

Abstract
Objective. Apremilast, a specific inhibitor of phosphodiesterase 4, modulates proinflammatory and antiinflammatory cytokine production. A phase IIb randomized, controlled trial (RCT) evaluated the effect of apremilast on patient-reported outcomes (PRO) in psoriatic arthritis (PsA).
Methods. In this 12-week RCT, patients with active disease (duration > 6 mo, ≥ 3 swollen and ≥ 3 tender joints) received apremilast (20 mg BID or 40 mg QD) or placebo. PRO included pain and global assessment of disease activity [visual analog scale (VAS)], Health Assessment Questionnaire-Disability Index (HAQ-DI), Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-F), and Medical Outcomes Study Short-Form 36 Health Survey (SF-36) assessing health-related quality of life (HRQOL). Percentages of patients reporting improvements ≥ minimum clinically important differences (MCID) and correlations between SF-36 domains and pain VAS, HAQ-DI, and FACIT-F were determined.
Results. Among the 204 randomized patients (52.5% men; mean age 50.6 yrs), baseline SF-36 scores reflected large impairments in HRQOL. Apremilast 20 mg BID resulted in statistically significant and clinically meaningful improvements in physical and mental component summary scores and 7 and 6 SF-36 domains, respectively, compared with no change/deterioration in placebo group. Patients receiving apremilast 20 mg BID and 40 mg QD reported significant improvements ≥ MCID in global VAS scores and FACIT-F versus placebo, and significant improvements in pain VAS scores. Moderate-high, significant correlations were evident between SF-36 domains and other PRO.
Conclusion. Apremilast resulted in statistically significant and clinically meaningful improvements in HRQOL, pain and global VAS, and FACIT-F scores.
Psoriatic arthritis (PsA) is a chronic inflammatory arthritis associated with psoriasis1. An estimated 40% of patients with psoriasis develop PsA1,2, with a prevalence in the general US population between 0.3% and 1.0%1. PsA is associated with poor health-related quality of life (HRQOL), including general health, bodily pain, and physical functioning, well below that of age- and sex-matched US norms3,4, and longterm work disability4,5,6. In a survey conducted by the National Psoriasis Foundation, 44% of patients with PsA who were not working reported this was partially or entirely due to their PsA2. The presence of both PsA and psoriasis may further influence HRQOL, with larger impairments than those seen with psoriasis alone7,8,9.
Understanding the effect of new treatments on patient-reported outcomes (PRO) is important when assessing their overall clinical value. The effect on HRQOL may be influenced by treatment-related factors, such as efficacy, tolerability, adverse events, safety, and treatment regimen (e.g., dosing frequency, route of administration, cost). Effective treatment of patients with PsA, including use of disease-modifying antirheumatic drugs (DMARD), has been shown to significantly improve PRO, including HRQOL10,11. However, these benefits differ among agents, with methotrexate (MTX) having a lesser effect on PRO than tumor necrosis factor (TNF) inhibitors9,12. In addition, treatment of patients with traditional and biologic DMARD therapy may be compromised by adverse events, poor tolerability, inconvenient route of administration, and/or injection/infusion reactions13,14,15,16. No oral DMARD therapy is currently approved by the US Food and Drug Administration for treatment of PsA, and there is only limited approval of leflunomide in Europe. Thus, efficacious, well tolerated, and easy-to-use treatment options are needed for patients with PsA.
During the past decade, the role of cyclic adenosine monophosphate (cAMP) in the pathophysiology of chronic inflammatory diseases has generated research interest. cAMP is a naturally occurring intracellular secondary messenger that helps to maintain immune homeostasis17,18. Phosphodiesterase 4 (PDE4) is a cAMP-specific phosphodiesterase and the dominant phosphodiesterase in inflammatory cells19,20,21. Inhibition of PDE4 increases the intracellular concentration of cAMP and modulates a network of proinflammatory and antiinflammatory mediators17,20,22,23. Apremilast (Celgene Corporation), a specific inhibitor of PDE4, works intracellularly to reduce production of proinflammatory mediators, such as TNF-α, interleukin 23 (IL-23), and interferon-γ, and increase production of anti-inflammatory mediators, such as IL-1020. Apremilast has been shown to be effective in the treatment of moderate to severe psoriasis and active PsA24,25,26.
