

Article Figures & Data
Figures
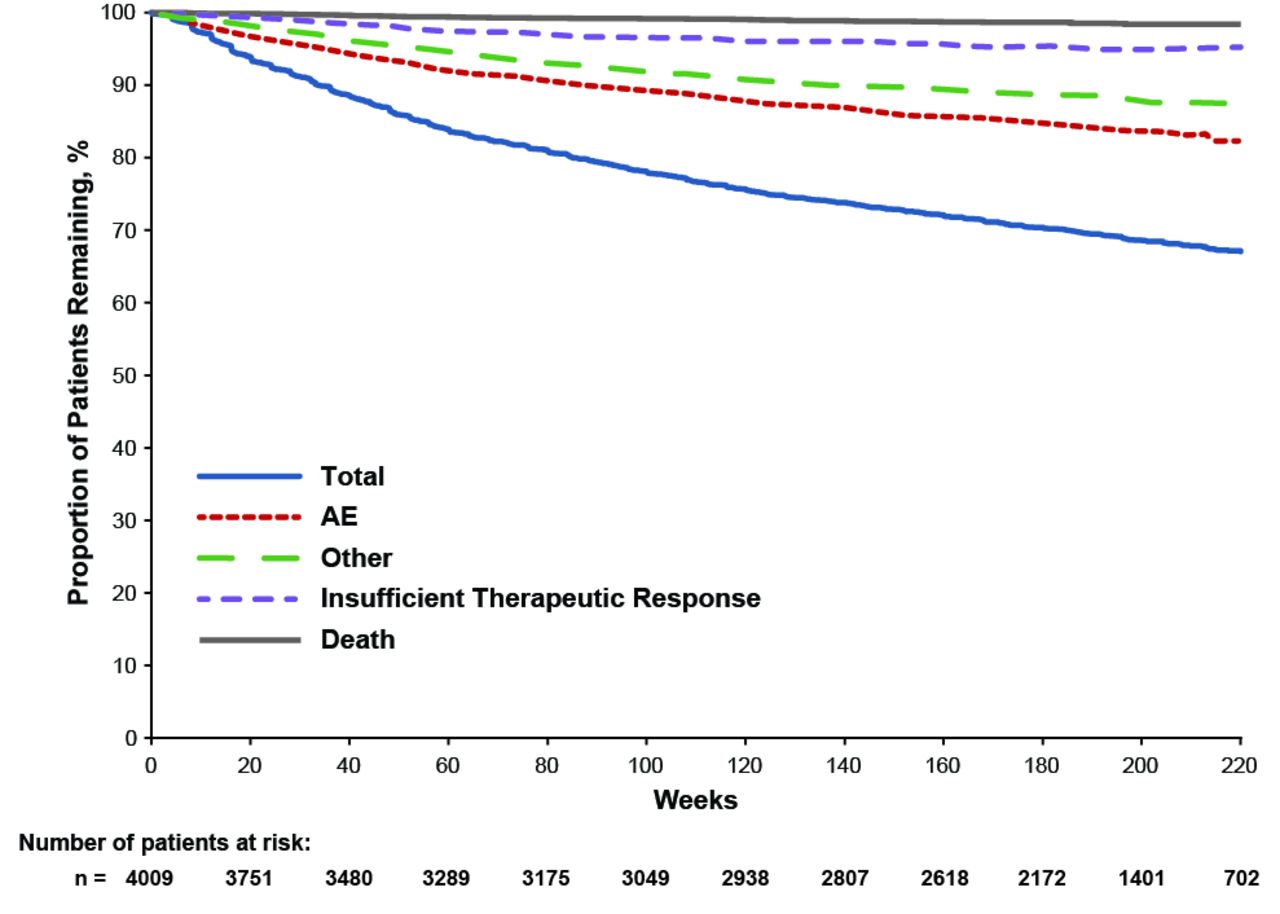
- Figure 1.
Kaplan-Meier plot of patient withdrawal by withdrawal reason (all-exposure population). AE: adverse event.
