

Abstract
Objective. To investigate disease course, outcome, and predictors of outcome in an unselected population-based cohort of individuals diagnosed with juvenile chronic arthritis (JCA) followed for 17 years.
Methods. The cohort consisted of 132 incidence JCA cases identified 1984–1986 according to EULAR criteria. At 5-year followup, 129 individuals underwent joint assessment, laboratory measurements, radiographic examination, and medication and functional assessment. At 17-year followup, 86 were examined with joint assessment, laboratory measurements, medication assessment, Health Assessment Questionnaire (HAQ), Keitel functional test (KFT), and Medical Outcomes Study Short Form-36 (SF-36).
Results. At 17-year followup, 40% were in remission, 44% changed subgroups, median HAQ score was 0.0 (range 0.0–1.5), and median KFT was 100 (range 54–100). SF-36 scores were significantly lower compared to a reference group. Thirty-nine percent of those in remission at 5-year followup were not in remission at 17-year followup. In multivariate analyses of variables from the 17-year followup: remission was predicted by remission at 5-year followup (OR 4.8); HAQ > 0 by rheumatoid factor (RF)-positivity at 5-year followup (OR 3.6); KFT < 100 by nonremission (OR 11.3); and RF-positivity (OR 5.6) at 5-year followup; and the SF-36 physical component summary score above average of the reference group by remission at 5-year followup (OR 5.8).
Conclusion. This longterm study of 86 individuals with JCA showed large variability of disease courses and of impaired health-related quality of life. Sixty percent were not in remission at 17-year followup. Longterm outcome was best predicted by and associated with characteristics at 5-year followup rather than those at onset.
- JUVENILE RHEUMATOID ARTHRITIS
- JUVENILE CHRONIC ARTHRITIS
- JUVENILE IDIOPATHIC ARTHRITIS
- PROGNOSIS
- OUTCOME ASSESSMENT
Juvenile chronic arthritis (JCA) and the most recent designation, juvenile idiopathic arthritis (JIA), are broad terms that describe a clinically heterogeneous group of arthritides of unknown cause, which begin before 16 years of age1. It is a rare disease with annual incidence between 7 and 23 children/100,000 in the Nordic countries2. There are a number of longterm studies of outcome of JCA/JIA but almost all are retrospective, cross-sectional, or selective, with varying classification criteria and assessment tools and diverse results3,4,5,6,7,8,9,10,11. Although many of the studies have accumulated much information, prognostic prediction of longterm outcome early after disease presentation remains difficult12.
In recent decades many classification criteria have been used and there are still new suggestions13, which also makes comparison of this already heterogeneous group difficult. Earlier, the American College of Rheumatology (ACR) criteria were used for juvenile rheumatoid arthritis (JRA)14 and in Europe the European League Against Rheumatism (EULAR) criteria were frequently used for JCA15. However, in the last decade the International League of Associations for Rheumatology (ILAR) criteria for JIA16 have commonly been used.
The aim of our study was to investigate disease course, outcome, and predictors of outcome in an unselected cohort of incidence cases with JCA followed for 17 years. Because this is a population-based longterm cohort study and the unselected participating individuals were diagnosed with JCA according to the EULAR criteria, we continued to use that term in this analysis.
MATERIALS AND METHODS
Design
A multicenter, prospective, longitudinal, population-based 17-year outcome study of JCA.
Patients
Patients were recruited from a prospective population-based epidemiological analysis of JCA in southwestern Sweden17. The study was conducted according to The Helsinki Declaration and approved by the regional ethics committee. The cohort consisted of 132 incidence cases identified from January 1, 1984, to December 31, 198618. All patients from pediatric clinics and local pediatricians, with onset of JCA during the study period, were reported. Patients with JCA born after 1967 were also sought at adult rheumatology clinics and orthopedic clinics. For the 17-year followup they were identified through the Swedish national civil register.
