

Abstract
Objective. To examine the efficacy and safety of antibiotic treatments for reactive arthritis (ReA).
Methods. We did a systematic review and metaanalysis of randomized controlled trials of antibiotics for treatment of ReA. We searched electronic databases and conference proceedings up to November 2011. Included trials reported on remission, joint counts, and pain or patient global scores in any language.
Results. Twelve trials were eligible for inclusion and 10 provided data for metaanalysis. The pooled relative risk of failure to achieve remission from a random effects model showed no significant benefit of antibiotic treatment on remission (7 trials, 375 participants, RR 0.74, 95% CI 0.49–1.10); however, substantial heterogeneity was observed (I2 = 76.3%, p < 0.0001). The treatment effect did not differ significantly by the type of organism triggering the ReA (chlamydia, 4 trials, RR 0.80, 95% CI 0.63–1.03, vs other microorganisms, 5 trials, RR 0.72, 95% CI 0.29–1.79, metaregression p = 0.477) or use of combination antibiotics (monotherapy, 6 trials, RR 0.70, 95% CI 0.39–1.26, vs combination therapy, 1 trial, RR 0.79, 95% CI 0.63–0.99, metaregression p = 0.466). When unblinded trials were excluded, the treatment effect was attenuated and heterogeneity decreased (RR 0.87, 95% CI 0.70–1.10, I2 = 32.8%, p = 0.19). No significant effects of antibiotic treatment were observed on joint counts, pain, or patient global scores; however, antibiotics were associated with a 97% increase in gastrointestinal adverse events.
Conclusion. Trials of antibiotic treatment for ReA have produced heterogeneous results that may be related to differences in study design. The efficacy of antibiotics is uncertain.
Reactive arthritis (ReA) is an inflammatory arthritis that typically occurs 2–4 weeks following an extraarticular infection1, most commonly with Chlamydia, Salmonella, Shigella, Campylobacter, and Yersinia species2. Chronic ReA is commonly defined as arthritis lasting > 6 months1,3; however, about 5%–20% of individuals with ReA remain symptomatic for > 1 year3, and interventions to achieve early remission are of interest.
ReA has traditionally been thought of as a “sterile” arthritis because cultures of joint fluids yield no growth of organisms. However, recent evidence suggests that Chlamydia species can become persistent in joint and synovial tissue4, and immunocytochemical staining has demonstrated the presence of persistent bacterial antigens, further implicating the role of microorganisms in the inflammatory process5,6. These findings provide a biological rationale for the use of antibiotic treatment for ReA and have renewed interest in this therapeutic approach.
There is no gold standard treatment for ReA; however, commonly used treatments include nonsteroidal antiinflammatory drugs (NSAID) and intraarticular corticosteroids. Although antibiotics have also been used for treatment of ReA, the efficacy of this approach has been unclear, and current recommendations remain conflicting7,8,9. Some proposed reasons for the discrepant results are differences in antibiotic regimens, duration of treatment, and the nature of the inducing microorganism (Chlamydia vs enteric pathogens). Further, existing trials have been small, with limited power to detect differences in clinical outcomes. Given these limitations, we conducted a systematic review and metaanalysis of randomized controlled trials (RCT) evaluating antibiotics for treatment of ReA. We also sought to evaluate whether the type of inciting microorganism, use of combination antibiotics, or trial quality could result in heterogeneous results between trials.
MATERIALS AND METHODS
Data sources and searches
We performed this study according to a prespecified protocol and following the Preferred Reporting Items for Systematic review and Meta-Analyses (PRISMA) statement10. Two reviewers (CB, JK) searched Medline (1950 to November 17, 2011), PubMed (1966 to November 17, 2011), Embase (1980 to November 17, 2011), and the Cochrane Central Register of Controlled Trials (1966 to November 17, 2011) using both MeSH terms and keywords pertaining to 2 major themes: ReA and antibiotic therapy (complete search strategy available from the author on request). Filters to retrieve RCT were applied when appropriate11. In addition, proceedings from 2 major scientific conferences (the American College of Rheumatology Annual Scientific Meeting and the Interscience Conference on Antimicrobial Agents and Chemotherapy) in the past 2 years were reviewed to identify relevant trials that might not have been published. Experts were also contacted to identify any ongoing or unpublished work.
Study selection
Trials were eligible for inclusion if the following criteria were met: a prospective RCT that included patients with ReA and used antibiotic treatment as the main intervention compared with placebo or no antibiotic treatment. Trials had to report data on at least 1 of 5 clinical outcomes of interest: clinical remission, swollen or tender joint counts, pain score, or patient global assessment score. Publications in all languages were included. Two reviewers independently performed the initial abstract screening and then completed a full-text review of relevant articles to confirm eligibility. The κ statistic was calculated for each step to assess agreement between reviewers and any disagreement was resolved by consensus. Trials that reported any clinical outcome were included in the systematic review, while only those reporting on prespecified outcomes with adequate data for pooling were included in the metaanalysis.
Data extraction and quality assessment
Two reviewers independently extracted the data from the primary trials using a standardized form. Primary authors were contacted to obtain further information if there was inadequate information in the article. When not otherwise available, numeric data were derived from measurements of graphical presentation of data. Outcomes included failure to achieve remission as defined by each trial, number of swollen or tender joints (a Ritchie articular index12 was accepted for the latter when reported), pain on a visual analog scale (VAS; articular pain at movement was taken if more than 1 pain type was reported), and a patient global assessment on a VAS. Adverse events were recorded as any adverse event (as defined by each trial) and gastrointestinal adverse events. The methodological quality of the trials was assessed according to the Cochrane Collaboration’s tool for assessing risk of bias in randomized trials13. If insufficient detail was reported of what happened in the trial, we judged trials as having unclear risk of bias. We considered blinding of both participants and outcome assessors to be present if “double-blinding” was reported in the article. Lastly, data were collected on clinical factors that could contribute to study heterogeneity, including by inciting organism (Chlamydia-induced vs other) and antibiotic strategy used (combination vs monotherapy). We defined combination therapy as the use of 2 or more agents from different antibiotic classes and therefore we categorized amoxicillin-clavulanate and trimethoprim-sulfamethoxazole as monotherapies.