In a phase II, multicenter, randomized, controlled trial (RCT), apremilast 20 mg BID and 40 mg QD showed efficacy and a favorable benefit:risk profile in the management of patients with active PsA25. After 12 weeks, 43.5% of patients receiving apremilast 20 mg BID (p < 0.001) and 35.8% receiving apremilast 40 mg QD (p = 0.002) exhibited ≥ 20% improvements in American College of Rheumatology (ACR20) response criteria versus 11.8% receiving placebo. Improvements were generally maintained over 24 weeks of treatment25. Our report summarizes the influence of apremilast treatment on PRO in this phase II RCT.
MATERIALS AND METHODS
Study design
This multicenter RCT enrolled men and women ≥ 18 years of age with active PsA (duration ≥ 6 months; ≥ 3 swollen joints; ≥ 3 tender joints) and negative rheumatoid factor (RF; titer ≤ 30 IU/ml). Patients must have discontinued systemic therapy for psoriasis and/or PsA, including but not limited to sulfasalazine, leflunomide, chloroquine, hydroxychloroquine, gold compounds, penicillamine, parenteral corticosteroids (including intraarticular), cyclosporine, oral retinoids, mycophenolate mofetil, thioguanine, hydroxyurea, sirolimus, tacrolimus, azathioprine, and fumaric acid esters within 28 days; phototherapy within 28 days; etanercept within 56 days; adalimumab, efalizumab, or infliximab within 84 days; and alefacept within 168 days of randomization. Patients using stable doses of nonsteroidal antiinflammatory drugs (≥ 2 weeks), oral corticosteroids (≥ 4 weeks), and/or MTX (≥ 8 weeks) before screening and throughout the study were eligible for study enrollment; those with erythrodermic, guttate, or pustular forms of psoriasis were excluded. Methods and results were as reported25.
At baseline, eligible patients were randomized 1:1:1 to receive placebo or oral apremilast (20 mg BID or 40 mg QD) for 12 weeks, stratified by concomitant MTX use. At Week 12, placebo patients were rerandomized to receive apremilast 20 mg BID or 40 mg QD until Week 24 in a blinded fashion; all other patients continued to receive their assigned dose of apremilast. Throughout the trial, concomitant treatment with phototherapy or other systemic DMARD, other than MTX, was prohibited. In patients with psoriasis, use of topical agents was prohibited, except coal tar shampoos, nonmedicated Eucerin cream, and low to moderate potency topical corticosteroids for treating psoriatic lesions. This report describes PRO, including HRQOL, at the primary 12-week endpoint.
PRO assessments
Changes from baseline to Week 12 and improvements ≥ minimum clinically important differences (MCID) were determined for PRO, including 3 components of the ACR response criteria, patient-reported pain and global disease activity by visual analog scale (VAS), and Health Assessment Questionnaire Disability Index (HAQ-DI); Functional Assessment of Chronic Illness Therapy for Fatigue (FACIT-F); and the generic Medical Outcomes Study Short-Form 36 Health Survey version 2 (SF-36). Definitions of the MCID for each instrument are summarized in Table 127,28,29,30,31,32.
Statistical analysis
All analyses were performed in the intent-to-treat population who had baseline and ≥ 1 postbaseline assessments, with last-observation-carried-forward used for missing values. Changes from baseline in each score were summarized using descriptive statistics. For continuous measures, Week 12 changes from baseline within treatment groups (apremilast 20 mg BID and 40 mg QD) were compared with placebo using an analysis of covariance model (with treatment as the factor, baseline as the covariate, and blocking for MTX use). If either physical component summary (PCS) and/or mental component summary (MCS) scores of the SF-36 were statistically significant, significance was tested for individual domain scores. Mean changes from baseline in domain scores are displayed using spydergrams33, with quantification of improvements by the health utility SF-6D after the method of Ara and Brazier, based on an algorithm using mean scores across all 8 domains of the SF-3634,35. As a benchmark comparison, without statistical analyses, US normative data were calculated based on age and sex distribution of the protocol population, using published norm-based scoring algorithms based on the 1998 National Survey of Functional Health Status36; no statistical analyses were conducted for differences between US normative data and study findings. Pearson correlations were determined for mean changes from baseline at Week 12 between the generic SF-36 Physical Function (PF), Bodily Pain (BP), and Vitality (VT) domain scores and disease-specific HAQ-DI, pain VAS, and FACIT-F, respectively. Correlations > 0.30 to ≤ 0.60 were considered moderate and > 0.60 high37.