The EULAR criteria15 were used to define cases of JCA and to divide patients into subgroups, as follows: (1) onset with systemic features; (2) onset with polyarthritis in the absence of marked systemic features, 5 or more joints affected; (3) onset with arthritis affecting 2 to 4 joints — pauciarticular; (4) or in the case of only 1 joint — monoarticular subgroup. This subgroup was separated from group 3, although it is not formally a subgroup within JCA. Within these groups children with probable juvenile ankylosing spondylitis (JAS), juvenile psoriatic arthritis (JPsA), and arthritis associated with inflammatory bowel disease (IBD) were also identified. Cases were identified as JAS if peripheral arthritis was combined with radiological evidence of sacroiliitis or with clinical evidence of sacroiliitis or axial involvement in combination with enthesitis. JPsA was defined as arthritis in combination with psoriasis diagnosed by a dermatologist. To identify a case of arthropathy associated with IBD, an intestinal mucosal biopsy indicating ulcerative colitis or Crohn disease was required. If a patient changed subgroup during followup the new subgroup was defined as the disease-course subgroup. A change from systemic onset to another subgroup required absence of systemic features for at least 2 years.
These EULAR criteria were chosen because they were used for patient retrieval and classification in the original epidemiological study, and it was not possible to convert the patients to the new set of criteria for JIA from ILAR16,19 retrospectively, because the inclusion criteria differ. The time of disease onset was defined as the time that onset of symptoms occurred and the onset type was determined 6 months later.
Followup schedule
Patients were examined and data were collected at onset, annually the first 5 years, and at 17-year followup.
Arthritis and joint involvement
Heat, pain (either tenderness or pain on motion), soft-tissue swelling, and restricted range of motion were recorded at inclusion, at 5-year followup, and at 17-year followup. If at least 2 of the factors were present, the joint assessment was considered to represent arthritis and if any of the factors were present, the joint assessment was considered as involved, i.e., showed either signs of active synovitis or residuals of previous synovitis.
Disease activity
The disease activity was evaluated by a physician’s overall assessment at inclusion, at 5-year followup (BAG), and at 17-year followup (LB) according to EULAR20,21, as follows: active = increasing number of joints irrespective of drug therapy; stable = stable number of joints but requiring drug therapy; inactive = no evidence of active synovitis and/or active extraarticular features and without drugs for < 2 years; or remission = no evidence of active synovitis and/or active extraarticular features and without drugs for ≥ 2 years. All disease-modifying antirheumatic drugs (DMARD) including biologics as well as analgesics, nonsteroidal anti-inflammatory drugs (NSAID), and glucocorticosteroids were considered as drugs. The disease activity levels were designated as remission = 1, inactive = 2, stable = 3, and active = 4. Nonremission was defined as inactive, stable, or active.
Disease activity duration score
Disease activity was divided into active + stable and inactive + remission and a disease activity duration score was defined as the percentage of time the patient had active + stable disease during the first 5 years of the disease.
Laboratory investigations
Erythrocyte sedimentation rate (ESR) was measured using standard procedures and was analyzed at inclusion, at 5-year followup, and at 17-year followup. At inclusion, antinuclear antibodies (ANA) were analyzed by indirect immunofluorescence using rat kidney sections and rheumatoid factor (RF) was analyzed by latex slide agglutination test, where titers > 1/25 and > 1/20, respectively, were considered positive, according to the clinical laboratories involved at that time.
Because studies22,23 have shown class-specific RF to be present in some childhood arthritis, IgM RF and IgA RF were analyzed at 5-year followup using an enzyme immunoassay (Pharmacia RF IgM EIA and RF IgA EIA; Pharmacia Diagnostics). Serum concentrations > 7.34 and > 3.58 arbitrary units/ml, respectively, were considered positive24.
Medication and arthroplasty
Medication and arthroplasty were registered annually during the first 5 years and at 17-year followup. The medication was divided into analgesics, NSAID, glucocorticosteroids, DMARD, and biologics.
Function and health-related quality of life
The Childhood Health Assessment Questionnaire (CHAQ)25 was used to evaluate functional status at the 5-year followup. If the child was < 9 years of age, 1 parent was asked to answer the questionnaire. At 17-year followup functional status was evaluated by HAQ26 and by the Keitel functional test (KFT)27. The KFT is a measure of 24 simple movement patterns. A maximum score of 100 represents the best movement pattern. In dichotomous analysis 100 was coded 1 and < 100 was coded 0.
