

Abstract
Objective. We investigated the clinical characteristics, potential difficulties in diagnosis, and therapy for coronary artery involvement in patients with Takayasu arteritis (TA).
Methods. Of 587 consecutive patients hospitalized with TA from 1998 to 2011, those found to have > 50% reduction of diameter of coronary artery by angiography were recruited. We defined the first finding of coronary involvement as baseline. The clinical features, laboratory data, coronary angiographic findings, treatment, and followup outcomes were summarized retrospectively.
Results. A total of 45 (7.7%, 45/587) patients with coronary involvement were identified, including 40 with typical angina, and 15 with myocardial infarction. Some had complications such as peripheral vascular murmur, pulseless disease, and hypertension. The average age at onset of cardiac symptoms was 40.3 ± 12.8 years (range 15–64) and 36 were female. At admission, erythrocyte sedimentation rates were elevated in 27 patients (60%) and C-reactive protein levels in 23 (51.1%). The ostia (37.4%) and proximal segments (33.3%) of coronary artery were most frequently involved. The treatment was stent implantation in 10 patients and coronary artery bypass grafting in 13. One female patient suffered sudden death during the angiography. During a mean followup of 5.8 ± 4.5 years, 8 patients died.
Conclusion. Coronary artery involvement in TA that leads to cardiovascular events, especially to cardiovascular death, is not rare. Early diagnosis and therapy should be emphasized.
Takayasu arteritis (TA) is a chronic large-vessel vasculitis of unknown etiology that mainly affects the aorta and its major branches, resulting in luminal stenosis and aneurysmal changes in the large vessels1. Adolescent girls and women in their second and third decades of life are at highest risk. This inflammatory arteritis is characterized by histopathology changes including adventitial thickening, focal leukocytic infiltration of media, and intimal proliferation2.
Coronary involvement in TA is not rare, as first described by Frovig and Loken3 in 1951, and coronary artery bypass grafting (CABG) was first performed in TA patients by Young and colleagues4 in 1973. Coronary artery involvement is detected in 10% to 30% of cases of TA5.
We evaluated clinical, laboratory, radiographic, and followup data from 45 patients with TA to determine potential difficulties of diagnosis and therapy of coronary involvement.
MATERIALS AND METHODS
Among a cohort of 587 patients hospitalized with TA in Fuwai Cardiovascular Hospital from 1998 to 2011, we evaluated 45 patients who were identified with coronary artery involvement determined by angiography. We defined the first finding of coronary involvement as baseline. Medical records including clinical, laboratory, radiographic, and followup data were analyzed retrospectively. The study protocol was approved by the local ethics committee.
Diagnostic criteria
The diagnosis of TA followed the American College of Rheumatology 1990 criteria6: age at disease onset ≤ 40 years; claudication of extremities; decreased brachial artery pulse; blood pressure difference > 10 mm Hg; bruits over subclavian arteries or aorta; and arteriographic abnormality. A patient was diagnosed with TA if at least 3 of these 6 criteria were present.
Anatomic classification criteria
Classification of TA was defined according to the anatomic criteria, as follows: Type I: arteritis affecting the aortic arch and its major branches; Type II: arteritis affecting the thoracic/abdominal aorta; Type III: arteritis affecting the entire aorta; and Type IV: arteritis affecting the pulmonary artery.
Coronary angiography
Abnormal coronary angiographic findings were defined as stenosis > 50%, coronary aneurysm, and ectasia.
Statistical methods
Statistical data were analyzed using SPSS version 19.0. The comparisons of data between the study groups were performed using an independent t test and chi-square test where appropriate. P values < 0.05 were considered statistically significant.
RESULTS
A total of 45 patients with coronary artery involvement were enrolled for study, from 1998 to March 2012, accounting for 7.7% of hospitalized patients in the same period with a diagnosis of TA. The cohort consisted of 36 women and 9 men, aged 43.5 ± 13.5 years (range 15–70 yrs). The average age at onset of cardiac symptoms was 40.3 ± 12.8 years (range 15–64 yrs), and 51.1% of patients presented at age 40 years or younger. Mean age at onset of TA was 27.5 ± 10.7 years (range 6–50 yrs).
Clinical features (Table 1)
Among the 45 patients, 40 (88.9%) had typical angina, which was the most common presenting problem, and 15 had a history of myocardial infarction. Among the 15 patients, 11 presented as acute myocardial infarction, and one suffered myocardial infarction twice. Cardiac onset presented as the first symptom of TA in 11 patients (10 cases of angina, 1 acute myocardial infarction). Age at onset of cardiac symptoms of these patients was significantly younger than among the other 34, 28.4 ± 10.1 versus 44.1 ± 10.9 years, respectively (p < 0.001). Three patients had no cardiac symptoms at onset, but ST-T ischemic changes and pathologic Q wave results from electrocardiography and angiography demonstrated coronary artery stenosis > 50%. In addition, heart failure was noted in 11 patients (24.4%).