Data synthesis and analysis
For binary outcomes (failure to achieve remission and adverse events), we pooled the relative risks obtained for each study using the random effects model of DerSimonian and Laird14. We also pooled the mean differences between treatment groups using random effects models for outcomes measured on continuous scales. We used means and SD measured at the end of study followup when reported, or the mean (SD) change in these measures for each treatment group over the followup period where end of study values were not reported15. SD were derived directly from 95% CI where necessary15. We pooled weighted mean differences (WMD) if the outcome was reported using a uniform scale across trials (swollen joint count), and the standardized mean difference (SMD) if trials reported the outcome using different scales (tender joint count, pain score, and global assessment). We assessed heterogeneity using Cochrane’s Q statistic and the I2 statistic, which quantifies the proportion of variability attributed to between-study heterogeneity16. Results were presented graphically using forest plots for each outcome.
Potential sources of heterogeneity were investigated using stratified analyses and metaregression. We examined the relationship between treatment effect and the following covariates: type of implicated pathogen (Chlamydia vs other); type of antibiotic treatment (monotherapy vs combination therapy); and risk of bias13. We also performed an influence analysis whereby the influence of each trial on pooled results was estimated by deleting each in turn for the analysis and noting the degree to which size and significance of the treatment effect and the I2 statistic changed11. We evaluated publication bias using funnel plots and Begg’s test for asymmetry. Stata version 12 was used for all analyses employing the metan, metareg, metabias, metafunnel, and metainf commands.
RESULTS
Study selection
Our search of electronic databases yielded a total of 249 unique citations (Figure 1). After abstract screening, 225 citations were excluded because they did not meet inclusion criteria. A total of 12 trials were included in our systematic review7,8,9,17,18,19,20,21,22,23,24,25.

The selection of studies for review. RCT: randomized controlled trial.
Study characteristics
The trial populations were clinically heterogeneous with varying definitions of ReA (Table 1). Three trials also included patients who had other diagnoses including uveitis24, “seronegative arthritis”22, and “undifferentiated oligoarthritis”21, and for these trials we included only the results of the subset of patients with ReA. All trials except one17 were conducted in adult populations. Of the trials included in the metaanalysis, 2 limited eligibility to patients with Chlamydia-induced ReA7,8 and 2 stratified results based on this subtype20,21. Only one trial7 reported enrollment of subjects with chronic ReA (duration ≥ 6 mo). The mean duration of symptoms prior to inclusion varied considerably between trials (range < 4 weeks to ≥ 6 mo).
Characteristics of the study population, intervention, and duration of followup of antibiotic treatment for reactive arthritis.
A variety of antibiotic regimens were studied; however, only one trial examined combination antibiotic therapy7 (Table 1). The duration of treatment also varied (range 14 days to 12 mo). Seven trials permitted the use of NSAID during the study. Only one trial7 permitted the use of disease-modifying antirheumatic drugs (DMARD) if the study participants were taking stable doses at 12 weeks prior to study entry. Additional characteristics of trials are reported in Appendix 1.
Study quality
Study quality is shown in Figure 2. There was a high risk of selection bias: only 4 trials adequately reported the method of randomization and only 3 trials adequately described allocation concealment. There was also a high risk of performance bias in 2 trials because there was no placebo. In 9 trials there was an unclear risk of detection bias because there was no description of blinding of the outcome assessment. Most trials had more than 10% of participants lost to followup and were therefore at risk of attrition bias. Eight trials were at high risk of reporting bias because of selective reporting, i.e., they did not specify adverse events a priori or had poorly defined outcome measures. Three studies had significant baseline differences between treatment groups and are recorded in “other bias” (Figure 2).
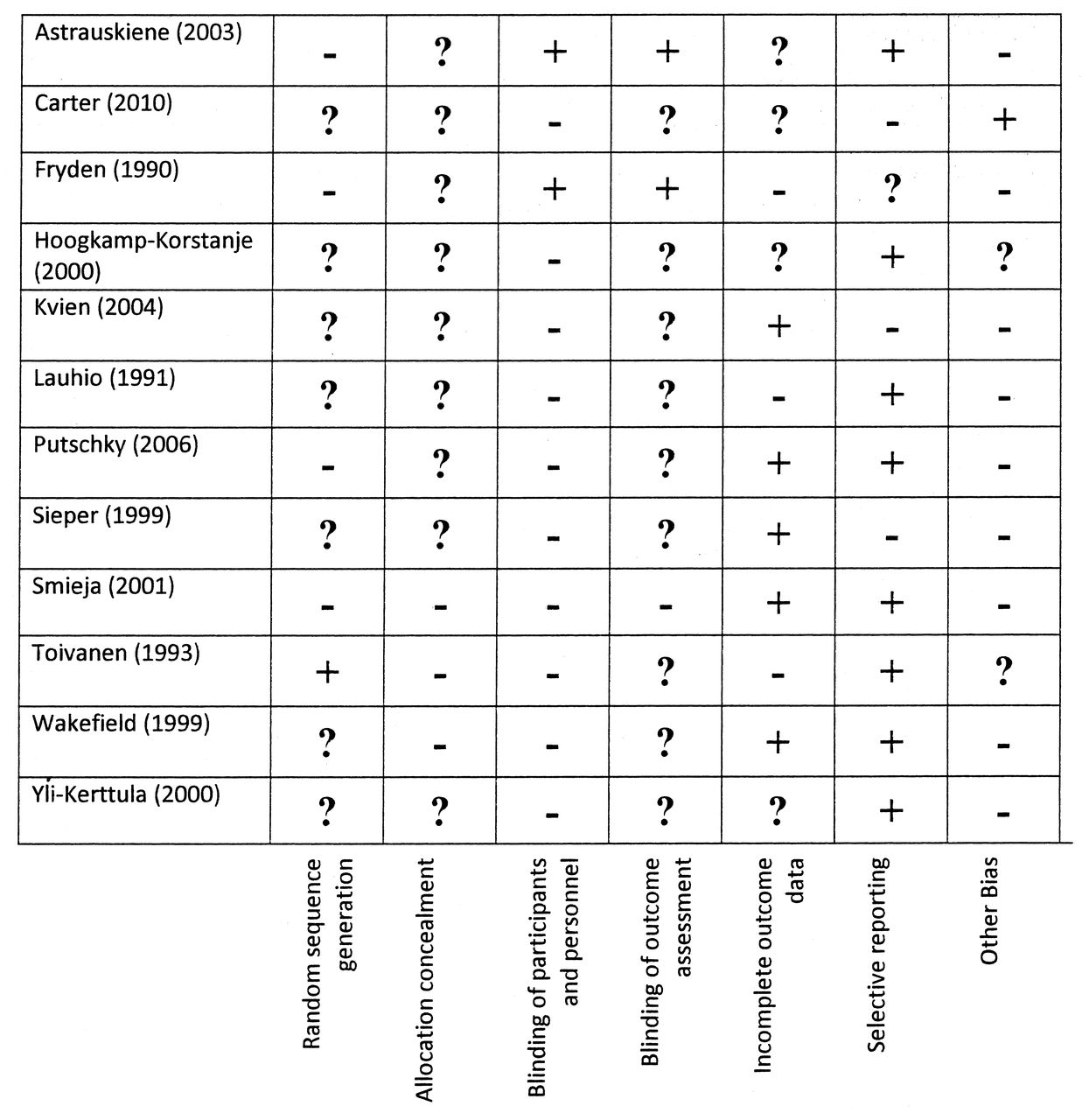
Quality assessment of trials included in the metaanalysis of antibiotic treatment for reactive arthritis. “+” denotes features at high risk of bias; “–” denotes feature at low risk of bias; “?” denotes features at uncertain risk of bias. As described in Higgins, et al13, selection bias may be due to inadequate random sequence generation or allocation concealment; performance bias is due to inadequate blinding of participants or personnel; detection bias is due to improper blinding of outcome assessment; attrition bias is related to incomplete outcome data; reporting bias is due to selective reporting. “Other bias” refers to possible bias due to important baseline differences between groups.