The individual’s self-reported health-related quality of life was assessed using the Swedish version of the Medical Outcomes Study Short Form-36 Health Survey (SF-36)28, a validated 36-item questionnaire comprising 4 domains of physical health: physical functioning (PF), role physical (RP), bodily pain (BP), and general health (GH); and 4 domains of mental health: vitality (VT), social functioning (SF), role emotional (RE), and mental health (MH). Scores range from 0 to 100, higher score reflecting better health. The 8 subscales can be summarized to 1 physical component score (PCS) and 1 mental component score (MCS) standardized to a mean (SD) value of 50. To compare the patients to a normative database, an age- and sex-matched reference group (n = 520) was randomly drawn from the Swedish SF-36 national normative database (n = 8930)29.
Radiographic examinations
Radiographs of the affected joints performed at 5-year followup or during the preceding year were evaluated and classified as follows: normal; stage I – early changes (periarticular soft-tissue swelling/periarticular osteoporosis/periosteal new bone formation); or stage II – advanced changes (cartilage destruction/bone destruction/bony ankylosis/large joint subluxations, epiphyseal fractures/vertebral compression fractures)30.
Statistical methods
Data were analyzed using the PASW Statistics 18 (SPSS Inc.). Values are expressed as mean ± 1 (SD) or median and range. Comparisons between groups were analyzed by the Mann-Whitney U test (2-tailed). Chi-square test was used for categorical data and Fisher exact test was computed when cells had expected values < 5. Correlations were calculated using Spearman rank correlation coefficient (rs). One-way ANOVA with posthoc Games-Howel for unequal variances was applied for comparison between multiple groups. After univariate analysis, multiple logistic regression with forward conditional method was used. In dichotomous variables, event was coded 1 and no event coded 0. Limit value for significance was set at p < 0.05 for all tests.
RESULTS
Study cohort
Out of 132 patients, 129 (97%) attended the 5-year followup visit, which occurred a mean 5.4 ± 0.6 years after disease onset, and 86 individuals (65%) participated in the 17-year followup, a mean 16.9 ± 1.0 years after disease onset (Figure 1). The sex distribution at the 17-year followup was slightly higher for the girls (61/86, 71%) compared to baseline (84/132, 64%), but this was not significant (p = 0.32). The individuals lost between the 5-year and the 17-year followup did not differ significantly from those at the 17-year followup with respect to age at onset (p = 0.69), presence of RF (p = 0.56) and ANA (p = 0.88) at baseline, number of joints with arthritis (p = 0.16), joints with involvement (p = 0.81) during the first year of disease, disease activity duration score during the first 5 years of disease (p = 0.78) or disease activity (p = 0.54), number of joints with arthritis (p = 0.28) or joints with involvement (p = 0.34), and CHAQ score at 5-year followup (p = 0.30). The rest of this report gives the results of the 86 individuals who were followed for 17 years.

Procedure of the prospective, longitudinal, population-based 17-year outcome study of 86 incidence cases of juvenile chronic arthritis.
Data at onset
Data from disease onset are illustrated in Table 1. The median age at onset was 8.3 years (range 0.6–15.8) for both girls and boys. The pauciarticular disease subgroup was most common at disease onset (38%), followed by the monoarticular (26%) and the polyarticular subgroups (22%). Only 9 individuals received DMARD within the first year from disease onset and another 5 individuals within the first 2 years from disease onset. All but 1 of these 14 early DMARD treatments were hydroxychloroquine and the majority of these early treatments were given in the polyarticular-onset subgroup. There was no significant association between early DMARD treatment and outcome at 17-year followup.
Characteristics at disease onset: subgroups, sex distribution, onset age, laboratory signs of inflammation assessed as erythrocyte sedimentation rate (ESR), presence of rheumatoid factor (RF; titers > 1/25 are positive), and antinuclear antibody (ANA; titers > 1/20 are positive) at disease onset in 86 incidence cases of juvenile chronic arthritis followed for 17 years. Values are medians and ranges if not indicated otherwise.
