthritis84. Sex and disease subset ratios varied between some cohorts, which could affect the frequency and severity of organ involvement85,86. Therefore, heterogeneity can affect the rate of complications, which is important when pooling data from several cohorts.
We tried to include large studies and as many studies as were available concerning each predefined organ system to diminish the variance, but some organ definitions yielded only a couple of studies where data could be pooled. Pooled studies of at least 4 cohorts for various organ prevalences were analyzed (Table 3), whereas the rates may be less certain and less generalizable in the analyses that included fewer studies. Some definitions of organ involvement had very few studies. There was also statistical heterogeneity (I2 > 50%) in some analyses and results could not be pooled. There may have been publication bias, because some of the funnel plots appeared to have asymmetry, and did not resemble inverted funnels, especially those with fewer or smaller studies (data not shown). Even some larger studies had asymmetrical funnel plots. This may be due to clinical and methodological heterogeneity. Smaller studies or studies from tertiary centers might have been performed in a selected SSc population.
The estimated prevalence of PAH defined by RHC in SSc of 15% (95% CI 12%–17%) was slightly higher than that from a metaanalysis from 5 studies (9%, 95% CI 6%–12%)21. The prevalence of PH in SSc by echocardiography (14%, 95% CI 8%–20%), or by sPAP > 35 mm Hg (14%, 95% CI 9%–19%), or by sPAP > 40 or 45 mm Hg (18%, 95% CI 14%–21%) in our study was roughly consistent with the prevalence of suspected PH by echocardiography leading to RHC (13%, 95% CI 7%–23%) reported by Avouac, et al21.
Some studies had higher than expected prevalence, such as the pooled prevalence of severe cardiac involvement. Also, some frequencies were higher in more severe organ involvement, such as for PH in SSc with sPAP > 35 mm Hg, which should be more frequent than that of sPAP > 40 mm Hg or 50 mm Hg. This can be due to selection bias of patients included in the studies and we could not adjust for this in the analyses.
Another limitation is that a pooled prevalence could not be calculated for every manifestation because some analyses included only 1 publication and different definitions of significant organ involvement were used in the publications (e.g., “severe skin sclerosis” used different cutpoints of the mRSS). The strength of our study is the large number of articles that could be pooled for various complications, and only cohorts that were relatively large were included. Not every organ system fits neatly into the 15% rule, such as GI involvement, RP, SRC (only in the early dcSSc subset), clinical congestive heart failure, etc. However, we observed that the 15% rule is often generalizable. SRC in dcSSc had a wide CI, so the point estimate may actually be different from 15%, but it overlaps 15%.
Many complications in SSc, including ILD as measured by a low percentage-predicted FVC, PAH, diastolic dysfunction, arrhythmias, inflammatory arthritis, myositis, SS, and digital ulcers and their complications, occur in about 15% of patients. SRC is uncommon overall but occurs in almost 15% of the dcSSc subset. The 15% rule of SSc organ involvement may help clinicians be aware of the frequency of many features of SSc.
Acknowledgment
The authors thank Dr. Heather Thiessen Philbrook for creation of forest plots.
APPENDIX 1 List of study collaborators
Investigators of the Canadian Scleroderma Research Group (CSRG): J. Markland, Saskatoon, Saskatchewan; D. Robinson, Winnipeg, Manitoba; N. Jones, Edmonton, Alberta; N. Khalidi, Hamilton, Ontario; P. Docherty, Moncton, New Brunswick; E. Kaminska, Hamilton, Ontario; A. Masetto, Sherbrooke, Quebec; E. Sutton, Halifax, Nova Scotia; J-P. Mathieu, Montreal, Quebec; M. Hudson, Montreal, Quebec; S. Ligier, Montreal, Quebec; T. Grodzicky, Montreal, Quebec; S. LeClercq, Calgary, Alberta; C. Thorne, Newmarket, Ontario; M. Fritzler, Advanced Diagnostics Laboratory, Calgary, Alberta.
Footnotes
-
The Canadian Scleroderma Research Group is supported by the Canadian Institutes of Health Research (CIHR) and the Fonds de Recherché en Santé du Québec; and the Scleroderma Society of Canada, Scleroderma Society of Ontario, Sclérodermie Québec, and Cure Scleroderma Foundation.
- Accepted for publication May 13, 2013.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.
- 73.
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵








{kind=link}
{kind=link}
{kind=link}
{kind=link}