Remission of ReA
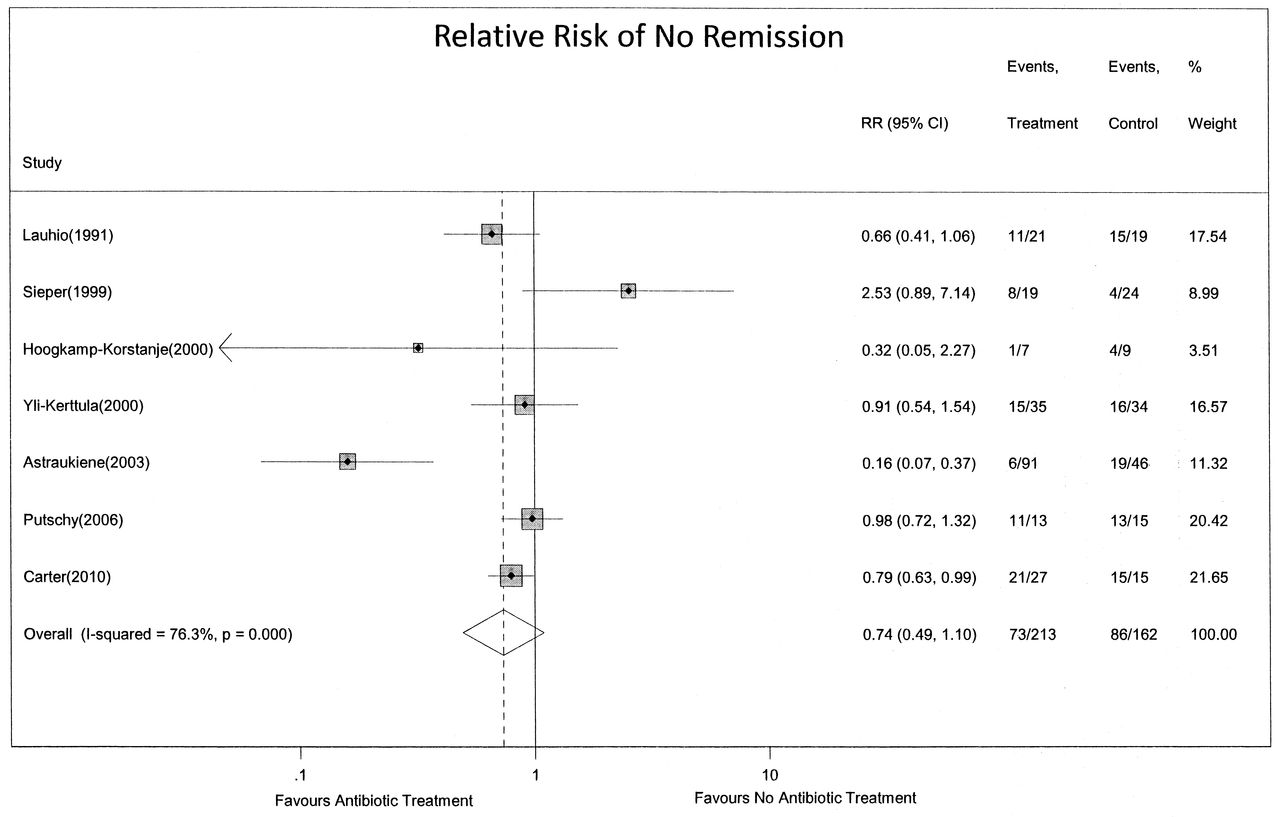
Based on results from 7 trials, including a total of 375 participants, antibiotic treatment had no significant effect on remission of ReA (pooled relative risk of failure to achieve remission 0.74, 95% CI 0.49–1.10; Figure 3). However, there was significant heterogeneity between trials (I2 = 76.3%, Q statistic p < 0.0001).