Data at 5-year followup
Data at 5-year followup are presented in Table 2. Thirty-three individuals (38%) were in remission, 17 (20%) had inactive disease, 25 (29%) had stable, and 11 (13%) had active disease. There was no significant association between disease activity and baseline data. Median CHAQ score at 5-year followup was 0.1 (range 0.0–1.9) and in univariate analysis it was significantly associated with age at disease onset (rs = 0.369, p = 0.001), number of involved joints at baseline (rs = 0.296, p = 0.007), and presence of ANA at baseline (rs = −0.260, p = 0.020). The median disease activity duration index was median 0.39 (range 0.04–1.00) and it was significantly associated with number of involved joints (rs = 0.424, p < 0.001) and presence of ANA at baseline (rs = −0.235, p = 0.033).
Five-year followup; subgroups, sex distribution, erythrocyte sedimentation rate (ESR), Childhood Health Assessment Questionnaire (CHAQ), disease activity, disease activity duration index during the first 5 years, number of arthritis and involved joints, radiographic joint changes, and use of disease-modifying antirheumatic drugs (DMARD) in 86 incidence cases of juvenile chronic arthritis followed for 17 years. Values are median (range) if not indicated otherwise.
Data from the 17-year disease course
During the 17-year disease course, 38 of the 86 individuals (44%) changed disease subgroup. From the monoarticular and pauciarticular subgroups, 16 of 55 (29%) changed to the polyarticular disease course. During the first 5 years of disease, 30 (35%) changed disease subgroups and between the 5-year and the 17-year followup 11 (13%) changes of disease subgroup occurred (Figure 2). Of the 33 individuals who were in remission at 5-year followup, only 20 remained in remission at the 17-year followup, whereas 4 were in the stable category and 9 in the inactive category. Twenty-one individuals had an early remission (defined as inactive disease within the first year and remission within the first 3 years of disease), and out of these only 12 remained in remission at 17-year followup whereas 5 were in stable and 4 in the inactive category. On the other hand, out of the 19 individuals with continuous active disease during the first 5 years, 4 were in remission at 17-year followup. During the first 5 years, 7 individuals had uveitis verified by an ophthalmologist and at 17-year followup another 4 had had uveitis according to the self-report questionnaire.

Changes of disease course subgroup during the 17-year followup for 86 incidence cases of juvenile chronic arthritis. JAS: juvenile ankylosing spondylitis; JPA: juvenile psoriatic arthritis; IBD: arthritis associated with inflammatory bowel disease.
Data at 17-year followup
Data at 17-year followup are presented in Table 3. Thirty-four (40%) individuals were in remission, 16 (19%) had inactive, 34 (40%) had stable, and 2 (2%) had active disease. Twenty individuals were treated with DMARD including corticosteroids and biologics: methotrexate (n = 12), sulfasalazine (n = 5), hydroxychloroquine (n = 1), prednisone (n = 2), and tumor necrosis factor inhibitors (n = 2). Two individuals had undergone major arthroplasty, one with shoulder replacement, elbow replacement, and bilateral hip replacement; the other with wrist arthrodesis. Both were in the polyarticular-onset subgroup. The median HAQ score was 0.0 (range 0.0–1.5), 54% of the individuals had HAQ = 0, and 25% had HAQ ≥ 0.5. The median Keitel functional test score was 100 (range 54–100) and 57% of the individuals had KFT score = 100. The median ESR was 8 (range 1–66). The number of joints with arthritis was significantly higher for females (p = 0.022) and the number of involved joints was positively correlated to the number of involved joints at baseline (rs = 0.240, p = 0.027).
Seventeen-year followup; subgroups, sex distribution, erythrocyte sedimentation rate (ESR), Health Assessment Questionnaire (HAQ), Keitel functional test (KFT), disease activity, number of arthritis and involved joints, and use of disease-modifying antirheumatic drugs (DMARD) in 86 incidence cases of juvenile chronic arthritis followed for 17 years. Values are median (range) if not indicated otherwise.