RESULTS
Patients
Of 204 patients randomized, 165 (80.9%) completed 12 weeks of treatment. Baseline demographic and disease characteristics are summarized in Table 2. The sample was composed of roughly equal proportions of men (52.5%) and women (47.5%) who were white (96.6%), overweight/obese (mean body mass index 30.2 kg/m2, SD 5.94), and had had PsA for a mean of 7.8 (SD 8.5) years.
Patient demographic and baseline disease characteristics.
PRO assessments
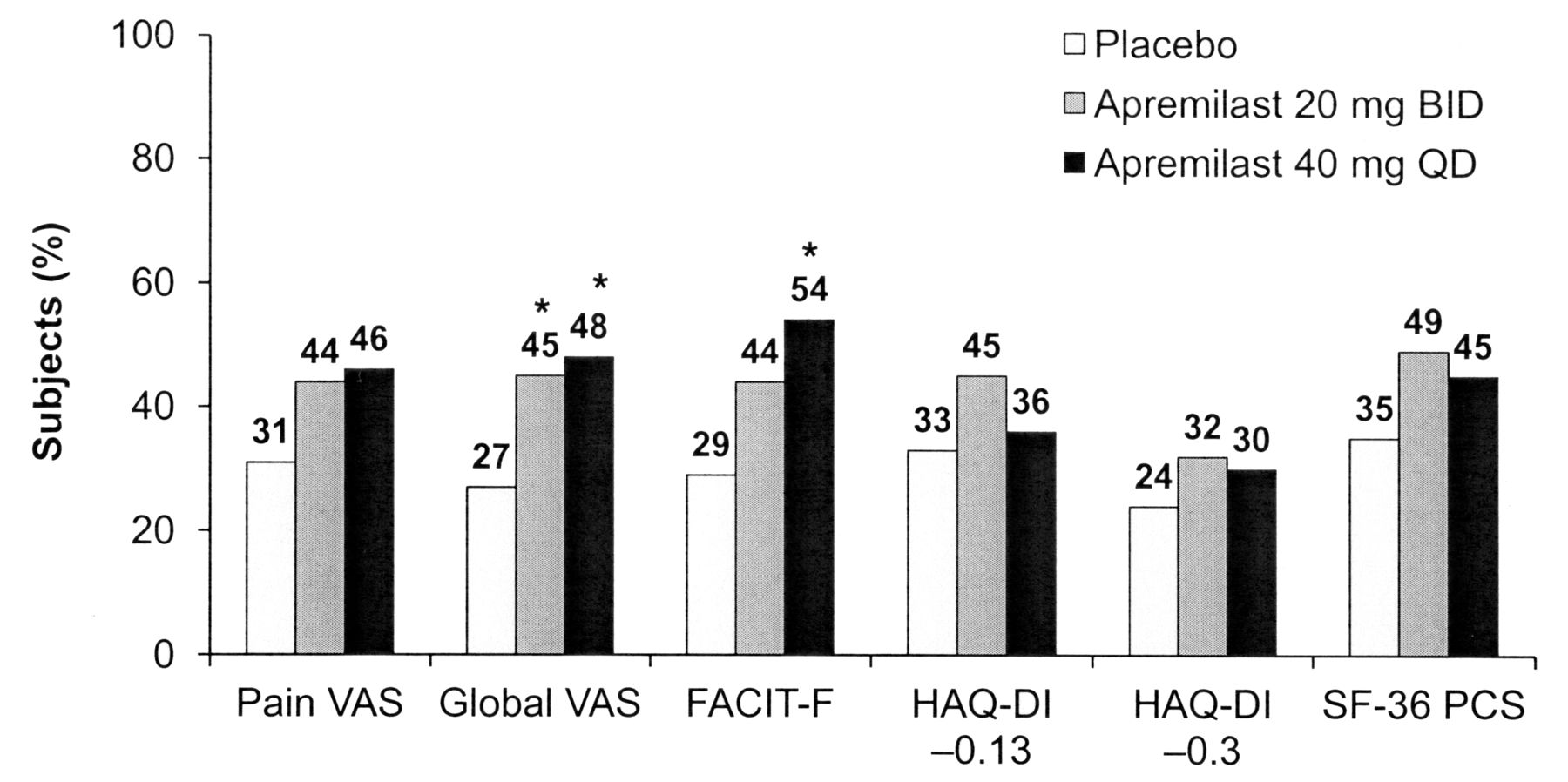
Patient-reported pain and global assessments of disease activity were comparable among treatment groups at baseline and ranged between 54 and 60 mm on a 100-mm VAS scale (Table 3). At Week 12, mean changes in pain VAS scores were significantly greater in patients receiving apremilast 20 mg BID and 40 mg QD (p < 0.05 vs placebo for both doses). Global assessment scores worsened from baseline for placebo group but improved with apremilast 20 mg BID and 40 mg QD (p < 0.05 vs placebo for both doses). As shown in Figure 1, at Week 12, a significantly greater proportion of patients reported improvements ≥ MCID in global assessments with apremilast 20 mg BID (44.9%; p = 0.04) and 40 mg QD (47.8%; p = 0.02) versus placebo. Numerically more patients reported clinically meaningful improvements in pain VAS scores with both apremilast doses versus placebo; however, differences versus placebo were not significant (p ≥ 0.10).