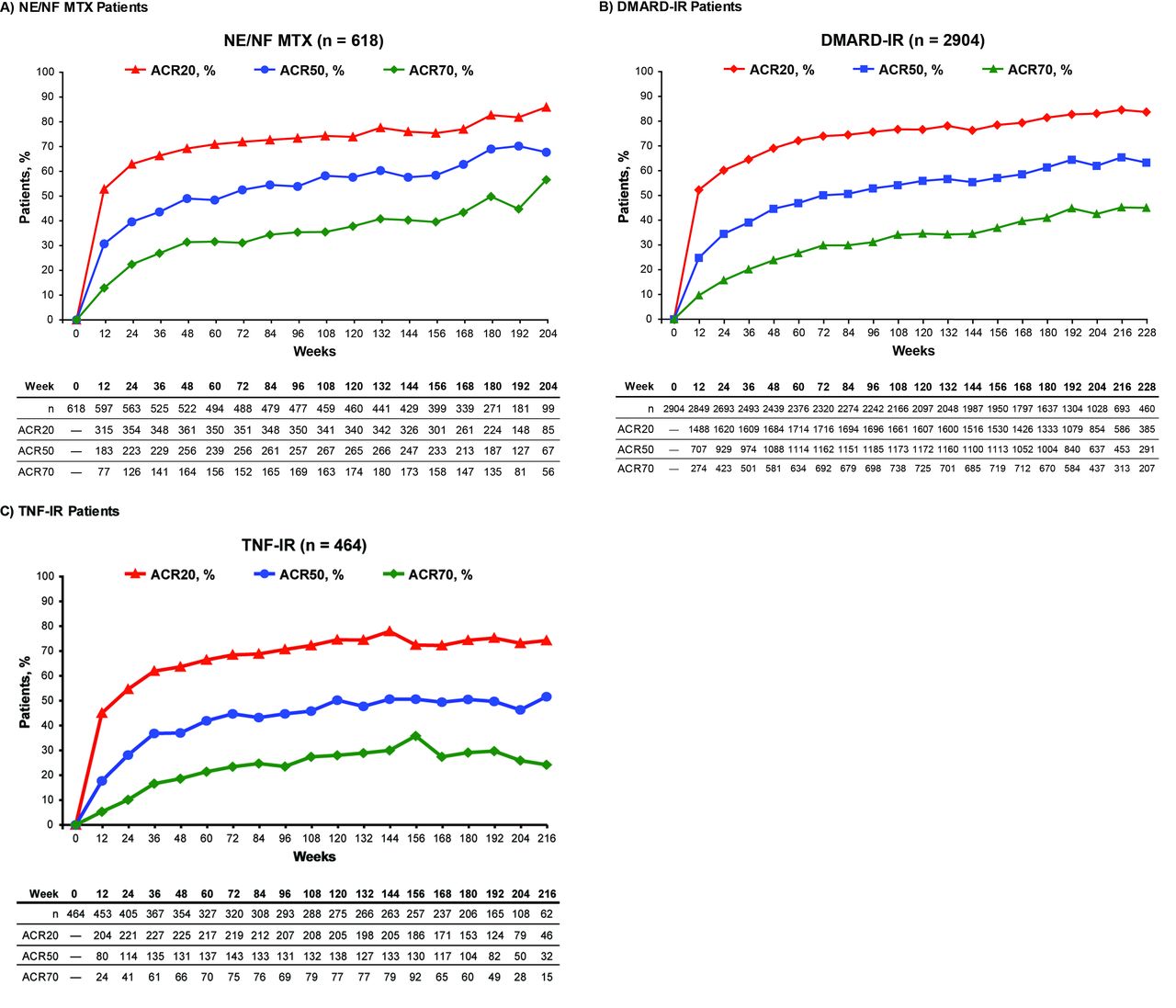
- Figure 2.
Proportions of patients who achieved ACR20/50/70 responses during longterm treatment with TCZ. (A) NE/NF MTX group. (B) DMARD-IR group. (C) TNF-IR group. Data are shown only for weeks containing ≥ 10% of patients originally included in each group at baseline. Last observation carried forward method was used for tender and swollen joint counts. No imputation was used for missing HAQ score, CRP, ESR, or visual analog scale assessments. CRP was used primarily for calculation of ACR response; if missing, ESR was used. Analysis was performed in successful completers, defined as patients who reached each timepoint. The number of patients with assessments decreased over time because some patients had not yet reached later assessments or had withdrawn. Patients who withdrew were classified as missing, and missing data were excluded from summary statistics. ACR: American College of Rheumatology; CRP: C-reactive protein; DAS28: Disease Activity Score at 28 joints; DMARD: disease-modifying antirheumatic drug; ESR: erythrocyte sedimentation rate; IR: inadequate response; LDA: low disease activity; MTX: methotrexate; NE/NF: never exposed/never failed; TNF: tumor necrosis factor; TCZ: tocilizumab.
