

Abstract
Objective. To determine the spectrum of manifestations in clinically important (i.e., requiring alterations of immunosuppressive therapy) psychiatric illness of pediatric systemic lupus erythematosus (pSLE) and to describe the laboratory and imaging features associated with psychiatric illness of pSLE (psySLE).
Methods. This was a single-center cohort study of patients with pSLE followed at a pediatric SLE clinic from August 1985 to July 2009. Patients with organic psychiatric disease due to SLE were included. Data regarding psychiatric features at initial presentation and during followup were obtained from psychiatry and rheumatology visits. Data regarding concomitant SLE disease activity and laboratory results were obtained from the institutional SLE database. Information from imaging studies was abstracted from patients' charts.
Results. Our cohort consisted of 53 pediatric patients (87% female) diagnosed with psySLE, representing 12% of the total pSLE cohort of 447 in the same time period. The median age at diagnosis of pSLE was 15.0 years and 16.1 years for psySLE. All patients reported symptoms of cognitive dysfunction and 75% of patients had additional psychotic features. Insight was preserved in 64% of patients with psychosis at diagnosis of psySLE. Visual distortion was observed among 32% of children with psySLE. Eighty-two percent of patients demonstrated clinical response to the institutional protocol of immunosuppression.
Conclusion. Cognitive dysfunction was present in all and additional psychosis present in 75% of pediatric patients with psySLE. Visual distortion and early preservation of insight were unique features of psychosis observed in this cohort of children/adolescents with psySLE.
Clinicians frequently recognize psychiatric manifestations of systemic lupus erythematosus (SLE). Before the establishment of the American College of Rheumatology (ACR) nomenclature for neuropsychiatric SLE (NPSLE)1, case reports and small case series had described some clinical features of psychiatric SLE (psySLE) in pediatric patients2,3,4. These studies noted that many patients with childhood psySLE had multiple features of cognitive impairment, mood disorders, and schizophreniform psychosis2. The more recent pediatric literature, using ACR nomenclature for central nervous system (CNS) involvement, reported that psychosis was a common NPSLE manifestation5,6,7,8,9. None of these studies had delineated the specific features of psySLE involvement nor reported the outcomes of patients with psySLE separately (from other non-psychiatric NPSLE manifestations). Only 2 small studies had focused exclusively on psySLE, to our knowledge3,10; therefore, specific information pertaining to this group of manifestations in patients with pSLE has been limited.
Cognitive dysfunction has been widely recognized as a feature of NPSLE. Cognitive dysfunction was defined by ACR NPSLE nomenclature as a deficit detected in any 1 domain (out of 8 commonly tested domains in neurocognitive testing) that represented a change from a premorbid status1. Although there was no standardized definition of neurocognitive impairment in patients with SLE before the ACR nomenclature definitions, earlier studies had used remarkably similar definitions to that subsequently defined by the ACR. When asymptomatic patients with adult-onset SLE (aSLE) were subjected to comprehensive neurocognitive testing, the prevalence of neurocognitive impairment had been reported to occur in up to 80%11,12,13. On followup retesting, however, the impairment remained stable or resolved in most patients14,15,16,17. These subclinical impairments did not predict subsequent development of clinically overt cognitive impairment nor adversely affect patients' health-related quality of life14,16,17,18,19. It is therefore not clear whether these impairments are clinically relevant. Similarly, nearly 60% of children without overt evidence of NPSLE met criteria for cognitive impairment when subjected to comprehensive neurocognitive testing20. Followup studies had not been reported in these asymptomatic patients with pSLE.
The aims of our large cohort study were to determine the spectrum of pSLE in children and adolescents requiring alteration of immunosuppressive therapy, and to describe the laboratory and imaging features of psychiatric illness in pSLE.