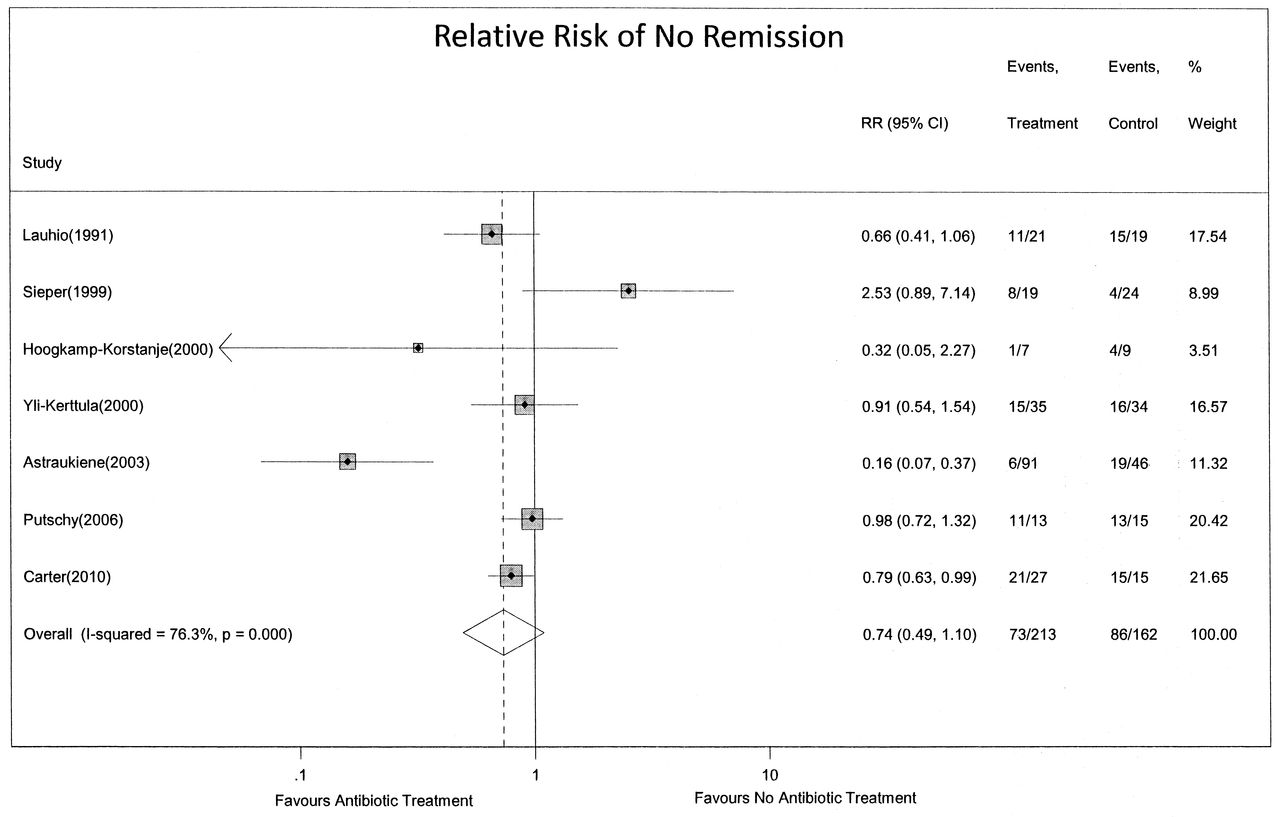
Relative risk of failure to achieve remission of reactive arthritis with antibiotic therapy using a random effects model.
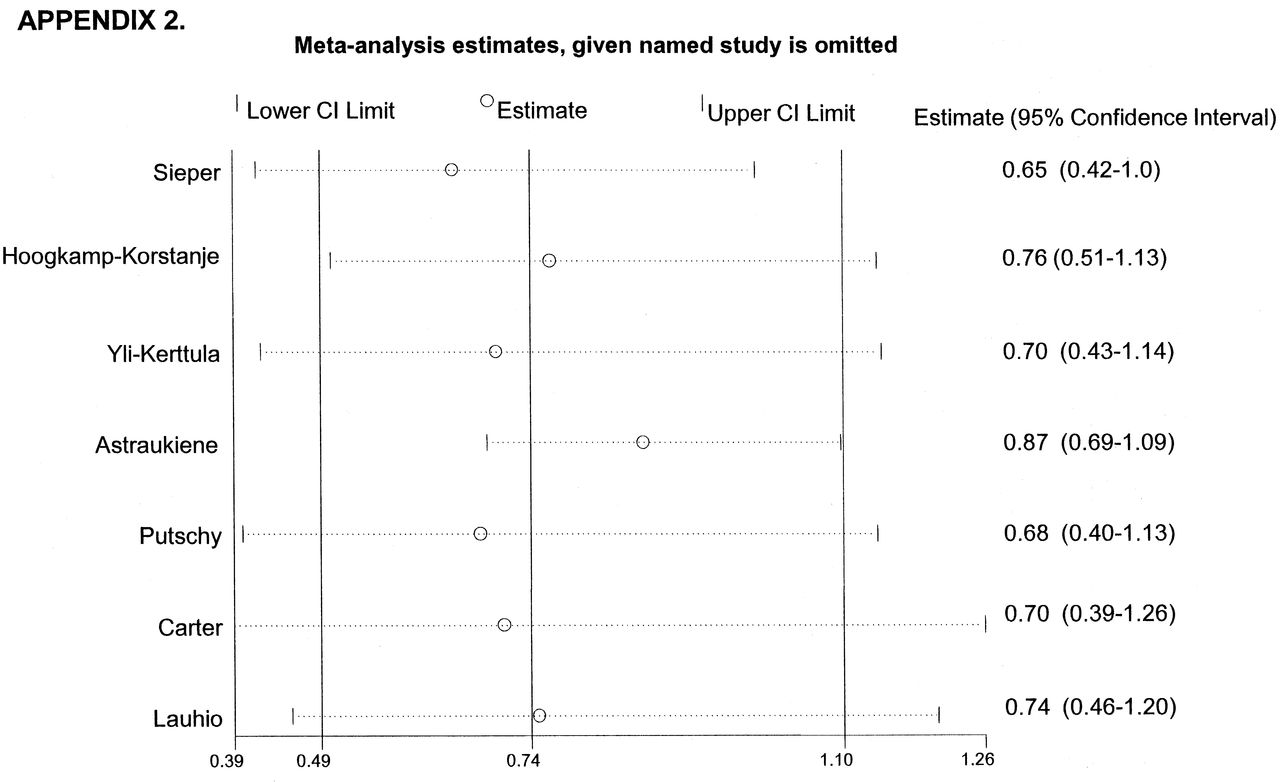
The results of stratified analyses and metaregression to explore reasons for heterogeneity are shown in Table 2. There was no significant difference in the effect of antibiotic treatment on remission according to the pathogen implicated (Chlamydia, 4 trials, 101 subjects, RR 0.80, 95% CI 0.63–1.03, vs other microorganisms, 5 trials, 274 subjects, RR 0.72, 95% CI 0.29–1.79, metaregression p = 0.477). Similarly, pooled results did not differ significantly according to whether the trial used antibiotic monotherapy or combination therapy (monotherapy, 6 trials, 333 subjects, RR 0.70, 95% CI 0.39–1.26, vs combination therapy, 1 trial, 42 subjects, RR 0.79, 95% CI 0.63–0.99, metaregression p = 0.466). Five trials were at uncertain risk of selection bias because of inadequate reporting of random sequence generation7,19,20,21,25; however, treatment effects were not significantly different from trials without risk of selection bias (metaregression p = 0.408). One trial by Astrauskiene17 was at risk for performance bias because it was not blinded. Although there was no statistically significant difference in the treatment effect between the unblinded and blinded trials (metaregression p = 0.137), heterogeneity decreased significantly in the strata of blinded trials (I2 = 32.8%), and the treatment effect was substantially attenuated (RR of failure to achieve remission 0.87; 95% CI 0.70, 1.10), compared to that observed in the unblinded trial (RR of failure to achieve remission 0.16; 95% CI 0.07, 0.37). The effect of this trial on the pooled results was further demonstrated in an influence analysis (Appendix 2), where the most substantial change in the point estimate of the treatment effect was identified with omission of the trial by Astrauskiene17.