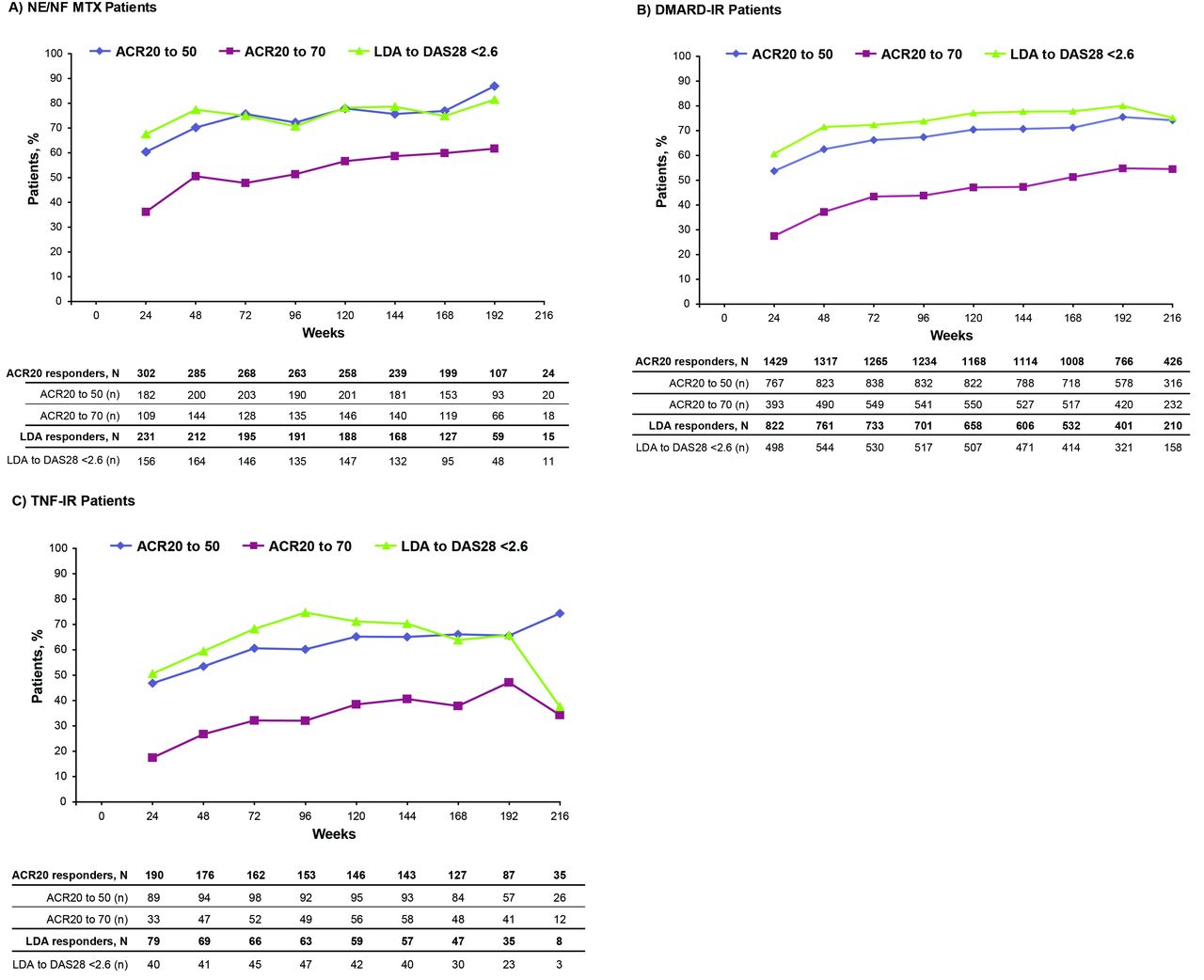
- Figure 3.
Patients who achieved ACR20 response at Week 12 and later achieved ACR50 and ACR70 responses, or LDA at Week 12 and DAS28 remission. (A) NE/NF MTX group. (B) DMARD-IR group. (C) TNF-IR group. Data are shown only for weeks with ≥ 10% of patients originally included in each group at baseline. Numbers of patients with assessments (n) decreased over time because some patients had not yet reached later assessments or had withdrawn. N represents the total number of responders, that is, patients with ACR20 (or LDA) response at Week 12 with assessment of ACR50 or ACR70 (or DAS28 remission) at each timepoint. ACR: American College of Rheumatology; DAS28: Disease Activity Score at 28 joints; DMARD: disease-modifying antirheumatic drug; IR: inadequate response; LDA: low disease activity; MTX: methotrexate; NE/NF: never exposed/never failed; TNF: tumor necrosis factor.