MATERIALS AND METHODS
Patients and design
Patients with psySLE were identified from our childhood SLE cohort, followed at The Hospital for Sick Children, Toronto, Canada, from August 1985 to July 2009. Patients were eligible for study if they (1) were < 18 years old at diagnosis of psySLE, (2) fulfilled at least 4 of the 11 classification criteria of SLE according to the ACR21, (3) had psychiatric illness as a manifestation of active SLE, and (4) had been treated and followed in our clinic during the study period. Patients were excluded if they had (1) preexistent primary psychiatric disorders unrelated to SLE, (2) transient reactive mood disorders after diagnosis of SLE (adjustment disorder)22, (3) steroid-induced psychosis23, or (4) coexistent neurodevelopmental disorders such that reliable assessment of their psychiatric status could not be carried out. Of 447 patients with pSLE followed in our clinic during the study time, 55 (12%) met inclusion criteria. Two of those patients were excluded: one had preexistent neurodevelopmental delay and was nonverbal and the other had Down syndrome; assessment of true deficit and response in these patients was difficult. None had steroid-induced psychosis. Fifty-three patients were included in our cohort study. The institutional research ethics board (REB 1000017883) approved our study.
Clinical features of SLE
Clinical data pertaining to demographics, SLE organ manifestations, disease activity [SLE Disease Activity Index (SLEDAI)24 and the European Consensus for Lupus Activity Measure (ECLAM)25], and laboratory data were obtained from the SLE database and verified with clinical charts as necessary.
We considered patients who were diagnosed with psySLE within 6 weeks from the date of diagnosis of SLE as having concurrent SLE and psySLE diagnoses. Patients were divided into 2 subgroups, (1) concurrent SLE and psySLE diagnoses and (2) initial SLE followed by psySLE diagnoses, for comparison purposes. For comparisons of coexistent non-psySLE disease activity, we presented a modified SLEDAI and ECLAM, without the contribution of psychiatric SLE items in the scores.
Assessment and classification of psychiatric illness of SLE
All patients in our clinic were screened specifically for cognitive (e.g., concentration, memory problems) or psychotic symptoms (e.g., hallucinations) during routine clinic visits. Psychiatric disorders of SLE were classified according to the ACR nomenclature for NPSLE with the exception of cognitive dysfunction and psychosis1. The ACR defined cognitive dysfunction based on formal neurocognitive testing. In our study, cognitive dysfunction was defined as severe self-reported or observed difficulties in concentration or memory that objectively, significantly impaired a patient's ability to perform academically. Although patients did not undergo an accepted battery of neurocognitive testing26, our psychiatrist (AL) formally, systematically evaluated cognitive function on all patients who reported psychiatric symptoms (including cognitive dysfunction). In all patients it was determined that the cognitive dysfunction was not due to fatigue or drug use and was out of proportion to that expected from mood disorders27. The Childhood Depression Inventory was performed on all patients. Although the ACR nomenclature for psychosis requires an absence of insight in the presence of hallucination or delusion, this was not necessarily true in patients with pSLE2. In fact, the ACR derived its criteria and case definition from the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) criteria for “psychotic disorder due to a general medical condition,” which does not require the absence of insight22. We therefore classified psychosis in this cohort in the same way. Patients must also have improved following SLE-specific treatment (i.e., immunosuppressive therapy).
Psychosis features include hallucinations and/or delusions22. Hallucinations referred to profound sensory distortions in a patient's perception of reality. These experiences occurred in the absence of a sensory input and may take on different modalities: visual, auditory, or tactile. Presence hallucinations referred to the sense of an undefined “presence” by the patient. Command hallucinations referred to hallucinations where the patient received a command to do something. Visual distortion referred to a change in shape or color of real objects. This could be static or the objects could seem to move. Delusions referred to false beliefs of external reality that were firmly sustained despite what everyone else believed and obvious evidence to the contrary.
We observed abnormal speech patterns. Word-finding difficulties were difficulties in naming items even though the patient knew the item. Word expression difficulties were difficulties in expressing words, or the patient felt “inhibited” such that they could not express the word describing an item.
Since 1987, one psychiatrist (AL) assessed > 90% of all our patients who had psychiatric manifestations. The recorded psychiatric features were thus internally standardized. The psychiatrist (AL) was consulted for adjudication where psychiatric notes were not explicit in classification of any patient — her assessment was taken as final verdict.