SF-36
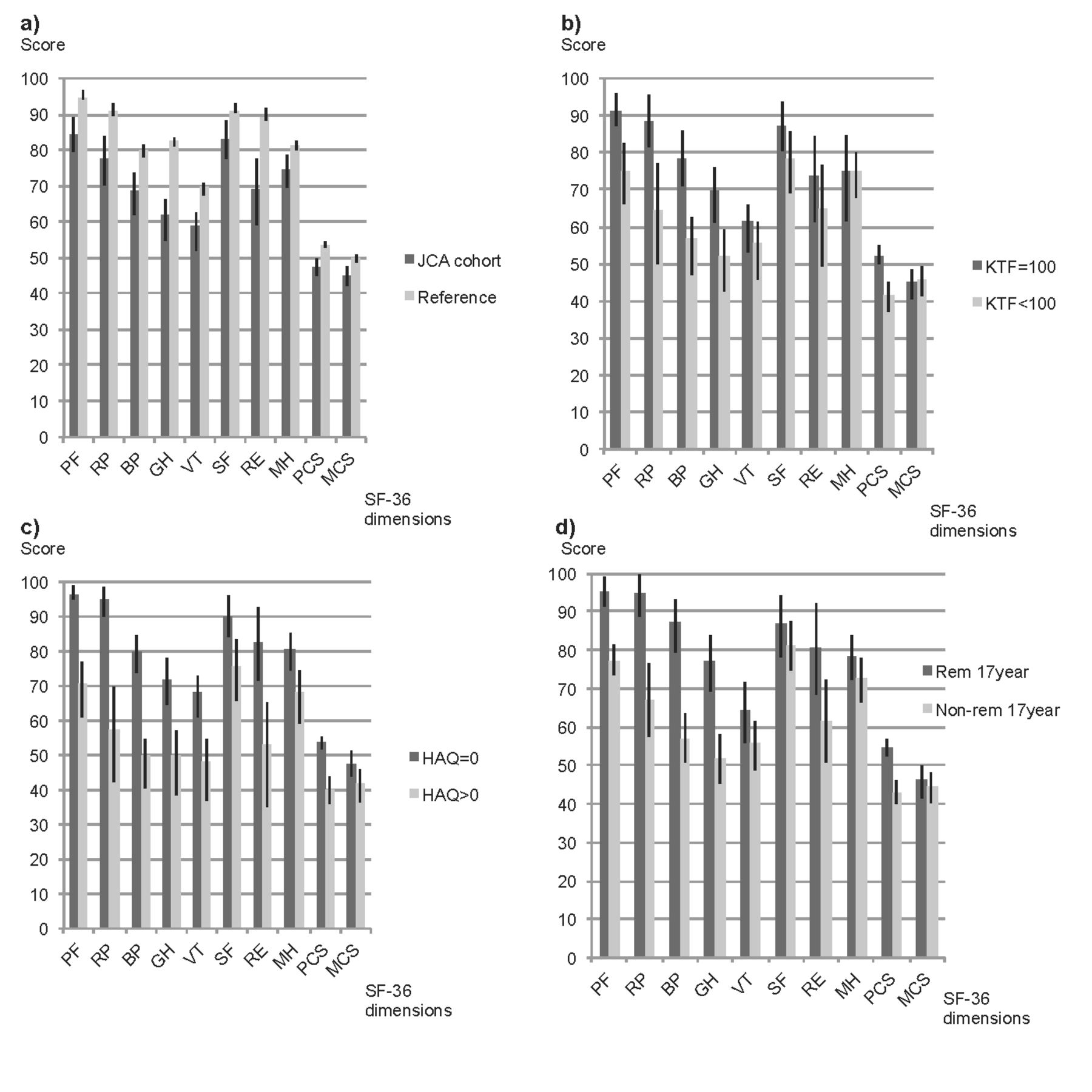
The SF-36 results are illustrated in Figure 3. In comparison with the age- and sex-matched reference population, individuals with JCA scored significantly lower in all domains: MH with p = 0.003, SF and MCS with p = 0.001, and the other 5 domains with p < 0.001. The individuals in remission at 17-year followup scored significantly better compared to the individuals in nonremission in all the physical health domains, with p < 0.001 for PF, RP, BP, GH, and PCS, but only for RE (p = 0.021) among the mental domains. A high HAQ score at the 17-year followup was associated with low scores in all the SF-36 domains with PCS (rs = −0.706, p < 0.001) and MCS (rs = −0.284, p = 0.008).