Stratified analysis of antibiotic treatment and risk of failure to achieve remission of reactive arthritis.
Risk of attrition bias was high or uncertain in 6 trials (Figure 2); however, treatment effects were not significantly different from trials without risk of attrition bias (metaregression p = 0.767). Similarly, selective reporting was deemed to be of high risk in 5 trials; treatment effects did not differ significantly in trials of low risk of selective reporting (p = 0.315). Baseline differences between treatment groups was seen to varying degrees in 3 trials and no differences in treatment effect were observed based upon this feature (metaregression p = 0.397).
Joint findings, pain, and patient global assessment
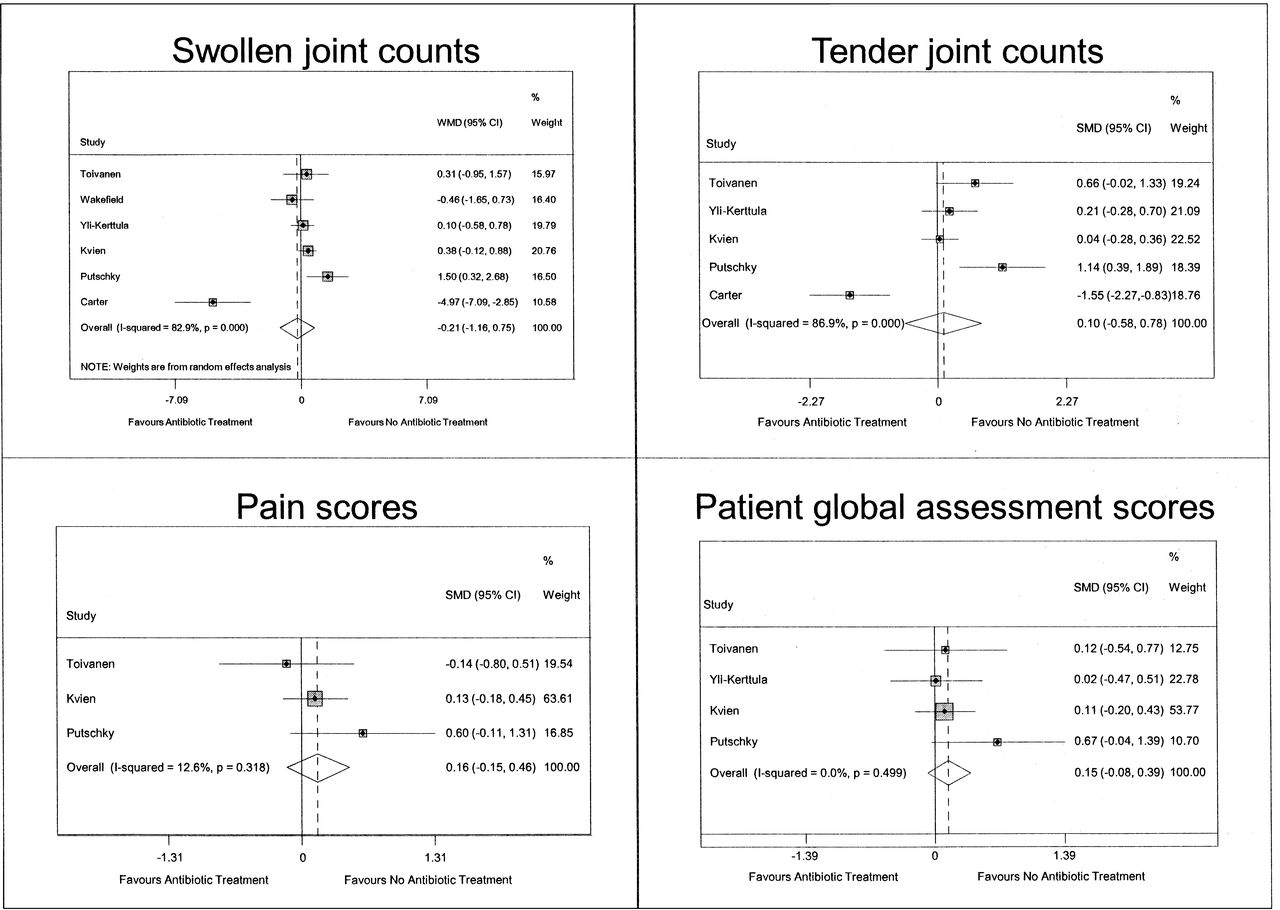
Based on results from 6 trials including 375 participants (Figure 4), there were no clinically or statistically significant effects of antibiotic treatment on the number of swollen joints (WMD −0.21, 95% CI 1.16–0.75). However, there was considerable statistical heterogeneity between the trials (I2 = 82.9%, Q statistic p < 0.0001; Figure 4). Neither the type of inciting organism (Chlamydia-induced vs other) nor risk of selection bias because of inadequate random sequence generation was associated with differences in the treatment effect (Appendix 3). The effect of antibiotics on swollen joint counts also did not differ between trials at high versus low risk of attrition bias or reporting bias (Appendix 3).