Clinical symptoms and signs.
The other clinical manifestations included hypertension (n = 24), pulseless disease (n = 24), peripheral vascular murmur (n = 32), dizziness or syncope (n = 15), and heart murmur (n = 12). Most patients lacked the risk factors of atherosclerosis. Three patients also experienced hyperlipidemia, and 3 diabetes mellitus. Seven patients had a history of smoking and 3 a history of alcohol consumption.
Classification of TA
Thirty-seven of the 45 patients were diagnosed by computed tomography angiography (CTA) and 8 by magnetic resonance angiography (MRA). Based on the angiography findings, 15 patients had Type I arteritis, 7 had Type II, 19 had Type III, 2 had Type I + IV, and 2 had Type III + IV.
Laboratory findings
At time of presentation of coronary artery disease, the mean erythrocyte sedimentation rate (ESR) was 27.8 ± 23.6 mm/h (reference value < 15 mm/h in men and < 20 mm/h in women) and mean C-reactive protein (CRP) was 12.5 ± 14.6 mg/l (reference value 0–8 mg/l). ESR and CRP values were elevated in 27 (60%) and 23 patients (51.1%), respectively.
ST-T ischemic changes and pathologic Q wave findings were recorded in 35 and 18 patients, respectively, by electrocardiogram. Echocardiographic examination suggested that segmental left ventricular wall motion abnormality was present in 10 patients. Left ventricular enlargement was noted in 11 patients. Left ventricular ejection fraction (LVEF) ranged from 30% to 80% and LVEF < 50% was noted in 8 patients.
Coronary angiography findings (Table 2)
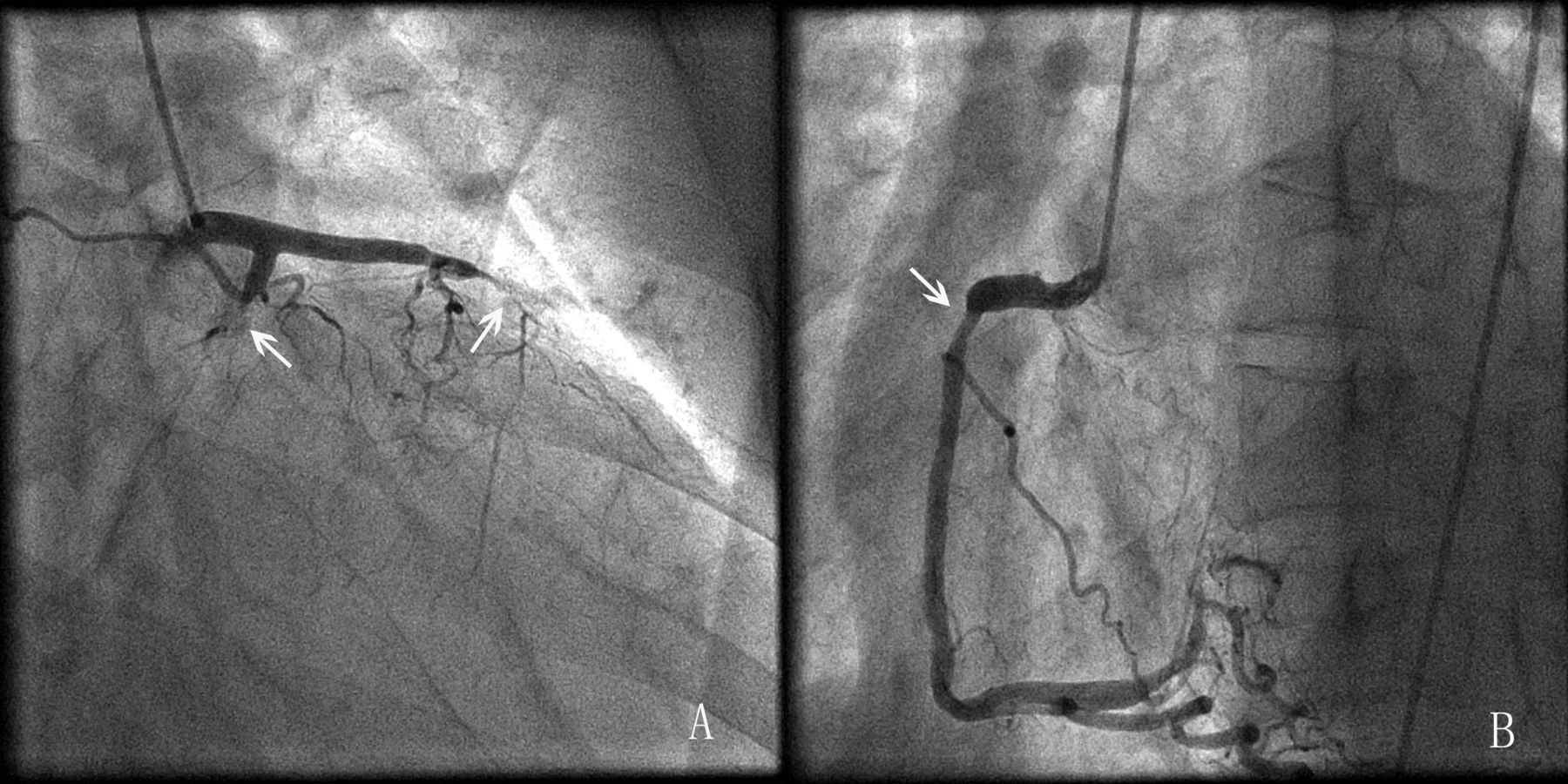
All 45 patients underwent coronary angiography (Figures 1 and 2), and a total of 99 coronary lesions were identified. The ostia and proximal segments of coronary artery were most frequently involved. Thirty-seven lesions of ostial coronary artery were found in 29 patients, of which 14 involved the left main coronary (LM), 4 the left anterior descending coronary (LAD), 5 the left circumflex coronary (LCX), and 14 the right coronary artery (RCA). Among the ostial lesions, there were 7 lesions of occlusion and 17 of narrowing > 90%. Thirty-three proximal lesions of coronary artery were found in 22 patients, of which 5 involved LM, 16 LAD, 5 LCX, and 7 the RCA. Seventeen and 12 lesions in the middle and distal segments of coronary artery were found in 8 and 11 patients, respectively, and 1 patient had involvement of only the middle segment of LAD.
Coronary angiographic findings.

Angiograms of a 25-year-old man with Takayasu arteritis who presented with chest pain and hypertension. Arrows show significant stenosis of the left main coronary artery (A) and right coronary arteries (B).
Angiograms of a 28-year-old woman with coronary artery involvement in Takayasu arteritis. Arrows show significant stenosis or occlusion of left anterior descending coronary (A), left circumflex coronary (A), and right coronary arteries (B).