Medical Outcomes Study Short Form-36 health survey (SF-36) mean scores (95% interval of the mean) in the 17-year followup for 86 incidence cases of juvenile chronic arthritis (JCA). A. The JCA cohort compared to age- and sex-matched reference population. (B) The JCA individuals with normal Keitel functional test (KFT) results compared to those with affected KFT. (C) JCA individuals with normal Health Assessment Questionnaire (HAQ) scores compared to those with affected HAQ results. (D) JCA individuals in remission (Rem) at 17-year followup compared to those not in remission. SF-36 domains are physical functioning (PF), role physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role emotional (RE), and mental health (MH). Scores range from 0–100, higher score reflecting better health. The 8 subscales can be summarized to 1 physical component score (PCS) and 1 mental component score (MCS).
Predictors at baseline and at 5 years for outcomes at the 17-year followup. Remission at 17-year followup
There was no significant association between remission and baseline variables such as sex, age at onset, onset subgroup, ANA, RF, number of joints with arthritis, number of joints with involvement, or ESR. In univariate analysis, remission at 17-year followup was associated with remission at 5-year followup and was inversely associated with CHAQ score, number of involved joints at 5-year followup, and disease activity duration index during the first 3 years, first 4 years, and first 5 years of disease (Table 4).
Predictors at first 5 years and 5-year followup associated with outcome at 17-year followup for 86 incidence cases of juvenile chronic arthritis. Univariate correlations with Spearman correlation coefficient are used for comparison between continuous and ordinal variables and chi-square test/Fisher exact test (FET) are used for comparison between categorical variables.
In a multiple logistic regression with variables at the 5-year followup dichotomized as remission/nonremission, CHAQ score was 0/> 0, disease activity duration index ≤ 0.5/> 0.5, and number of involved joints 0/> 0; remission at 5-year followup was the most important variable predicting remission at the 17-year followup (OR 4.8, 95% CI 1.8–12.5).
HAQ score at 17-year followup
In univariate analysis, HAQ score was significantly associated with CHAQ score, number of involved joints, and nonremission at 5-year followup. HAQ was also associated with RF positivity at 5-year followup and disease activity duration index during the first 5 years of disease (Table 4). There were no significant associations with baseline variables.
In a multiple logistic regression with dichotomized variables at the 5-year followup, RF positivity at 5-year followup was the most important variable associated with HAQ > 0 at the 17-year followup (OR 3.6, 95% CI 1.0–13.3).
KFT at the 17-year followup
In univariate analysis, the KFT result was significantly associated with number of involved joints at baseline and disease activity duration index during the first 2, 3, 4, and 5 years of disease (Table 4). The KFT result was also significantly associated with CHAQ score, number of joints with arthritis, number of involved joints, RF positivity, and nonremission at 5-year followup.
In a multiple logistic regression with dichotomized variables at the 5-year followup, nonremission at 5-year followup (OR 11.3, 95% CI 2.7–47.9) and RF positivity at 5-year followup (OR 5.6, 95% CI 1.0–30.6) were the most important variables for KFT score < 100 at the 17-year followup.
SF-36 at 17-year followup
In univariate analysis the SF-36 PCS was significantly associated with disease activity duration index during the first 2, 3, 4, and 5 years of disease and with CHAQ, number of joints with arthritis, number of involved joints, and nonremission at 5-year followup (Table 4). There was no significant association for PCS with baseline variables and no significant association for MCS with either baseline or 5-year followup variables.
In a multiple logistic regression with dichotomized variables at the 5-year followup, remission at 5-year followup was the most important variable associated with SF-36 PCS, better than the average of the reference group at 17-year followup (OR 5.8, 95% CI 2.2–15.4).
DISCUSSION
This is a unique longitudinal 17-year prospective study of incidence cases of juvenile arthritis showing the diversity of disease course and disease outcomes for a population-based JCA cohort. The individuals showed a large variability of disease courses and had impaired health-related quality of life compared to a matched reference group. Sixty percent of the individuals were not in remission at the 17-year followup, and half experienced effects on physical function. Longterm outcome was best predicted by and associated with characteristics at the 5-year followup rather than by variables at onset and in the first years of disease. Hence these predictors are not early predictors and cannot provide guidance for early treatment of the disease. Some individuals were lost between the 5-year and the 17-year followup and we do not know the disease course after the 5-year followup for them. However, they did not differ significantly in the tested variables from individuals that participated in the 17-year followup, which implies that the study population was representative for a population-based unselected cohort of patients with JCA.