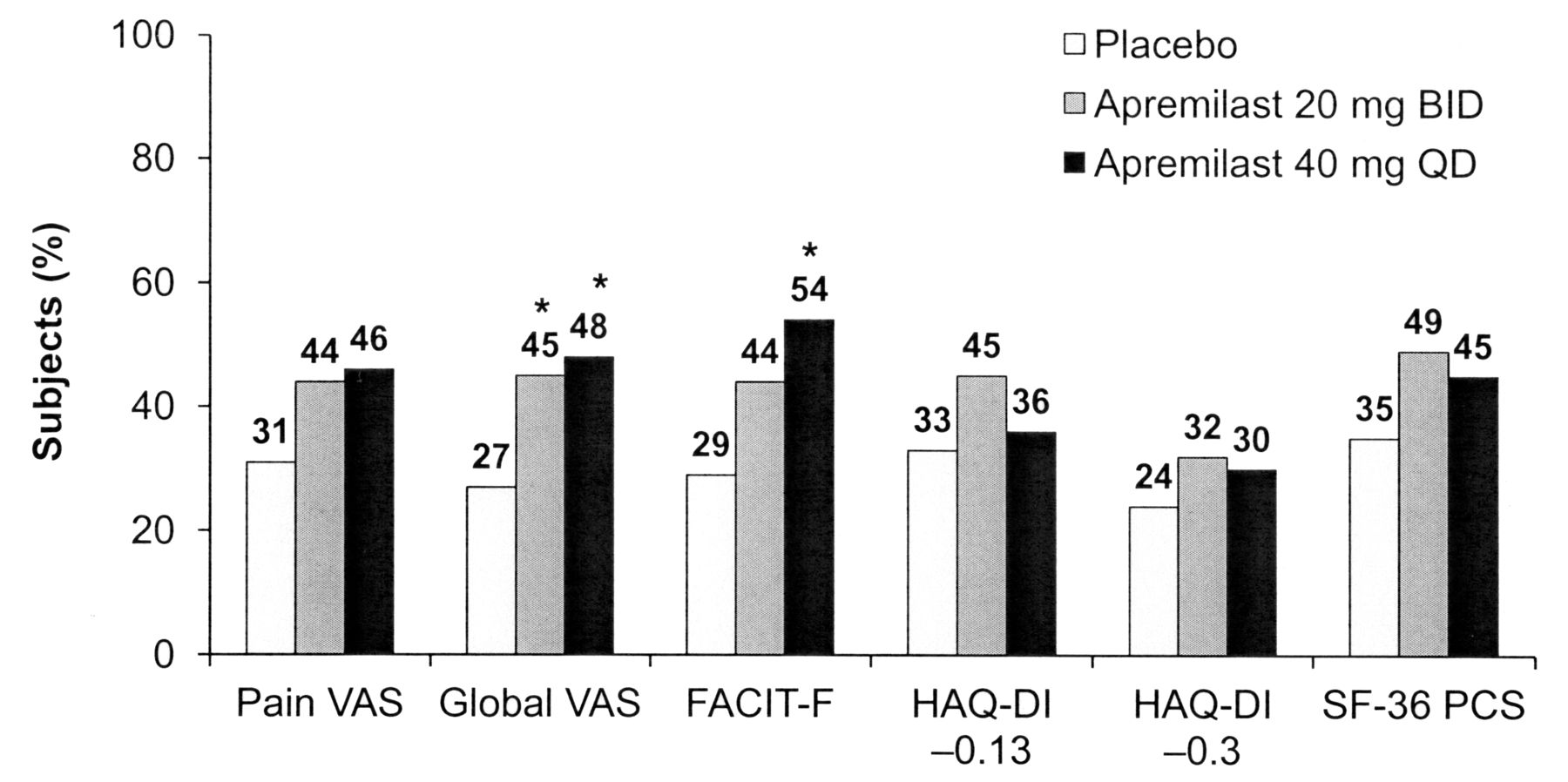
Percentage of patients reporting improvements above the respective MCID of the patient-reported outcomes pain (on VAS), global disease activity (VAS), fatigue (FACIT-F), function (HAQ-DI), and HRQOL (SF-36 PCS). *Significant differences, p < 0.05. FACIT-F: Functional Assessment of Chronic Illness Therapy-Fatigue; HAQ-DI: Health Assessment Questionnaire Disability Index; SF-36 PCS: 36-Item Medical Outcomes Study Short Form-36 Health Survey physical component summary; HRQOL: health-related quality of life; VAS: visual analog scale.
Summary of pain and global VAS scores, FACIT-F, and HAQ-DI.
Changes from baseline in HAQ-DI scores are summarized in Table 3. Mean HAQ-DI scores were similar among treatment groups at baseline (range 0.96–1.24, SD 0.77–0.65). Mean changes from baseline in placebo were small (–0.05), but improved in both active treatment groups (–0.16 and −0.15), which approached MCID. A numerically greater proportion of patients treated with apremilast reported improvements ≥ MCID at Week 12 compared with placebo when MCID was defined as −0.13 or −0.3; however, differences versus placebo were not significant (p ≥ 0.16; Figure 1).