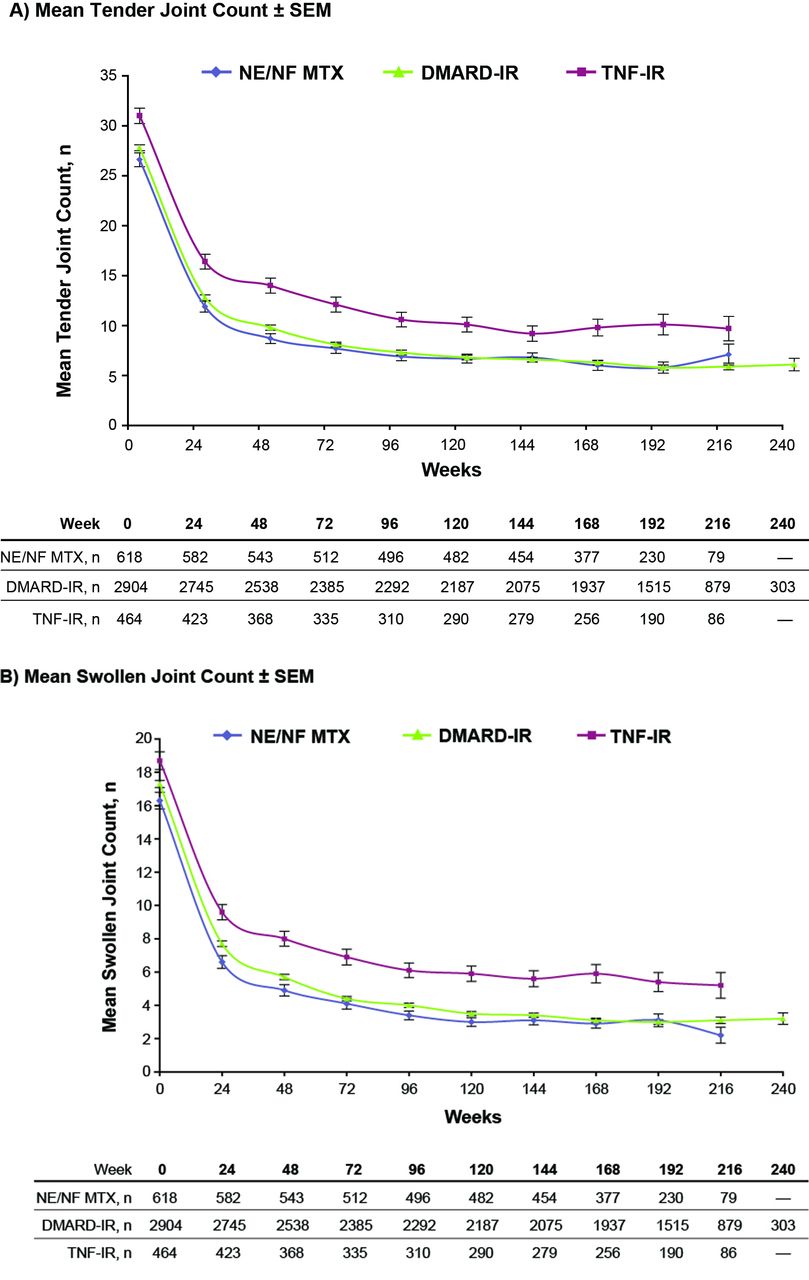
- Figure 4.
Summary of (A) tender joint count (68) and (B) swollen joint count (66) over time by treatment group. Tender and swollen joint count data are shown only for weeks containing ≥ 10% of patients originally included in each treatment group at baseline. Last observation carried forward was used for missing swollen or tender joint counts. Analysis was performed in successful completers, defined as patients who reached each timepoint. Numbers of patients with assessments decreased over time because some patients had not yet reached later assessments or had withdrawn. Patients who withdrew were classified as missing, and missing data were excluded from summary statistics. DMARD: disease-modifying antirheumatic drug; IR: inadequate response; MTX: methotrexate; NE/NF: never exposed/never failed; SEM: standard error of the mean; TNF: tumor necrosis factor.
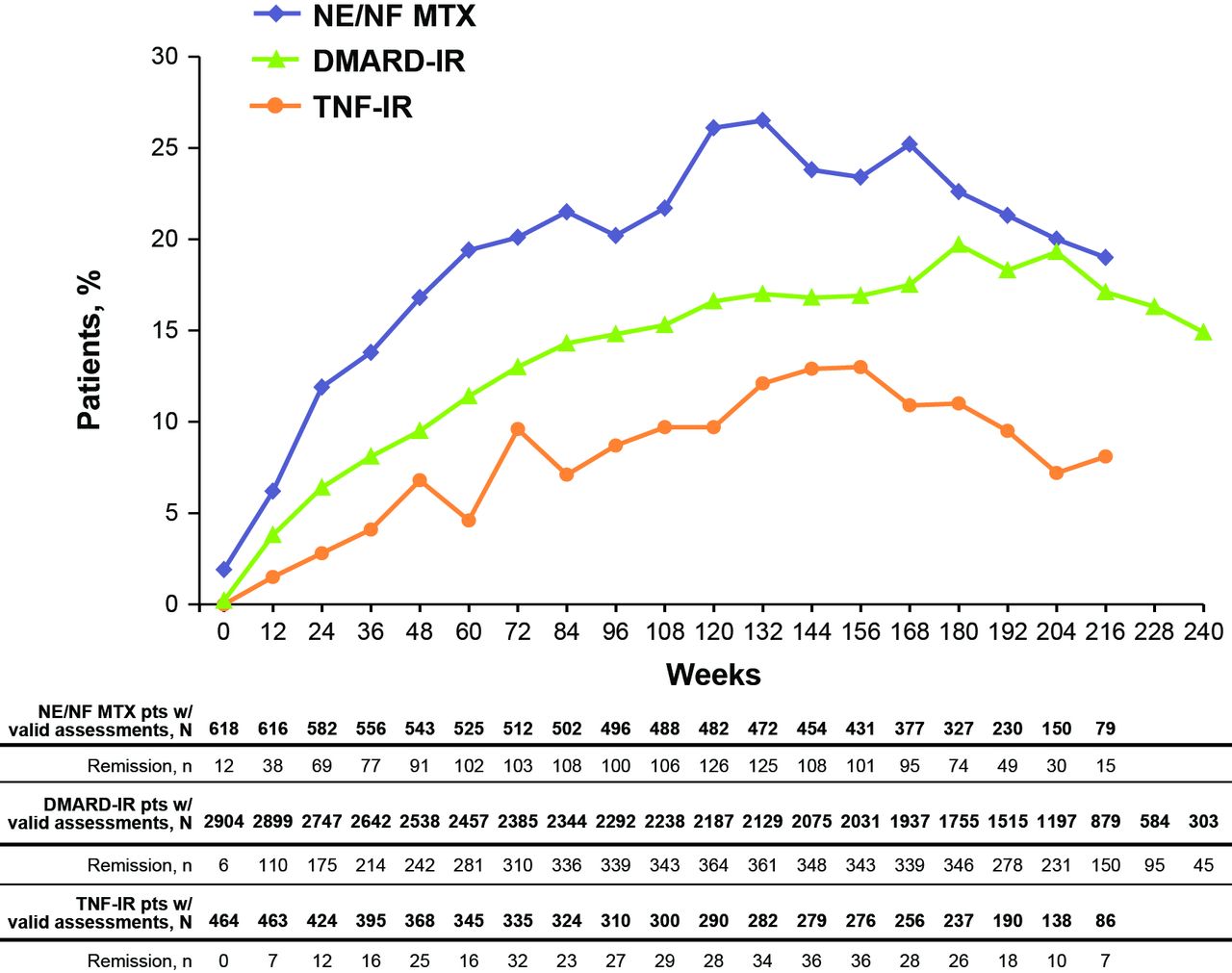
- Figure 5.
Patients who achieved low disease activity (LDA; DAS28 ≤ 3.2) or DAS28 remission (DAS28 < 2.6) during longterm treatment with TCZ. Data are shown only for weeks containing ≥ 10% of patients originally included in each group at baseline. Last observation carried forward was used for tender and swollen joint counts. No imputation was used for erythrocyte sedimentation rate or for Patient Global Assessment of Disease Activity score. Numbers of patients with assessments decreased over time because some patients had not yet reached later assessments or had withdrawn. DAS28: Disease Activity Score in 28 joints; DMARD: disease-modifying antirheumatic drug; IR: inadequate response; MTX: methotrexate; NE/NF: never exposed/never failed; TNF: tumor necrosis factor; TCZ: tocilizumab.
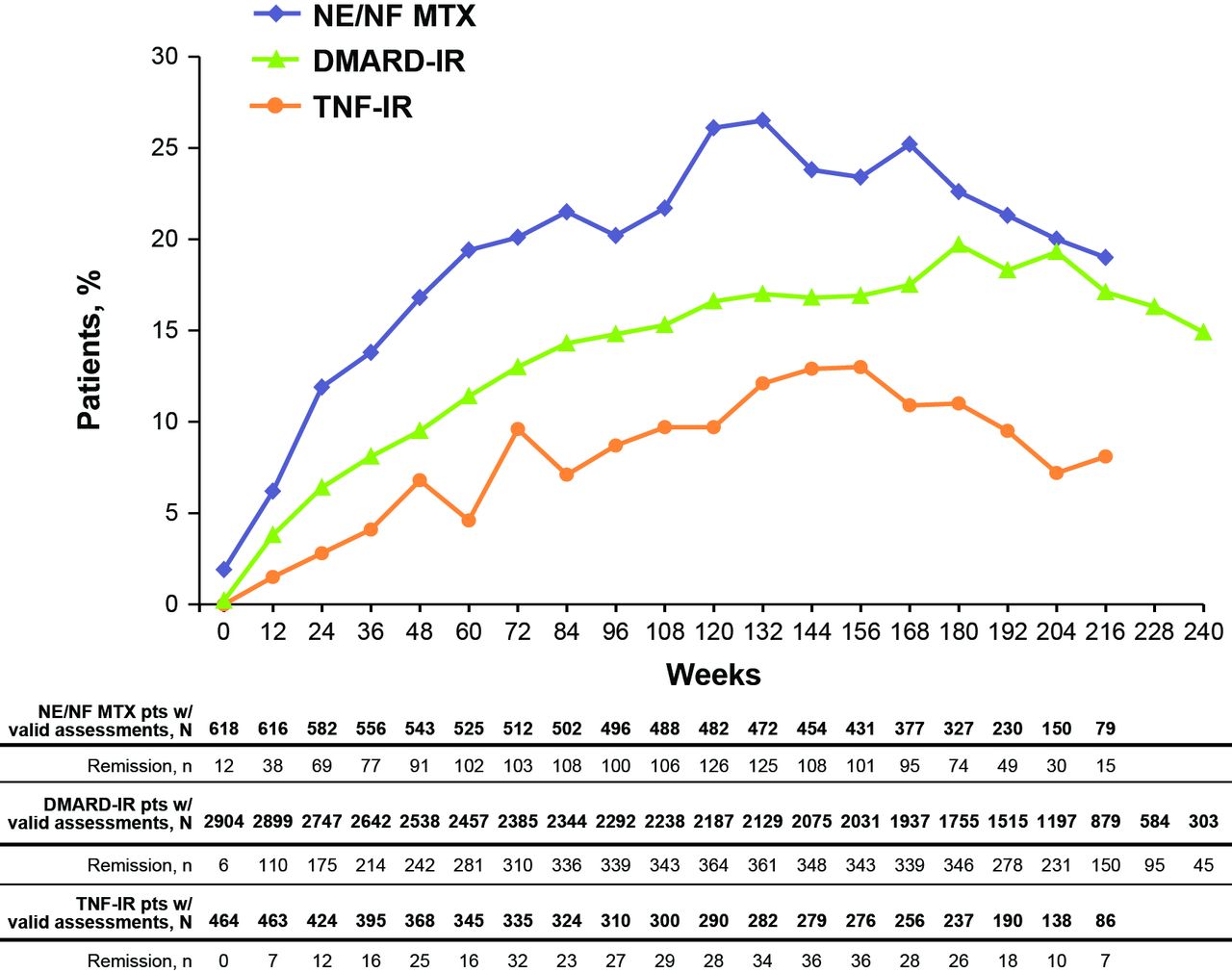
- Figure 6.
Patients who achieved remission according to ACR/EULAR Boolean criteria. Remission is achieved if the patient has no more than 1 tender joint, no more than 1 swollen joint, CRP no greater than 1 mg/dl, and Patient Global Assessment of Disease Activity score no greater than 1 cm. Data are shown only for weeks containing ≥ 10% of patients originally included in each group at baseline. Last observation carried forward was used for tender and swollen joint counts. Nonresponder imputation was used for missing CRP and Patient Global Assessment score. Numbers