

Abstract
Objective. Data on when to stop use of biological agents in rheumatoid arthritis (RA) are scant. We assessed the length of remission and the rate of clinical relapse in patients with RA who had to discontinue treatment with tocilizumab (TCZ) because of the ending of longterm (5 yrs) open-label clinical trials.
Methods. All patients at 2 participating centers in Mexico were in remission, defined as Disease Activity Score 28 ≤ 2.6, with no swollen joints at the time of the last TCZ infusion. Patients were followed thereafter every 8 weeks for 12 months or until relapse. Relapse was defined as the presence of ≥ 1 swollen joint. Doses of methotrexate and antiinflammatory drugs were not changed during the followup period.
Results. Forty-five patients were analyzed, 87% were women (mean age 52 yrs, mean disease duration 14 yrs). During the 12 months of followup, 44% of patients maintained remission. Relapses occurred in 56% of patients: 14 during the first 3 months after the last TCZ administration. Retreatment using other agents achieved low disease activity or remission.
Conclusion. Longterm clinical remission is possible in a number of patients with RA after suspension of TCZ. This effect has also been reported with other biologic agents. Additional data are required to support recommendations for discontinuing a biological agent after achieving remission.
Rheumatoid arthritis (RA) produces a multidimensional effect ranging from pain, stiffness, progressive destruction of diarthrodial joints, and development of comorbid conditions such as cardiovascular disease or cancer to family distress and high societal costs1,2. Although the incidence of RA peaks during the fifth decade of life, it can affect individuals in all age groups. Indeed, in some countries, in almost half of patients with RA the disease begins before the age of 35 years3. Spontaneous remissions may occur in some patients but most have a chronic progressive course.
RA treatment has changed considerably during the last decade with the development and introduction into daily clinical practice of biological disease-modifying agents. When to initiate biological agents in the course of the disease has been an issue of much discussion4,5,6, yet according to the new American College of Rheumatology guidelines7, biologic agents are recommended for early and established RA with moderate to high disease activity and/or poor prognosis features (e.g., positive rheumatoid factor or anticitrullinated protein antibodies), thus increasing the proportion of patients who are candidates for their use.
Despite advances in the field of biological agents and algorithms to use them, data about when to stop such treatment are scant. Emerging data indicate that discontinuing the biologic agent is more likely to be possible after achieving and maintaining remission4,5,6,8,9,10,11,12,13,14,15,16,17,18,19; if confirmed, this possibility would have a remarkable influence medically and with regard to health economics. Disease activity outcomes after the ending of an industry-sponsored clinical trial may provide useful information to support the above concept.
We assessed the length of remission and the rate of clinical relapse in patients with RA who had to discontinue the interleukin 6 (IL-6) blocker tocilizumab (TCZ) because of the ending of longterm open-label clinical trials, at 2 participating centers in Mexico.
MATERIALS AND METHODS
Study design
This was a prospective cohort study of patients with RA assembled at the last TCZ infusion because of the ending of 2 open-label, industry-sponsored longterm extension trials.
Patients
All patients were enrolled first in 1 of 4 multinational, industry-sponsored randomized clinical trials of TCZ20,21,22,23 at 2 participating centers in Mexico; these patients then continued into 1 of the 2 open-label extension studies24,25 using methotrexate (MTX) and TCZ 8 mg/kg every 4 weeks for 5 years. The entry criterion was that at the last TCZ infusion (Week 260) all these patients be in remission, as defined by a 28-joint Disease Activity Score < 2.6 and the absence of swollen joints.
Procedures and followup
After the ending of the extension studies, patients no longer received TCZ but continued with MTX on the same dose as before. All patients returned to their referral clinic to continue with standard of care. Referral rheumatologists have different intervals between appointments and variability in joint count. Thus, to ascertain relapse and the time it occurred, patients were monitored at our clinics for 12 months as follows: (1) each patient had a structured telephone interview based on the COPCORD core questionnaire26 every 8 weeks by a senior medical student; (2) each patient was instructed to communicate with our centers without delay if they believed they had any swollen joint. In any case, if a patient reported a swelling joint or had the possibility of resurgence of RA, an appointment was made at our clinics no more than 1 week later; at that point physical examination and joint count were performed by the same rheumatologist (CRR, ASO, or JMT) as during the 5 years of the extension studies, using a similar template of 68 joints. (3) All patients were also assessed by the same rheumatologists, under the same procedures, at the end of the 12-month followup.
The primary outcome was relapse, defined as the time when the patient presented at least 1 swollen joint as assessed by a rheumatologist. Rates of relapses were calculated as the ratio of relapsed patients to the total number of patients in a given period of time. Length of remission was calculated by difference of time from last infusion to time of relapse. Data during the followup period were collected by senior medical students independent from the industry-sponsored clinical trials.
Statistics
Data are presented with means and 2-tailed SD. Differences between means were determined using nonparametric tests (Mann-Whitney U test or Kruskal-Wallis 1-way ANOVA). Cox’s proportional hazard model was used to explore potential predictor variables for relapse or length of remission. Significance was set at p ≤ 0.05 level.