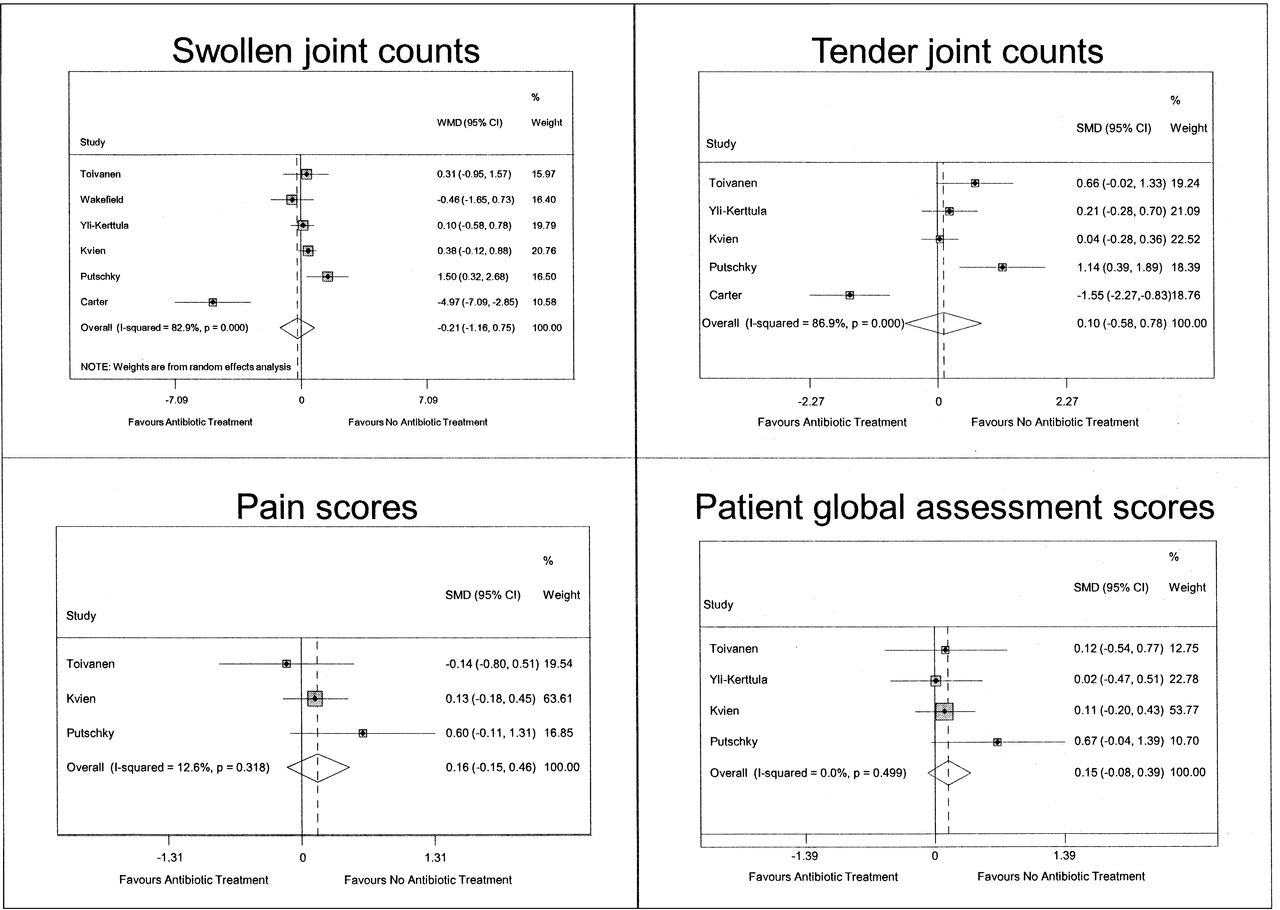
Effects of antibiotic therapy for reactive arthritis on additional outcomes using random effects analyses: weighted mean difference of swollen joint counts (top left); standardized mean difference (SMD) of tender joint counts (top right); SMD of pain scores (bottom left); SMD of patient global assessment scores (bottom right). Dots represent point estimates, lines represent 95% CI, and shaded boxes represent the percentage of weight contributed by each study. Open diamonds represent pooled results and are centered on the pooled point estimate, with length representing the pooled 95% CI.
There were no significant effects of antibiotic treatment on the number of tender joints (5 trials, 326 participants, SMD 0.10, 95% CI −0.58 to 0.78, I2 = 86.9%, p < 0.0001), pain (3 trials, 220 participants, SMD 0.16, 95% CI −0.15 to 0.46, I2 = 12.6%, p = 0.381), or patient global assessment of disease activity (4 trials, 284 participants, SMD 0.15, 95% CI −0.08 to 0.39, I2 = 0.0%, p = 0.499; Figure 4).