LM lesion was noted in 23 patients (51.1%), of which 9 cases had only LM involvement with significant lesions such that narrowing of the lumen was > 80%. Twenty-two patients (48.9%) were diagnosed with single coronary artery disease, which was the most common condition in our study, 11 (24.4%) patients with bilateral coronary artery disease, and 12 (26.7%) patients with triple coronary artery disease.
Therapy
Therapeutic strategies included both medical treatment and revascularization. One patient, with stenosis of 95% in the ostia of LM and RCA, underwent sudden death during coronary angiography. Twenty-four patients underwent coronary revascularization. Percutaneous coronary intervention was performed in 10 patients.
Thirteen patients underwent CABG. Twenty patients received conservative treatment. Of 16 patients undergoing peripheral vascular revascularization, 7 received stent implant, 7 underwent percutaneous balloon dilatation, and 2 received artificial vessel grafts. Glucocorticoids (prednisone) were administered to 31 patients with active disease. Prednisone was started at a daily dose of 30 mg for 1 month, and then tapered according to a maintenance dose of 10 mg by 6 months. Oral Tripterygium wilfordii, a Chinese traditional herb widely used in treatment of autoimmune and inflammatory diseases, was added to glucocorticoids in 3 patients who were unresponsive after 1 month to glucocorticoids alone. No other immunosuppressive agents or biologics were used in any patients.
Patient outcomes (Table 3)
After discharge from hospital, 44 patients were followed for 5.8 ± 4.5 years (range 0.4–27.1 yrs). Six patients were lost during followup. A total of 9 patients (20%; 9/45) died and 8 died during the followup period. Among the causes of death, 1 patient experienced sudden death during coronary angiography, 3 patients had received stents, 1 had received CABG, and 4 had received only medical therapy. The causes of death included complications of acute myocardial infarction in 3, heart failure in 3, brain trauma in 1, and sudden cardiac death in 1 patient.
Prognosis of 3 methods of therapy.
One patient who experienced CABG (3 arterial grafts) suffered a perioperative myocardial infarction, and coronary angiography revealed that ostial anastomosis of 2 arterial grafts led to occlusion. Three patients complained of angina frequently for uncontrolled inflammation activity, although they had received longterm glucocorticoid therapy. In March 2012, heart transplant surgery was performed in 1 female patient who had had repeated heart failure.
DISCUSSION
TA is a chronic vasculitis affecting primarily women (in 80% to 90% of cases), appearing at a relatively young age, usually between age 10 and 40 years7. The average age at onset of cardiac symptoms in patients we studied was 40.3 years, and the majority of patients reported typical cardiac symptoms. To our knowledge women of this age with coronary disease are very rare, which may easily lead to a missed diagnosis. If young patients with peripheral artery disease, especially women, complain of recurrent chest pain, a physician should be alert to the possibility of TA involving the coronary vessel.