All participating patients had provided signed informed consent for each clinical trial following protocols of the institutional ethics committees and regulatory agencies. All patients were informed in advance about the ending of the longterm extension studies, and all had agreed to be on a waiting list to try to find another biological treatment in case of relapse.
RESULTS
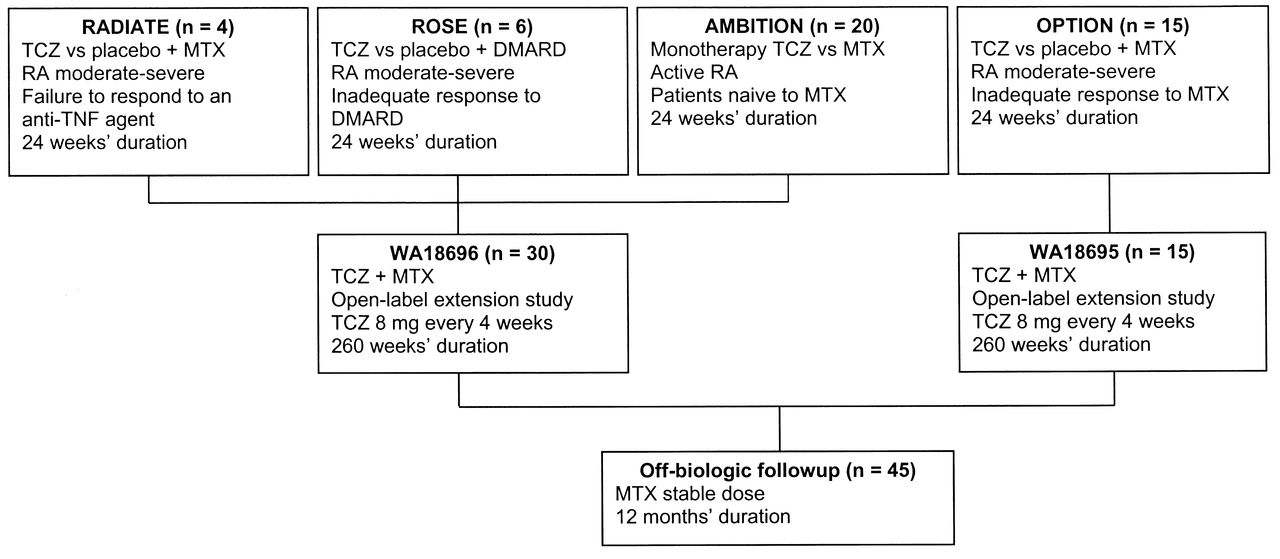
Forty-five patients participated in the study. Of these, 4 were first enrolled in the RADIATE trial because of failure to respond to an anti-tumor necrosis factor (TNF) agent20, 6 were enrolled in the ROSE trial because of inadequate response to traditional disease-modifying antirheumatic drugs (DMARD)21, 20 were enrolled in the AMBITION trial and were MTX-naive at the time of enrollment to assess TCZ monotherapy22, and 15 patients were enrolled in the OPTION trial because of inadequate response to MTX23. After these trials that lasted 6 months, patients continued in the open-label extension trials24,25 (Figure 1). All patients were receiving MTX, including those enrolled first in the AMBITION trial, at the same dose for the entire time of the open-label extension trials and during the followup. Those who participated in the open-label extension trials were also in remission at least for the last 4 years and at the time of the last TCZ infusion. Table 1 shows demographic and clinical characteristics of the 45 patients at the last TCZ infusion.
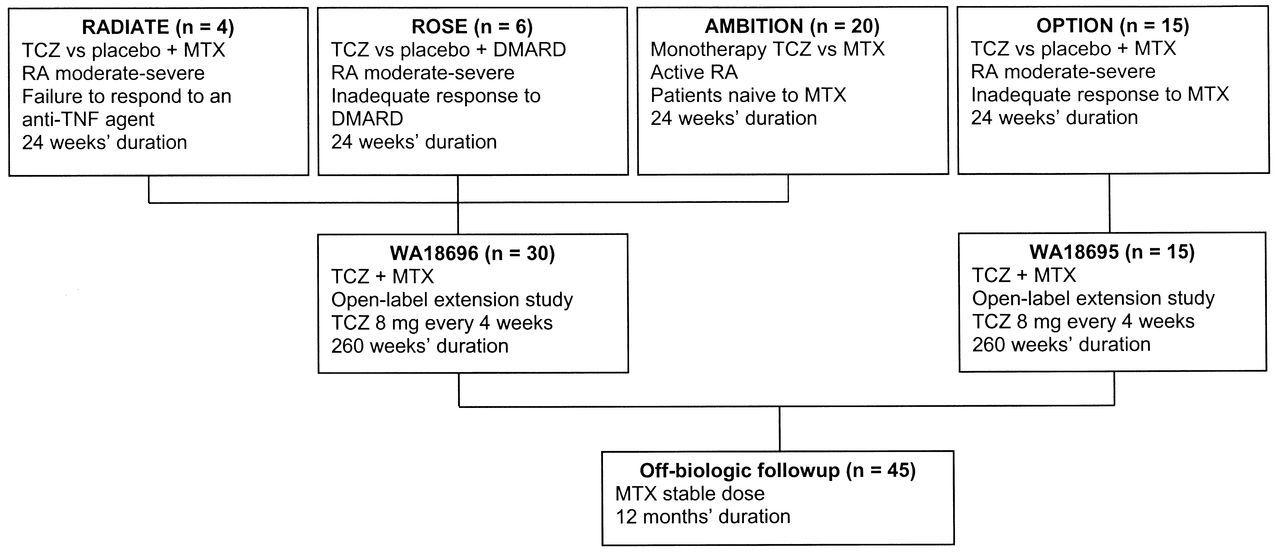
Core clinical trials where patients were first enrolled. TCZ: tocilizumab; MTX: methotrexate; RA: rheumatoid arthritis; TNF: tumor necrosis factor; DMARD: disease-modifying antirheumatic drug.