Laboratory and imaging features
Some of our patients were evaluated with lumbar puncture and/or CNS imaging at diagnosis. The indications for lumbar puncture and CNS imaging varied by year; the most common indication was to rule out other causes for symptoms, e.g., infection or space-occupying lesion. The reports of these investigations were obtained from patients' charts.
Statistical analysis
Summary statistics were computed. Medians and interquartile ranges (IQR) were reported for skewed variables, means and SD for normally distributed variables. Continuous variables were compared using the Student's t-test and categorical variables using chi-square test or Fisher's test as appropriate. All statistical analyses were performed using SAS version 9.2 (SAS Institute).
RESULTS
Clinical characteristics at diagnosis of SLE and psySLE
Demographics and clinical features at diagnosis of SLE for all patients in the cohort are presented in Table 1.
Basic demographics and clinical features at diagnosis of pediatric patients with systemic lupus erythematosus (SLE) and at diagnosis of patients with psychiatric SLE (psySLE).
The median time from diagnosis of pSLE to diagnosis of psySLE was 32 days (IQR 0–312 days). Seventy-seven percent of patients were diagnosed with psySLE within 1 year of the diagnosis of pSLE. The median time from initial psychiatric symptom to the diagnosis of psySLE was 60 days (IQR 21–217.5 days). Nine patients (17%) had psychiatric symptoms, predating diagnosis of SLE by > 6 months. Psychiatric illness was diagnosed concurrently (< 6 weeks) with the diagnosis of SLE in 27 (51%) patients (including the 9 patients with preceding psychiatric symptoms; Table 1). Two patients had no other active clinical features of SLE at the diagnosis of psySLE. Concomitant renal involvement, disease activity (without psySLE), and autoantibody profiles for the 2 groups of patients are presented in Table 1.
Classification of psychiatric illness of SLE
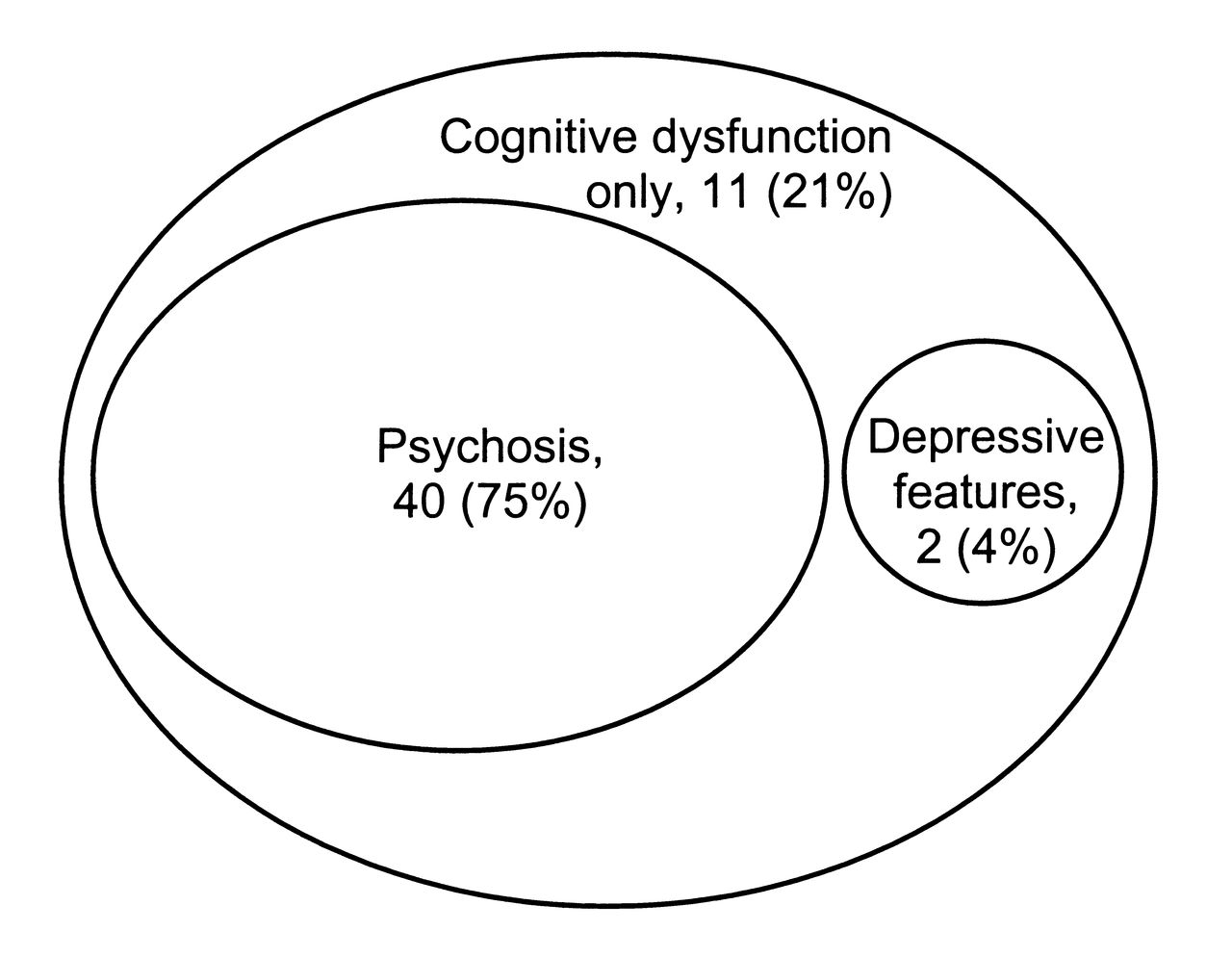
All our patients reported symptoms of cognitive dysfunction. In addition to the symptoms of cognitive dysfunction, 40 (75%) patients had features of psychosis (Figure 1). Acute confusional state was a presenting feature in 9 patients. When the acute confusional state improved, 7 patients had psychosis and 2 patients had cognitive dysfunction only and were classified accordingly. Although depressed mood was reported in 62% of the