Mean FACIT-F scores and changes from baseline observed at Week 12 in each treatment group are summarized in Table 3. Baseline mean FACIT-F scores were similar across all treatment groups (range 27.7–32.1, SD 12.8–11.9). At Week 12, mean changes in FACIT-F scores were significantly greater (vs placebo) with apremilast 20 mg BID (p = 0.004) and 40 mg QD (p = 0.028). Clinically meaningful improvements in FACIT-F scores were reported by 43.5% and 53.7%, respectively, of patients receiving apremilast 20 mg BID (p = 0.07) and 40 mg QD (p < 0.01; Figure 1).
At baseline, mean PCS and MCS scores were lower than US normative scores of 50 (SD 10), about 1.5 SD less in PCS scores (range 33.3–37.3) and 0.5 SD in MCS scores (range 43.5–45.0). After 12 weeks of treatment, improvements in both PCS and MCS scores were statistically significant with apremilast 20 mg BID [2.4 (p = 0.026) and 3.4 (p = 0.003), respectively, vs placebo] and ≥ MCID, compared with deterioration in placebo; there were numerical but not statistically significant changes with apremilast 40 mg QD. A greater proportion of patients receiving apremilast 20 mg BID and 40 mg QD reported improvements ≥ MCID in PCS scores versus placebo, although differences were not statistically important (Figure 1).