Demographic and clinical characteristics of the 45 studied patients at the last tocilizumab infusion.
Table 2 shows a frequency distribution of relapses. Twenty patients (45%) maintained clinical remission at 12 months after last TCZ infusion: 9 (45%) of 20 patients from the AMBITION study, 7 (46.6%) of 15 patients from the OPTION study, 1 (25%) of 4 patients from the RADIATE study, and 3 (50%) from the ROSE study. Relapses occurred in 25 patients; patients from the AMBITION study relapsed steadily during the year of followup after last TCZ infusion; patients from the OPTION and RADIATE trials relapsed mostly during the first trimester; and patients from the ROSE trial relapsed during the first and second trimester.
Frequency distribution of relapses and retreatment after relapses of the 45 patients.
We did not identify predictor variables for relapse or length of remission, including disease duration at entry to the core trials, age, or sex, using Cox’s proportional hazard model.
Patients who relapsed were treated further based on their healthcare resources and preferences. The 25 patients who relapsed continued with MTX, but it was increased in 9 patients. A second DMARD was indicated in 5 other patients; glucocorticoids were added in 3, anti-TNF agents were prescribed in 4, rituximab was used in 3, and TCZ was restarted in another 4 patients. All patients achieved a low disease activity status or remission.
DISCUSSION
Achieving remission to maintain functional ability and prevent joint damage is the treatment goal in RA. The clinical outlook has changed considerably with the use of biological disease-modifying agents. However, these agents are not exempt from short- and longterm risks and have a high cost, and the longterm effects of suppressing a particular immunological signal remain unknown. If they are not essential to maintain suppression of rheumatoid inflammation, it would be beneficial if such therapies could be discontinued once the initial treatment goal had been achieved. This possibility would have notable effects in patient safety and health economics.
Our study shows that it is possible to maintain longterm clinical remission after withdrawal of the IL-6 blocker TCZ; 20 out of 45 patients maintained clinical remission at 12 months, and relapses, using a stringent criterion, occurred mostly during the first 5 months after the last TCZ infusion. However, our study should be viewed as a proof of concept, because several limitations must be considered. We studied a small convenience sample of patients in remission from 2 participating centers. Patients were enrolled in different core trials, with heterogeneous criteria, e.g., some were naive to MTX, others were enrolled because of failure of an anti-TNF agent, etc. The study design precludes proper calculations about predictors of relapse or the length of remission, and effect size.
However, it is possible that factors such as shorter disease duration5, negative rheumatoid factor, male sex, longer duration of biological treatment17, rapid achievement of remission, nonsmoking, absence of HLA shared epitope9, or initial treatment with biologicals rather than delayed treatment6 may be independent predictors of successful discontinuation of biological agents.
Although our definition of relapse was stringent and based on clinical grounds, the effect on the progression of structural damage was not assessed.
Our results are in accord with those of other investigations and it seems that this phenomenon is not specific to a given biological agent, as per similar reports with other agents, such as abatacept18, adalimumab5,12,14,17,19, infliximab5,8,9,10,16,17, and etanercept5,17. Maintaining remission after discontinuation of these agents was highly variable — it has been described in 0 to 97% of patients, in studies with different patient populations, diverse outcome definitions, and followup durations between 12 weeks and over 7 years. In patients who had a disease flare, retreatment with these agents was successful in 70% to 100%. There is only 1 previous report of 4 patients who relapsed after withdrawal of TCZ and who improved after retreatment with this agent27. In our patients who relapsed, retreatment strategies achieved either remission or low disease activity.
We agree with the position stated by van den Broek, et al6 about a research agenda to support guidelines for stopping biological therapies in patients with RA. The concept that longterm remissions may happen in a proportion of patients after stopping several biologic agents has been proved. It is obvious that relapses can happen, but it may be acceptable to aim at a temporary drug “holiday” rather than permanent drug-free remission. Further research should focus on predictors of remission and relapse (e.g., shorter disease duration, duration of remission before discontinuation of the biologic therapy), definitions of how to detect relapses at very early stages, strategies for early restart of biological treatment, influence on structural damage, and the efficacy of retreatment.
- Accepted for publication March 12, 2013.








{kind=link}