cohort (33 patients), none met criteria for major depressive disorder as defined by ACR/DSM-IV. Depression was associated with psychosis, preceded the diagnosis of SLE, or was triggered by social stressors in 31/33 cases. The other 2 patients showed prominent depressive symptoms in addition to cognitive dysfunction but did not satisfy criteria for major depression. Their cognitive dysfunctions were deemed to be out of proportion to their depressed mood. No patient met criteria for an anxiety disorder.

The spectrum of psychiatric entities among patients with psychiatric illness of systemic lupus erythematosus (SLE) in childhood. Based on a total population of 53 pediatric patients with psychiatric illness of SLE. All had cognitive dysfunction. Forty patients had additional psychosis features, 11 had only cognitive dysfunction, and 2 had prominent depressive mood disorder in addition to the cognitive dysfunction.
Psychiatric features of SLE
All patients had cognitive dysfunction. Concentration difficulties and decreased short-term memory were the most common symptoms reported. Forty (75%) patients had additional psychosis features, with hallucination the most prominent symptom (Table 2). Insight was preserved in the majority of these patients, with loss of insight generally seen only after prolonged symptoms.
Psychiatric and commonly associated neurological features in psychiatric disease of childhood systemic lupus erythematosus (SLE). Unless otherwise stated, percentages were calculated using the whole population of 53 patients.
Visual distortion was reported in 32% of patients. Speech difficulties were identified in 77%. Almost half of the patients reported photophobia and/or phonophobia with or without accompanying headache.
Eighteen (34%) patients reported suicidal ideations. Of these, 3 attempted suicide but were unsuccessful
Laboratory and imaging findings
Lumbar puncture (LP) was performed in 24 patients (45%) at diagnosis of psySLE. Nine of the 24 LP (36%) were abnormal; 7 (38%) patients had elevated total protein only, and 2 patients had both elevated white cells and total protein (both had cognitive dysfunction only). Elevated total protein only was observed in 1 patient with isolated cognitive dysfunction and 6 with psychosis. Opening pressure was found to be documented for only 7 patients and was elevated in 1 patient. None of the cerebrospinal fluid (CSF) cultures was positive for infection.