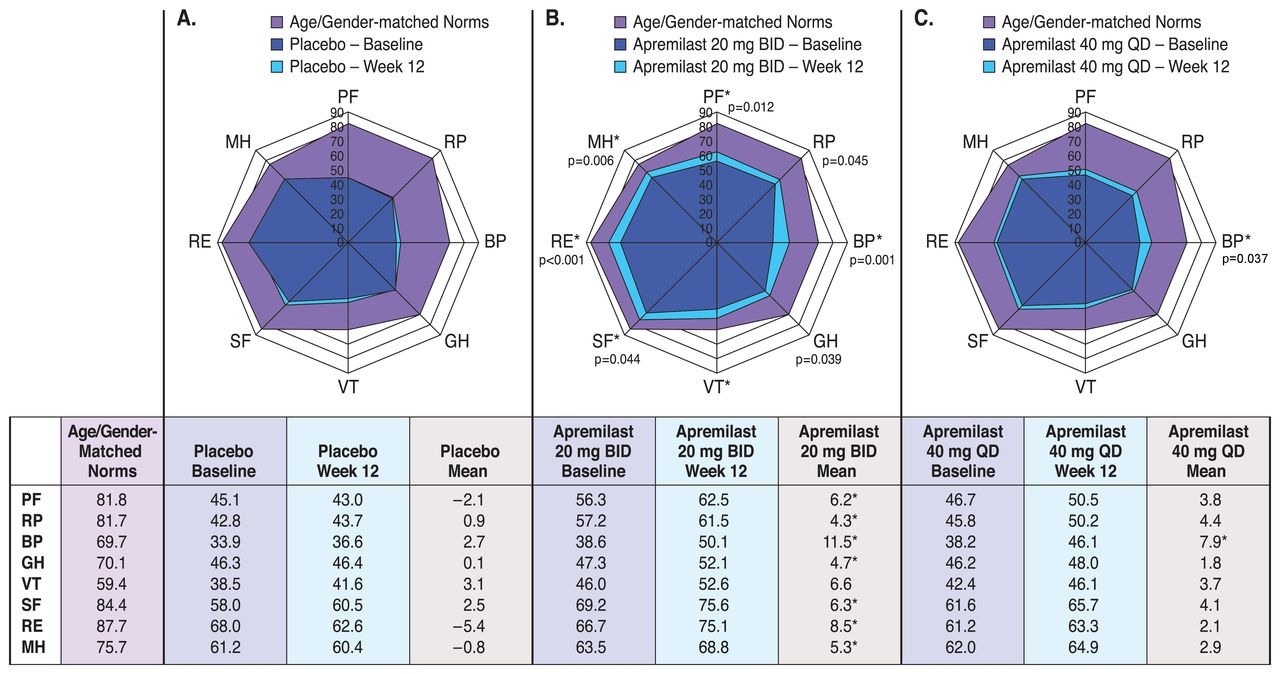
At baseline, SF-36 domain scores in all groups were well below age- and sex-matched US normative values specific to this population by about 20 to 30 points in physical domains and > 10 points in mental domains, indicating large disease-associated impairments in HRQOL. At Week 12, patients receiving placebo reported little improvement in 5 and deterioration in 3 domains of the SF-36, with clinically meaningful worsening in the Role-Emotional (RE) domain (exceeding −2.5 for MCID for deterioration; Figure 2A). Patients treated with apremilast 20 mg BID reported statistically significant (p < 0.05) mean improvements in 7 of 8 domains, which were clinically meaningful in 6 domains (Figure 2B). Among patients treated with apremilast 40 mg QD, statistically significant and clinically meaningful improvement was reported in the BP domain (Figure 2C). SF-6D baseline utility scores were 0.233 to 0.298 lower than age- and sex-matched US norms of 0.821. Treatment-associated improvements in the apremilast 20 mg BID and 40 mg QD groups resulted in mean increases of 0.076 and 0.047 in SF-6D utility scores, respectively, which exceeded the minimum important difference (MID).