In our study the individuals followed for 17 years had a median age of 8.3 years at disease onset. This is about the same as in a study in northern Norway between 1985 and 1994: Moe, et al31 found median age at onset was 7.5 years; a more recent study in the Nordic countries found it was 6.8 years2. The subgroup distribution of 22% polyarticular-onset disease is also in accord with results from Berntson, et al2, and we believe this distribution is representative for an unselected population of patients with JCA in a Northern European setting.
At 5-year followup, 38% of the individuals were in remission. In a cohort of 185 patients with JRA, Selvaag, et al32 found 26.9% were in remission at 3-year followup, but those were partly referral patients and remission was defined as 6 months without medication. In a cohort of 47 patients with JCA in Costa Rica with followup after a median disease duration of 4.1 years, Arguedas, et al33 found half still had active or stable disease according to the EULAR criteria. Among the 55 patients who were examined radiographically at 5-year followup, 22% had changes. In a JRA cohort of 258 patients, Flatø, et al8 found 24% with erosions 6 years after diagnosis, but that cohort was referral-based and not population-based. We found no significant associations between radiographic changes at 5-year followup and outcome at 17-year followup, but that could be due to lower disease activity at 5-year followup among those not examined radiographically.
During the 17-year course, many individuals changed disease subgroup and stages of disease activity. Twenty-nine percent of the monoarticular and pauciarticular disease subgroups changed to the polyarticular subgroup, which corresponds to the oligoarticular-extended subgroup defined in the ILAR criteria. At 17-year followup, the subgroup with a polyarticular disease course was the largest, and the monoarticular disease-onset subgroup had lost the most individuals. Minden, et al6 found that about one-third of the patients with oligoarticular onset had polyarticular-extension disease after a median of 16.5 years, in a population- and referral-based cohort of 215 individuals with retrospectively determined JIA. In contrast, Koivuniemi, et al11 found no changes from the mono-arthritis/oligoarthritis subgroup to the polyarthritis subgroup in an 8-year followup, but their JCA cohort was small and there was a mean of 2.1 years between first symptoms and diagnosis.
At 17-year followup, 40% of the individuals in our study were in remission. This is in accord with findings from Minden, et al6, who found complete remission in 36% of a population-based cohort of 74 individuals with retrospectively determined JIA. In a hospital-based study of 683 patients with JCA, Fantini et al9 found that one-third were in remission after 11 years, whereas Zak, et al5 found that almost two-thirds were in remission after an average of 26.4 years in a referral-based cohort of 65 patients with JCA. The higher remission rate could be due to longer followup, but in a survey among a population-based cohort of 44 JRA cases with average followup of 25 years, Peterson, et al4 found that two-thirds reported evidence of active arthritis. Like Minden, et al6, we found no correlation between baseline variables and disease activity at the 17-year followup. However, our study has identified that remission at 17-year followup was associated with low disease activity duration index, low HAQ score, and remission at the 5-year followup. Although remission at 5-year followup was the most important variable for remission at 17-year followup, our study also showed that 39% of the individuals who were in remission at 5-year followup were not in remission at the 17-year followup. Flatø, et al8 found in a study of 268 JRA patients followed up after 15 years that half were in remission, but about one-fourth of them had had 1 or more periods of previous remission, and among the half in nonremission 74 out of 135 patients had had 1 or more previous periods of remission. They also found that young age at onset, DRB1*08, long duration of elevated ESR, and a large number of affected joints within the first 6 months were risk factors for nonremission. This was a larger cohort, but it consisted of referral cases admitted to a university hospital and the determination of remission was based on the ACR preliminary criteria14 with an increased time limit.
At the time the patients were included in this population-based longitudinal study, methotrexate and other more potent immunomodulatory drugs were not in frequent use or did not exist. Even at the 17-year followup, biologic therapies were not commonly used. The fact that very few individuals received early DMARD treatment and that those treatments consisted almost exclusively of hydroxychloroquine may contribute to the 5-year and 17-year outcomes34,35.