Forty patients underwent magnetic resonance imaging (MRI) at the time of diagnosis of psySLE. MRI was reported as normal in 50%, cerebral atrophy alone in 20% (8 patients), and white matter changes alone in 15% (6 patients). Two patients had both white matter changes and cerebral atrophy. One patient had a congenital structural aberration in addition to white matter changes and cerebral atrophy; 1 had mutiple cortical ischemic changes in bilateral occipital lobes; and 2 had incidental congenital structural aberrations.
Nineteen patients underwent both LP and MRI. Of these, 68% (13 out of 19) had at least 1 abnormal study of the 2 tests.
DISCUSSION
NPSLE in pSLE is reported to occur in 22% to 95% of patients and involvement may range from peripheral neuropathy to frank psychosis3,4,6,7,8,9,28. Previous studies in pSLE had not focused on psychiatric manifestations4,7,8,9,28 or focused only on a specific manifestation such as psychosis10. A case series of 10 patients reported on a larger spectrum of psychiatric involvement in pSLE but did not specifically address clinically important cognitive dysfunction3. Of the largest cohort of patients with psychiatric illness of pSLE to date, we presented details of the full spectrum of clinical features in psySLE and classified this cohort according to definitions set out in the ACR/DSM-IV nomenclature1,22.
Hallucination was the most common psychosis feature in our patients. The ACR nomenclature glossary for the definition of psychosis requires that hallucinating patients not have insight. However, the ACR criteria also stated that it was based on the DSM-IV definition of “psychosis due to a general medical condition”1; the DSM-IV does not require loss of insight to diagnose “psychosis due to a medical condition.” Insight is a fluctuating feature and a marker of severe psychiatric disease. It may indeed be retained in early and mild stages of psychosis. In our study, 64% of the patients retained insight even in the presence of vivid hallucinations. Insight was observed to be lost in cases in which the hallucinations were prolonged. Our findings are similar to a previous pediatric report that described the preservation of insight in pSLE patients with active visual hallucinations2. It is also possible that early preservation of insight may be a unique feature of pSLE, in contrast to aSLE. The ACR nomenclature for psychosis may need to be modified for use in the pSLE population — as the DSM-IV was, for the pediatric population. We suggest that it is important that clinicians be aware that hallucinations can occur despite full insight in pSLE, and that as patients may not report these symptoms voluntarily, diagnosis could be delayed.
In our study, the first to describe in detail the features of psySLE in childhood, we found a previously unreported feature of visual distortion in 32%. Patients with visual distortions perceived objects to change shape and color, and/or to move. A few patients had a special version of this that we have termed “slinky,” where an object was perceived to lengthen and extend outward toward the patient and then retract to its original form. This has not been observed in patients with primary psychiatric disorders and may be a useful feature to inquire when assessing children/adolescents for psySLE.
Suicidal ideation occurred in one-third of patients, with 6% of the cohort having attempted suicide (20% of patients with suicidal ideation). Although no previous pediatric study had reported on suicide in SLE, one adult SLE study reported that 2% of patients with SLE attempted suicide29. All of those who attempted suicide had features of NPSLE, including overt cognitive dysfunction and depressed mood before the suicide attempt29. When interviewed prospectively, 8% to 34% of adult patients with SLE (including patients with no primary psychiatric diagnosis or NPSLE) reported suicidal ideation30,31,32. Because we found that a significant proportion of children with psySLE had suicidal ideation and did attempt suicide, we suggest that rheumatologists be aware of this and assess each pediatric patient with psySLE for suicide risk.
In our study, we focused on patients with cognitive dysfunction requiring treatment with immunosuppressive therapy. Because the focus of our study was to detect this type of impairment, we cannot address the issue of clinical relevance of asymptomatic abnormalities detected by formal neurocognitive testing as suggested by studies in adults with SLE33. Indeed, the relevance of using the ACR criteria to detect defects requiring change in immunosuppressive therapy has been questioned. The 2010 European League Against Rheumatism (EULAR) recommendations for management of SLE with neurologic manifestations stated that cognitive dysfunction in most patients had a benign course, while severe cognitive dysfunction requiring treatment occurred in only 3%–5% of patients with aSLE34. This same approach was also used by the Systemic Lupus International Collaborating Clinics group in its NPSLE studies, in which only clinically overt and relevant cognitive dysfunction as assessed by physicians was included35,36. All the patients in our study had objective evidence of cognitive dysfunction: they all had significant decrease in school performance. In addition, we also required our patients with cognitive dysfunction to demonstrate improvement following immunosuppressive treatment as confirmation that the observed cognitive dysfunction was indeed due to psySLE. The proportion of patients with cognitive dysfunction was similar to studies in which clinically overt cognitive dysfunction had been reported, including a recent metaanalysis7,37,38,39.