A. SF-36 domain scores at baseline and endpoint (Week 12) in patients receiving placebo versus age- and sex-matched norms. Gridlines represent changes of 10 points each, from minimum clinically important differences (MCID) to 2×MCID. An increase in score indicates improvement. Innermost polygon (dark blue): health-related quality of life (HRQOL) reported at baseline. Outer polygon (lavender): age- and sex-matched US normative values specific to this protocol population. Intermediate polygon (light blue): improvements in placebo at endpoint (Week 12). B. SF-36 domain scores at baseline and endpoint in patients receiving apremilast 20 mg BID versus age- and sex-matched norms. Gridlines represent changes of 10 points each (from MCID to 2×MCID). An increase in score indicates improvement. Innermost polygon (dark blue): HRQOL reported at baseline. Outer polygon (lavender): age- and sex-matched US normative values specific to this protocol population. Intermediate polygon (light blue): improvements in apremilast 20 mg BID at endpoint at Week 12, statistically significant in 7 of 8 domains and ≥ MCID in 6. C. SF-36 domain scores at baseline and endpoint in patients receiving apremilast 40 mg QD versus age- and sex-matched norms. Gridlines represent changes of 10 points each (from MCID to 2×MCID). An increase in score indicates improvement. Innermost polygon (dark blue): HRQOL reported at baseline. Outer polygon (lavender): age- and sex-matched US normative values specific to this protocol population. Intermediate polygon (light blue): improvements in apremilast 40 mg QD at endpoint at Week 12, statistically significant and ≥ MCID in the BP domain. *≥ MCID. SF-36: Medical Outcomes Study Short Form-36; BP: Bodily Pain; PF: Physical Function; MH: Mental Health; RE: Role-Emotional; RP: Role-Physical; SF: Social Function; VT: Vitality; GH: General Health.
Table 4 summarizes Pearson correlations between mean changes from baseline in individual domains of SF-36 and pain VAS, HAQ-DI, and FACIT-F scores at Week 12. Statistically significant, high correlations were observed between SF-36 VT domain and FACIT-F with apremilast 20 mg BID and SF-36 PF domain and HAQ-DI with apremilast 40 mg QD (p < 0.001 for both). Moderate correlations, also statistically significant, were evident for all treatment groups between SF-36 BP domain and pain VAS scores and SF-36 PF domain and HAQ-DI as well as SF-36 VT domain with FACIT-F for placebo.
Correlations between mean changes in SF-36 domains and pain VAS, HAQ-DI, and FACIT-F*.
DISCUSSION
At baseline, patients with active PsA reported large impairments in HRQOL, evidenced by SF-36 scores well below US age- and sex-matched norms, especially in the physical but also the mental domains. These findings are consistent with previous reports describing poor HRQOL in RCT and clinical series in PsA and other inflammatory arthritides3,4,9,38. Impaired physical function, by PCS, PF, Role-Physical (RP), BP, and General Health (GH) domains of the SF-36 and HAQ-DI scores reported by patients in this trial, is also consistent with reports of work disability by many individuals with PsA4,5,6.
As shown in other studies, improvements in physical functioning and pain appear prominent among overall HRQOL improvements in patients with PsA9,10,11. The proportion of patients receiving apremilast 20 mg BID who reported improvements in SF-36 domain scores ≥ MCID was generally consistent with the proportion of ACR20 responders in this trial: 43.5% of patients receiving apremilast 20 mg BID and 35.8% of patients receiving apremilast 40 mg QD, published in a separate report25.