At 17-year followup, the median HAQ score was 0.0, with a range of 0.0–1.5; the score median was in accord with results from Minden, et al6, but in that study the range was broader (0.0–2.5). Packham and Hall7 found in a longterm followup (28 years) of 231 adults with persistent JIA that > 40% had severe disability (HAQ > 1.5). Flatø, et al36 found in a 9.7-year followup of 72 referral patients that 60% had no disability (CHAQ/HAQ = 0). They also found that persistent disease and polyarticular disease course during the first 5 years were associated with CHAQ/HAQ > 0 at followup. In our study, persistent disease during the first 5 years also was associated with HAQ > 0, but not with onset subgroup or disease course subgroup at 5-year followup. We found RF positivity was the most important predictor, but the confidence interval was broad because of few RF-positive patients. We found the Keitel functional test at 17-year followup revealed similar associations, but apart from being significantly associated with CHAQ, number of involved joints, RF positivity, and remission at 5-year followup, it was also significantly associated with number of joints with arthritis at 5-year followup, disease activity duration index after just 2 years of disease, and number of involved joints at baseline.
The SF-36 score at 17-year followup for the JCA cohort in our study was significantly lower compared to an age- and sex-matched normal population for all of the domains. In a referral cohort of 258 patient, 15 years after JRA diagnosis, Flatø, et al8 found poorer physical health than that in the controls according to the SF-36 subscales. In 82 patients with JIA from an adult rheumatology department database, Foster, et al10 found significantly worse scores for all the domains except physical relations and mental health, compared to a control group. In a cohort of 55 patients with JIA (median 8.7 yrs after symptom onset), Östlie, et al37 found the PCS of SF-36 was significantly lower compared to the general population, but there was no significant difference in the MCS. In our study we found that all the physical health domains were significantly associated with nonremission, functional disability according to HAQ, and KFT. In the mental domains there was a tendency for unfavorable scores for the individuals in nonremission and with functional disability, but there was a significant association only to the HAQ score, which could be due to the limited number of individuals. Östlie, et al37 also found that PCS and MCS data were significantly associated with HAQ scores.
Juvenile arthritis is a heterogeneous disease with a variety of disease courses during the first 17 years after onset. In our study of a population-based cohort diagnosed with JCA, many individuals also changed subgroup after 5 years of disease, and many individuals with early remission and remission at the 5-year followup were not in remission at the 17-year followup. At 17-year followup, 60% were in nonremission, almost half had some physical disability according to HAQ score and/or Keitel functional test, and the whole cohort had significantly lower health-related quality of life assessed by the SF-36 compared to an age- and sex-matched reference population. The outcome variables at 5-year followup were important predictors for outcome at 17-year followup. Because the most recent treatment strategies are more efficient, we can expect better longterm outcomes in the future, but further longitudinal studies are needed to confirm this assumption.
Acknowledgment
We are grateful to all patients participating in this study, and to Göran Kvist, Rheumatology Unit, Södra Älvsborg Hospital, Borås; Karin Svensson, Rheumatology Unit, Skaraborg Hospital, Skövde; and Dan Norberg, Rheumatology Unit, NU Hospital Group, Uddevalla, for assisting in organizing examinations at their units. We are also grateful to Frida Christiansson, Spenshult Hospital for Rheumatic Diseases, for her help with examinations; Maria Andersson, Research and Development Centre, Spenshult Hospital for Rheumatic Diseases, for help with laboratory procedures; and Birgitta Archenholtz, Sahlgrenska University Hospital, for advice on functional tests.
Footnotes
-
Supported by grants from The Health and Medical Care Executive Board of the Region Västra Götaland, Rune and Ulla Amlövs Foundation for Rheumatology Research, The Swedish National Rheumatism Association, The Rheumatism Association District of Gothenburg, The Medical Society of Gothenburg, the Region Västra Götaland (agreement for research and education of medical students between the Swedish Government and the university hospitals), and The Health and Medical Care Committee of the Regional Executive Board, Region Västra Götaland.
- Accepted for publication December 19, 2012.








{kind=link}
{kind=link}
{kind=link}