Adverse events
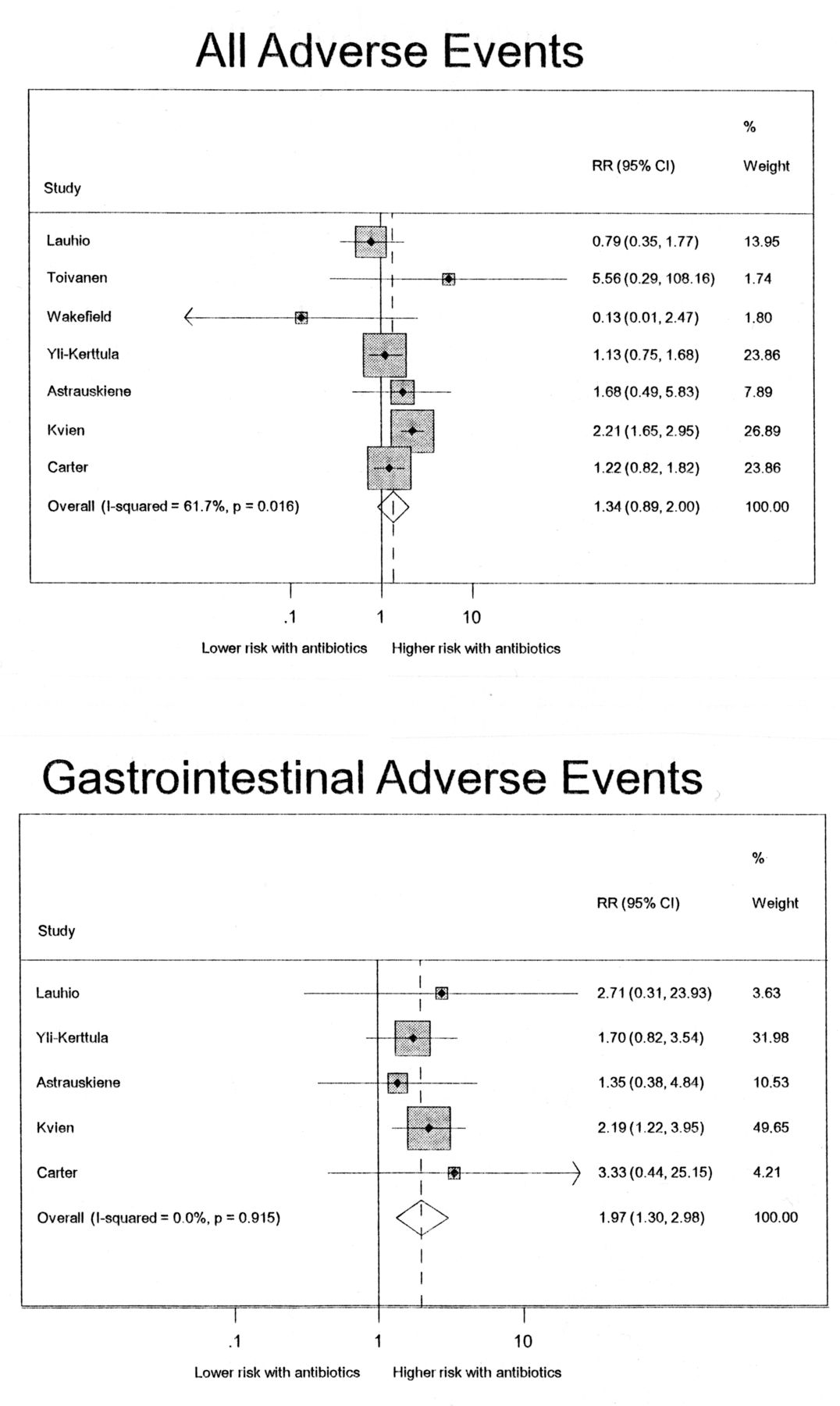
Adverse events were defined variably between the trials. Pooled results from 7 trials, including 534 participants, showed a nonsignificant increase in risk of any adverse event with antibiotic treatment (pooled RR 1.34, 95% CI 0.89–2.0); however, there was heterogeneity between trials (I2 = 61.7%, p = 0.016; Appendix 4). Five trials, which included 442 participants, reported gastrointestinal adverse events, with an almost 2-fold higher risk with antibiotic treatment (pooled RR 1.97, 95% CI 1.30–2.98), without heterogeneity in this effect (I2 = 0%, Q statistic p = 0.915; Appendix 4).
Publication bias
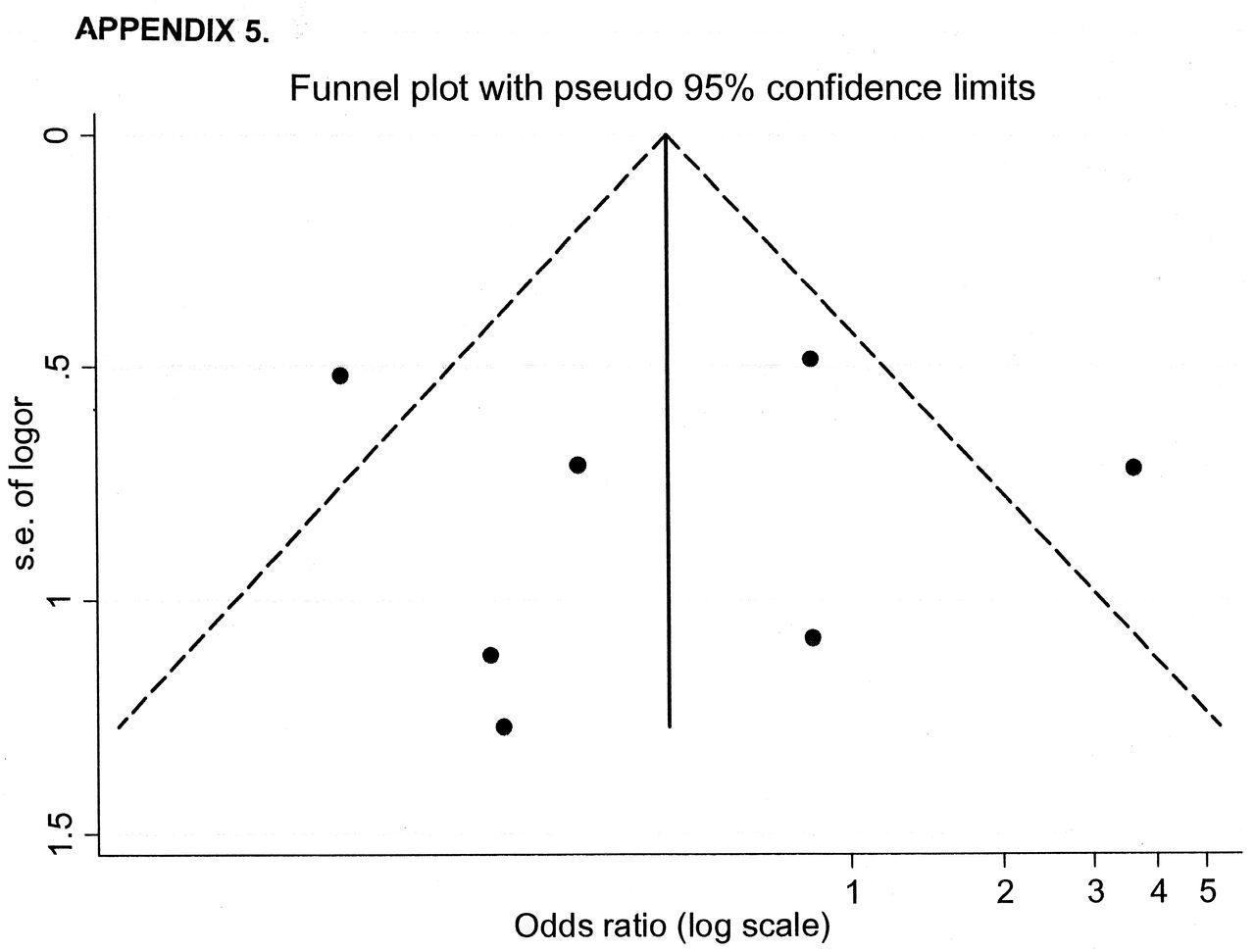
The funnel plot for failure to achieve remission of ReA showed no asymmetry suggestive of small study effects. Lack of publication bias was further supported by Begg’s test (p = 0.881; Appendix 5).