The incidence of coronary involvement in TA is relatively low, but not rare. According to our results, the incidence is 7.7%. Endo, et al8 described 130 patients with a diagnosis of TA, and detected 31 patients with coronary involvement. However, not all patients with TA underwent coronary angiography, which may have resulted in some individuals with coronary involvement being overlooked. Therefore, the incidence may be higher than reported.
On the basis of pathological features, the following 3 types of coronary lesions can be distinguished: type 1, stenosis or occlusion of the coronary ostia and proximal segments of the coronary arteries; type 2, diffuse or focal coronary arteritis, which may extend diffusely to all epicardial branches or may involve focal segments, the so-called skip lesions; and type 3, coronary aneurysms. Type 1 lesion is detected most frequently. Narrowing of coronary arteries develops mainly because of extension of the inflammatory processes of proliferation of the intima, and owing to contraction of the fibrotic media and adventitia from the ascending aorta9. Accelerated atherosclerosis caused by vascular inflammation may be another explanation of coronary lesions10. Ostial and proximal lesions were the most common findings (> 70%) in our study, similar to results described by Matsubara and colleagues9. However, our results suggested that lesions of middle and distal segments were not rare and were usually associated with ostial or proximal lesions. Only 1 patient had a lesion of the middle segment of LAD, with no other coronary involvement. Coronary aneurysms were not detected.
Coronary involvement in TA is always associated with peripheral artery disease7. Isolated coronary involvement is very rare, probably appearing in fewer than 5% of cases11,12,13, which may make clinical diagnosis difficult. TA with coronary involvement and TA combined with coronary atherosclerotic disease (CAD) can be identified as follows. First, the cardiac symptoms of TA with coronary artery involvement always appear at a relatively younger age than TA combined with CAD, and disease is more common in women. Second, angiography results suggest that the ostial and proximal lesions are involved most frequently in patients with TA involving coronary artery. Third, patients with TA-involved coronary artery do not demonstrate risk factors for atherosclerosis, a situation that is different from TA combined with CAD.
In this disease, ischemia caused by coronary lesions is one of the major causes of death. It is ideally necessary to make a diagnosis in the early phase, especially in the pre-stenotic phase. However, there is always a delay of several months or years before diagnosis in cases of TA, even in patients with diminished or absent pulse14,15,16. Angiography remains the gold standard for diagnosis. To avoid delays in diagnosis and treatment, early coronary CTA or intracoronary angiography should be performed in patients in whom there is clinical suspicion of coronary artery involvement in TA. Coronary lesions involved in TA were often located in the ostia, and stenosis can be very serious. It is noteworthy that improper performance of the angiography process may lead to sudden death as in a female patient reported in our study.
The prognosis of patients with coronary involvement who have received conservative treatment is often poor, and many have died of cardiac events17. Therefore revascularization should be undertaken promptly. The timing of operations should be avoided during the active stage of inflammation in TA. To avoid cardiac accidents, however, revascularization must be performed without delay when patients have unstable angina; corticosteroid or immunesuppressive therapy should be administered at the same time18.
The optimal revascularization method for TA involving coronary artery has not been determined. According to a 10-year followup study8, the actual survival rates and cardiac event-free rates at 10 years were 81.4% ± 8.4% and 72.6% ± 9.6%, respectively. When CABG is performed, the type of grafts and site of proximal anastomosis should be selected carefully19. Because subclavian arteries and internal thoracic arteries may be involved in inflammation, saphenous vein grafts could be a better choice. A report on an American cohort of 75 patients with TA who underwent peripheral revascularization demonstrated that recurrent stenoses occurred in 78% of the angioplasties and in 36% of the surgical procedures20. To our knowledge, there are no reports of results of coronary stenting for TA even in a small group of patients. According to our data, there was a higher mortality in patients who had percutaneous procedures compared to CABG. However, recent developments of drug-eluting stents resulted in a better patency rate than bare-metal stents21,22,23, thus offering a different potential strategy for revascularization.
Our study has some limitations. It was a retrospective design, and patients undergoing revascularization were not randomized. Six patients were lost to followup, a development that may lead to an underestimation of mortality.
Coronary artery involvement in TA is not rare, and patients are predominantly young women. Inflammation can affect all parts of coronary artery, although ostial or proximal lesions are especially prevalent. Myocardial ischemia can be the major cause of death. Prompt and correct diagnosis and treatment should be the goal because of the poor prognosis. In addition, revascularization is strongly recommended in these patients.
- Accepted for publication December 19, 2012.








{kind=link}
{kind=link}