of patients with assessments decreased over time because some patients had not yet reached later assessments or had withdrawn. ACR: American College of Rheumatology; CRP: C-reactive protein; DMARD: disease-modifying antirheumatic drug; EULAR: European League Against Rheumatism; IR: inadequate response; MTX: methotrexate; NE/NF: never exposed/never failed; TNF: tumor necrosis factor.



Tables
- Table 1.
Study design and treatment features of tocilizumab phase III randomized controlled trials and open-label extensions.
Study Patient Population Treatment Duration Treatment Combination Therapy Rescue Therapya Efficacy Population*, n = 3986 All-exposed Safety Population*, n = 4009 All-control Safety Population**, n = 4199b Randomized Controlled Studies LITHE N = 1196c Moderate to severe active RA
MTX-IR2 yrs TCZ 4 mg/kg Q4W
TCZ 8 mg/kg Q4We
Placebo Q4WMTX 10–25 mg QW Wk 16: blinded TCZ 4 mg/kg (from placebo) or 8 mg/kg (from 4 mg/kg)
After 12 wks of escape 1 treatment: TCZ 8 mg/kgDMARD-IR group: n = 1149 n = 1149 initially randomly assigned to:
Control: n = 351
TCZ 4 mg/kg: n = 399
TCZ 8 mg/kg: n = 399Control: n = 392
TCZ 4 mg/kg: n = 399
TCZ 8 mg/kg: n = 399OPTION N = 623c Moderate to severe active RA
MTX-IR24 wks TCZ 4 mg/kg Q4W
TCZ 8 mg/kg Q4W
Placebo Q4WMTX 10–25 mg QW Wk 16: TCZ 8 mg/kg DMARD-IR group: n = 597 n = 597 initially randomly assigned to:
Control: n = 179
TCZ 4 mg/kg: n = 212
TCZ 8 mg/kg: n = 206Control: n = 204
TCZ 4 mg/kg: n = 212
TCZ 8 mg/kg: n = 206TOWARD N = 1220c Moderate to severe active RA
DMARD-IR24 wks TCZ 8 mg/kg Q4W
Placebo Q4W (randomized 2:1)DMARD Wk 16: adjustment of background DMARD DMARD-IR group: n = 1158 n = 1158 initially randomly assigned to:
Control: n = 356
TCZ 8 mg/kg: n = 802Control: n = 414
TCZ 8 mg/kg: n = 802RADIATE N = 499c Moderate to severe active RA
TNF-IR24 wks TCZ 4 mg/kg Q4W
TCZ 8 mg/kg Q4W
Placebo Q4WMTX 10–25 mg QW Wk 16: TCZ 8 mg/kg TNF-IR group: n = 464 n = 464 initially randomly assigned to:
Control: n = 126
TCZ 4 mg/kg: n = 163
TCZ 8 mg/kg: n = 175Control: n = 160
TCZ 4 mg/kg: n = 163
TCZ 8 mg/kg: n = 175AMBITION N = 673c Active RA
No MTX during last 6 mo and no MTX failure24 wks TCZ 8 mg/kg Q4Wf
MTX 7.5–20 mg weekly
Substudy: placebo 8 wks then TCZ 8 mg/kg
Q4W for 16 wksNone Substudy only up to wk 8: TCZ 8 mg/kg NE/NF MTX group: n = 618 n = 618 initially randomly assigned to:
Control: n = 330
TCZ 8 mg/kg: n = 288Control: n = 385g
TCZ 8 mg/kg: n = 288Phase 1 Drug Interaction N = 23 RA patients Single dose TCZ 10 mg/kg
TCZ 10 mg/kg + simvastatin on days 1, 15, and 43MTX 10–25 mg QW NA NA n = 23 initially randomly assigned to: TCZ 10 mg/kg: n = 23 NA Longterm Extension, Open-label Studies LITHE extension phase N = 909d Ongoing study; moderate to severe active RA
MTX-IR3 yrs (planned) TCZ 8 mg/kg Q4W MTX 10–25 mg/wk NA NA 909 NA GROWTH95 N = 537 Patients completing treatment in OPTION −5 yrs (planned) TCZ 8 mg/kg Q4W MTX 10–25 mg/wk NA NA 537 NA GROWTH96 N = 2066 Patients completing treatment in AMBITION, RADIATE, TOWARD, and drug interaction study −5 yrs (planned) TCZ 8 mg/kg Q4W Study dependent
None (AMBITIONf)
MTX, 10–25 mg/wk (RADIATE) Other DMARD (TOWARD)NA NA 2066 NA -
Abbreviations
-
↵* TCZ-treated patients (from controlled and extension studies).
-
↵** TCZ- or control-treated (from controlled studies).
-
↵a Patients who did not attain 20% improvement in swollen joint count (SJC) or tender joint count (TJC) could receive rescue therapy during the randomized phase.
-
↵b Does not include 23 patients from the phase I clinical pharmacology study and 12 patients initially randomly assigned in the randomized controlled studies who did not receive study treatment: LITHE (n = 6), OPTION (n = 1), TOWARD (n = 4), and RADIATE (n = 1).
-
↵c No. patients randomly assigned during phase III study.
-
↵d Estimated no. patients who entered extension phase (study is ongoing; final data not available).
-
↵e At Week 52, all patients were required to start open-label TCZ 8 mg/kg for Year 2 unless they had attained ≥ 70% improvement in SJC and TJC, allowing them to continue the blinded therapy they were receiving at the end of Year 1 to Week 104.
-
↵f Patients who attained ≥ 50% reduction in TJC and SJC (assessed from baseline) while receiving initially randomized study treatment at weeks 20 and 24 could opt to continue their current blinded treatment in a transition phase that lasted until the last patient enrolled in AMBITION completed the 24-week randomized phase of the study; 234 AMBITION patients continued to receive TCZ 8 mg/kg monotherapy for all evaluations.
-