Although the ACR nomenclature recognized 5 discrete psychiatric entities1, we found a more limited spectrum of entities in this cohort. Cognitive dysfunction and psychosis were the 2 entities most commonly observed4,6,8,9,28,38. After excluding social stressors and preexisting mood disorders, only 2 patients satisfied the criteria for mood disorder with depressive features. Those 2 patients also had very prominent cognitive dysfunction symptoms, similar to a previous study27. In our population of predominantly female adolescents, it was unsurprising that mood disorders secondary to adjustment difficulties and social stressors were common.
We observed a number of other neurological complaints associated with psySLE: speech difficulties, persistent headaches, photophobia, phonophobia, and significant sleep disturbances (insomnia/hypersomnolence). Although headaches are a common feature in pSLE, the headaches seen in patients with psySLE tended to be more severe and persistent than the headaches seen in up to 70% of patients with pSLE7. Because patients may dismiss mild symptoms of cognitive dysfunction and not report hallucinations and visual distortions, direct questioning may be necessary to detect these symptoms.
Similar to previous studies, a CSF abnormality was present in only 37.5% and a normal CSF examination does not exclude the presence of psySLE3,10,23,40. Similarly, only 50% of the MRI scans were abnormal, with cerebral atrophy and white matter abnormalities the most common abnormal findings. These MRI findings are similar to previous reports, in which abnormalities were seen in 11% to 70% of patients3,10,23,40. Our findings agree with the 2010 EULAR recommendations for management of NPSLE that CSF and MRI examination were only modestly sensitive and specific (MRI only) for psySLE34.
Our study has limitations. Because this was a clinically defined cohort of patients and not part of a prospective study, routine neurocognitive testing was not performed. While it is a gold standard for diagnosing cognitive deficits and delineating the specific domains affected, neurocognitive testing detects subclinical deficits in asymptomatic patients with SLE. Because the study population consisted of children and adolescents still in school, we used significant decline in school performance without any other explanation as an external objective measure to substantiate subjective cognitive symptoms. Since we conducted our study, the Childhood Arthritis and Rheumatology Research Alliance (CARRA) has proposed a framework to standardize neurocognitive assessment in patients with pSLE41. CARRA studies are now under way to find a valid and accessible means of assessing neurocognitive function in clinical settings among patients with pSLE.
We described clinical features of psySLE in patients with pSLE. All patients had cognitive dysfunction. Hallucinations were common, but insight was preserved in the majority of patients with pSLE — a unique feature in psySLE of childhood. Although not previously reported, visual distortions were prominent and were often reported by children with psySLE. While the ACR nomenclature serves an important purpose in standardizing terminologies for researchers studying NPSLE, we found that the nature of the psychosis seen in pSLE was different from that observed in aSLE. Because insight was preserved in the majority of our pSLE patients with psychosis early in their disease course, strict adherence to the ACR definitions could delay appropriate treatment of these patients. Rheumatologists caring for patients with pSLE should still consider the possibility of psychosis secondary to SLE in the presence of insight, so that treatment could then be instituted in a timely manner. Finally, suicidal ideation and attempted suicides were not uncommon in this population; suicide risk should thus be assessed in all these patients.
Acknowledgment
Dr. Silverman holds the Ho Family Chair in Autoimmune Diseases. Dr. Lim was supported by the Peterborough KM Hunter Graduate Studentship, the Joseph M. West Family Memorial Scholarship, the Eddie Steinberg Scholarship Fund, and the Chrisholm Memorial Fellowship
- Accepted for publication September 27, 2012.








{kind=link}