Administration of apremilast 20 mg BID was associated with broad improvements in patient-reported HRQOL at 12 weeks, statistically in PCS, MCS, and 7 of 8 domain scores of SF-36; clinically meaningful in MCS and 6 of 8 domain scores; and reflected by more patients receiving 20 mg BID reporting improvements ≥ MCID. In contrast, SF-36 domain scores showed little change or even deterioration with placebo. Importantly, larger changes with both doses of apremilast were reported in the BP domain with the lowest scores at baseline, followed by RE, Social Function (SF), PF, and Mental Health (MH), indicating improvements in social and emotional well-being as well as pain and functioning. Clinically meaningful changes in VT (fatigue, energy, and pep) were not statistically significant, as the largest change in placebo occurred in this domain. While these results are encouraging, this was a relatively short study, and achievement of ACR20 over time indicates that improved response may be seen with longer treatment25; it is hoped that continuing longer-term, phase III studies will better illustrate the effects of apremilast on HRQOL.
Both active doses of apremilast were associated with statistically significant reductions in pain and global VAS scores and FACIT-F versus placebo, all clinically meaningful. These broad improvements across PRO are consistent with the reported changes in SF-36. Moderate to high, statistically significant correlations between SF-36 domains and pain VAS scores and HAQ-DI and FACIT-F demonstrate that the generic SF-36 measure of HRQOL offers sensitivity similar to the disease-specific instruments for detecting treatment-associated improvements. It also reflects the influence of disease and treatment-associated improvements in social and emotional functioning and mental health, which are not specifically assessed in other PRO.
A large proportion of individuals with PsA also have psoriasis, which adversely affects HRQOL, but to a different degree39,40,41. Patients with PsA report an effect of disease on physical functioning: PF and RP domains, and BP and VT domains, which also affect RE and SF domains. In contrast, psoriasis has a relatively greater effect on mental rather than physical domains, particularly RE and SF, with a lesser degree of effect on RP and BP domains9,24. In the current study population, 27% of patients had moderate to severe psoriasis at baseline. In a separate phase II RCT, apremilast was shown to be effective for treatment of moderate to severe plaque psoriasis, where 28.7% of patients treated with 20 mg BID and 40.9% with 30 mg BID achieved ≥ 75% reductions from baseline in Psoriasis Area and Severity Index scores24. At baseline, SF-36 domain scores between the PsA and psoriasis populations were similar in SF and MH domains, but 16 to 21 points lower in the 4 physical domains and 9 to 10 points lower in the VT and RE domains. Apremilast 30 mg BID was also shown to significantly improve PRO, including HRQOL at 16 weeks in a population with moderate to severe plaque psoriasis, with similar magnitudes of change across physical and mental domain scores and endpoint values that approximated or met age- and sex-matched norms in the PF, RP, GH, VT, and SF domains42.
Limitations
Data in this report include posthoc analyses based on results from predefined secondary PRO. Nonetheless, they were designed to better characterize treatment-associated changes with active therapy and have further validated the utility of a generic instrument assessing HRQOL in PsA (the SF-36). The short duration of this trial — 12 weeks — limits the results, but nonetheless supports dose-related findings. The influence of longer-term apremilast treatment on patients’ HRQOL will be assessed in ongoing, phase III trials that are expected to yield valuable information.
This trial used a rigorous design and provided strong evidence that apremilast is effective for the treatment of patients with active PsA25. As described in a separate report, adverse events were predominantly mild or moderate in severity and generally did not lead to treatment discontinuation25. Importantly, no opportunistic infections have been reported with use of apremilast. Based on these findings, the Psoriatic Arthritis Long-term Assessment of Clinical Efficacy (PALACE) phase III study program, which consists of four 52-week RCT, followed by longterm open-label extensions (2–5 years), will evaluate the efficacy and safety of apremilast in active PsA, including a higher apremilast dose (30 mg BID), as studied in psoriasis24.
Active PsA is associated with physical impairments and large decrements in patient-reported HRQOL. In our current study, apremilast 20 mg BID in patients with active PsA resulted in broad and statistically significant as well as clinically meaningful improvements in both disease-specific and generic measures of HRQOL and may become an important treatment option for this patient population.
Acknowledgment
The authors received editorial support in the preparation of this report from Peloton Advantage LLC, and Jennifer Schwinn, RPh.
Footnotes
-
Sponsored by Celgene Corporation.
- Accepted for publication February 4, 2013.








{kind=link}
{kind=link}