↵g 284 patients from blinded study; 101 patients from placebo substudy. DMARD: disease-modifying antirheumatic drug; IR: inadequate response; MTX: methotrexate; NA: not applicable; NE/NF: never exposed/never failed; QW: once every week; Q4W: once every 4 weeks; RA: rheumatoid arthritis; SJC: swollen joint count; TCZ: tocilizumab; TJC: tender joint count; TNF: tumor necrosis factor.
-
All-control Population, n = 4199 All-exposed Population (cutoff date: Feb. 17, 2010), n = 4009 Control, n = 1555 TCZ 4 mg/kg + DMARD/MTX, n = 774 TCZ 8 mg/kg ± DMARD/MTX, n = 1870 Overall 0–12 Mo 13–24 Mo 25–36 Mo > 36 Mo Total duration, PY 824.6 564.6 1194.1 12293.1 3470.9 3026.1 2732.7 3063.5 AE, rate/100 PY Anya 339.0 358.0 381.6 257.2 379.4 275.8 252.4 224.5 Severea,b — — — 16.8 22.2 16.7 15.8 12.9 Led to withdrawala 6.9 10.1 10.2 5.2 9.2 4.4 3.8 2.9 Led to dose modification/interruptiona 27.8 32.9 34.2 36.0 40.3 38.5 38.7 36.8 Serious AE, rate/100 PY Anya 14.4 13.6 14.5 14.1 15.5 13.4 14.8 13.6 Death rate/100 PY 0.73 0.00 0.75 0.45 0.55 0.33 0.44 0.29 AE with rate ≥ 2/100 PY by SOCa Infections and infestations 87.9 93.9 93.4 68.7 96.7 83.8 80.8 73.7 Gastrointestinal disorders 55.3 47.3 56.8 32.7 55.0 32.8 29.3 23.9 Musculoskeletal and connective tissue disorders 38.8 30.3 29.1 27.5 34.7 31.1 27.8 25.2 Nervous system disorders 20.5 21.4 24.0 12.8 22.4 13.0 10.6 8.9 Skin and subcutaneous disorders 19.6 29.4 31.7 15.6 27.3 14.5 12.0 10.8 General disorders and administrative site conditions 18.2 17.5 18.0 9.2 16.2 8.3 7.6 5.2 Respiratory, thoracic, and mediastinal disorders 14.8 18.4 17.5 11.8 17.1 12.3 11.0 10.1 Injury, poisoning, and procedural complications 13.9 15.8 15.8 14.5 16.9 15.1 14.3 13.7 Investigations 12.4 17.5 25.0 10.8 20.9 9.8 8.2 6.2 Vascular disorders 10.3 14.2 12.4 8.4 13.3 8.8 7.8 6.2 Psychiatric disorders 7.9 8.3 8.3 5.4 8.2 5.5 5.5 3.4 Metabolism and nutrition disorders 6.3 7.4 7.1 7.3 8.9 8.4 6.1 7.5 Blood and lymphatic disorders 5.3 5.7 7.3 5.2 7.4 4.6 5.4 5.5 Eye disorders 5.0 6.4 8.2 6.1 7.9 6.3 6.0 5.2 Renal and urinary disorders 4.0 2.7 4.1 2.9 3.6 2.8 2.7 2.8 Reproductive and breast disorders 4.4 4.3 5.3 3.4 4.6 3.4 2.9 3.0 Cardiac disorders 3.5 2.7 4.0 4.1 4.5 4.5 3.8 4.0 Ear and labyrinth disorders 3.3 3.9 2.9 2.3 3.1 2.7 2.2 1.6 Neoplasms benign, malignant, unspecified (including cysts and polyps) 1.7 5.1 2.6 3.1 3.5 2.9 3.4 3.0 Immune disorders 1.9 1.8 2.4 1.6 2.3 1.8 1.6 1.0 Hepatobiliary disorders 1.7 1.1 2.8 1.8 2.2 1.5 1.9 