DISCUSSION
In this systematic review, we identified 12 trials of antibiotics for the treatment of ReA. Although trials varied in study populations, antibiotic regimen, and outcomes reported, data on clinical remission were identified from 7 trials with 375 patients. In pooled analyses, antibiotic treatment did not significantly reduce the risk of failure to achieve remission, although there was heterogeneity in this effect. Further analyses did not demonstrate clinically or statistically significant benefits to antibiotic treatment on joint counts, pain, or patient global scores, and suggested that antibiotic treatment may have adverse side effects.
The majority of trials identified by our systematic review failed to show an effect of antibiotics on remission. The exceptions were 2 trials7,17, which may in part explain the heterogeneity observed. One of those trials was conducted in a pediatric population17, a factor that substantially influenced the pooled results. Notably, this study was not blinded, and when excluded, the treatment effect further approached the null and heterogeneity was substantially reduced. This finding suggests that performance or detection bias may have contributed to its discrepant result and may explain much of the heterogeneity observed. Pooled analyses of trials at low risk for these forms of bias showed no significant effect of antibiotic treatment on remission.
Some experts propose that Chlamydia-induced ReA may be uniquely responsive to antibiotic treatment because it is mediated by chronic infection, citing biological evidence that Chlamydia may adopt a persistent phenotype in synovial tissue, while only bacterial fragments of other enteric pathogens have been demonstrated in joints4. We were not able to identify differences in the treatment effect based on pathogen type, although our ability to detect such a difference was limited, because not all trials stratified or restricted cohorts based on the inciting microorganism. Among the trials included in the metaanalysis, only those by Carter, et al7 and Putschky, et al8 were restricted to Chlamydia-induced ReA. Their conclusions differed, with Carter, et al7 reporting improved outcomes after prolonged antibiotic treatment and Putschky, et al8 reporting no benefit to treatment. The Carter study7 was unique in that it examined longterm combination therapy antibiotics in chronic ReA and patients were permitted to take DMARD if they were taking stable doses prior to randomization. Also, although the study was reported to be blinded, the use of rifampin, which can cause discoloration of bodily fluids, may have revealed treatment assignment.
The type and duration of antibiotic therapy have also been suggested as potential contributors to differences in treatment efficacy because of varying antimicrobial effects. Further, some antibiotics (including tetracycline26 and macrolides27) may have antiinflammatory effects independent of their antimicrobial activity28. Indeed, tetracycline treatment is effective in improving disease activity in rheumatoid arthritis29. Only 1 trial7 examined the use of combination therapies, which have the broadest potential for antimicrobial and antiinflammatory effects. In that trial, Carter, et al reported significant improvement in remission and joint counts with regimens containing rifampin in addition to either doxycycline or azithromycin, although metaregression did not identify significant differences in the treatment effect between that trial and trials examining antibiotic monotherapy.
Heterogeneous results were also observed for the effect of antibiotic treatment on swollen or tender joint counts, largely as a result of the greater efficacy reported in the trial of combination antibiotics7. This heterogeneity could not be explained by the inciting organism, and it remains uncertain whether other aspects of the study design, study population, or combination antibiotic regimen could have accounted for these differences.
There are caveats to interpreting the results of this meta-analysis. Trial design varied substantially, including the definitions and chronicity of ReA, the outcomes reported, and the antibiotic agents and duration of treatment administered, all of which may have contributed to statistical heterogeneity and limited the interpretation of the pooled result. Further, given the limited number of trials, with small sample sizes, metaregression had low power to identify features of heterogeneity. Lastly, many trials were at risk of bias.
Although the results of our study do not demonstrate efficacy of antibiotics for the treatment of ReA, this does not exclude the possibility that in subgroups of patients, or with specific treatment approaches, antibiotics may be effective. Given our findings, the use of antibiotics for treatment of ReA should at present remain restricted to clinical trials designed to resolve this uncertainty. The findings from the one trial of combination antibiotic therapy7, including a macrolide or a tetracycline and rifampin, suggest that this might be the antibiotic strategy most warranting future evaluation in larger trials for chronic ReA. Such future trials should ensure adequate allocation concealment, strategies to minimize losses to followup, appropriate blinding, and standardized use of cointerventions including DMARD, steroids, and NSAID to reduce the risk of bias.
In this systematic review and metaanalysis we observed heterogeneous effects of antibiotic treatment for ReA. These findings suggest that the efficacy of antibiotics for treatment of ReA remains uncertain, and that their use for this condition requires further evaluation in larger, well designed clinical trials.
Acknowledgment
The authors thank Dr. W. Ghali, D. Lorenzetti, and P. Ronskley for reviewing the manuscript. Additionally, the authors thank Drs. J.D. Carter and T. Yli-Kerttula for providing additional study information.
APPENDIX 1
Definitions of outcomes and adverse events reported in trials of antibiotic treatment for reactive arthritis.
APPENDIX 3
Stratified analysis of antibiotic treatment and swollen joint counts in reactive arthritis trials.
APPENDIX 4

Comparison of all adverse events and gastrointestinal adverse events between studies. Dots represent point estimates, lines represent 95% CI, and shaded boxes represent the percentage of weight contributed by each study. Open diamonds represent pooled results and are centered on the pooled point estimate, with length representing the pooled 95% CI.

Footnotes
-
Dr. Barber is funded by the UCB-CRA-TAS Post-Graduate Rheumatology Fellowship and Alberta Innovates Health Solutions Clinical Fellowship. Dr. James is supported by an alternative funding plan from the Government of Alberta and the University of Calgary.
- Accepted for publication January 30, 2013.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}