2.0 SAE with rate ≥ 1/100 PY by SOCa Infections and infestations 3.3 3.5 4.8 4.4 4.4 3.8 5.0 4.7 Gastrointestinal disorders 1.0 0.9 1.7 1.2 1.5 1.0 1.1 1.2 Musculoskeletal and connective tissue disorders 1.8 1.2 0.6 0.9 1.0 1.0 0.9 0.8 Nervous system disorders 0.7 1.4 0.8 0.8 1.0 0.8 0.7 0.7 Injury, poisoning, and procedural complications 1.1 1.1 1.8 1.2 1.4 1.5 1.0 1.0 Cardiac disorders 1.1 0.4 1.1 1.0 1.0 1.0 1.1 1.0 Neoplasms, benign, malignant, unspecified (including cysts and polyps) 0.8 1.8 0.5 1.2 1.0 1.0 1.4 1.3 -
↵a Multiple occurrences of the same AE in a patient are counted once in each period.
-
↵b Intensity of AE graded by the investigator as mild, moderate, or severe. PY: patient-years; SAE: serious adverse event; SOC: system organ class; TCZ: tocilizumab; DMARD: disease-modifying antirheumatic drug; MTX: methotrexate.
-
- Table 3.
ACR/EULAR remission rates and components at the last evaluable timepoint in the efficacy population. Remission is achieved if the patient has no more than 1 tender joint, no more than 1 swollen joint, CRP no greater than 1 mg/dl, and Patient Global Assessment of Disease Activity score no greater than 1. Last evaluable timepoint is the last week with ≥ 10% of patients originally included in each group at baseline. Last observation carried forward was used for TJC and SJC. Nonresponder imputation was used for missing CRP and Patient Global Assessment Disease Activity score.
Criterion, n (%) NE/NF MTX, n = 618 DMARD-IR n = 2904 TNF-IR, n = 464 Last evaluable timepoint Week 216 Week 240 Week 216 No. patients with efficacy assessment at timepoint 79 303 86 TJC ≤ 1 39 (49.4) 170 (56.1) 30 (34.9) SJC ≤ 1 56 (70.9) 188 (62.0) 39 (45.3) CRP ≤ 1 mg/dl 44 (55.7) 200 (66.0) 60 (69.8) Patient global assessment of disease activity score ≤ 1 (1–10 scale) 18 (22.8) 58 (19.1) 14 (16.3) Remission (all ≤ 1) 15 (19.0) 45 (14.9) 7 (8.1) Remission (SDAI ≤ 3.3) 16 (20.3) 63 (20.8) 10 (11.6) -
ACR: American College of Rheumatology; CRP: C-reactive protein; DMARD: disease-modifying antirheumatic drug; EULAR: European League Against Rheumatism; IR: inadequate response; MTX: methotrexate; NE/NF: never exposed/never failed; SDAI: Simplified Disease Activity Index; SJC: swollen joint count; TJC: tender joint count; TNF: tumor necrosis factor.
-








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}