

Abstract
Objective. The Disease Activity Score-28-C-reactive Protein 4 [DAS28-CRP(4)] composite measure for rheumatoid arthritis (RA) is based on 4 variables: tender and swollen joint counts, CRP, and patient global assessment. DAS28-CRP(3) includes only 3 variables, because patient global assessment has been omitted. Thresholds for low and high disease activity are the same for the 2 scores. The objective of our study was to compare the 2 DAS scores and their responses on the individual patient level.
Methods. Baseline and 12-week disease activity data from 239 patients with RA treated with a biological agent were extracted from the Danish registry for biological treatment (DANBIO). Cohen's effect sizes (ES) and disease activity levels according to the DAS thresholds were assessed. The Bland-Altman method was used to examine the bias between the DAS scores and the 95% limits of agreement (LoA).
Results. Baseline values for DAS28-CRP(4) and DAS28-CRP(3) were 4.8 ± 1.2 and 4.6 ± 1.1, respectively. At 12 weeks, DAS28-CRP(4) had improved by −1.39 ± 1.34 (p < 0.0001). At that timepoint the bias of DAS28-CRP(3) was −0.07 (LoA −0.69, 0.55) (p < 0.0001). The bias of the DAS28-CRP(3) response was +0.21 (LoA −0.49, 0.91) (p < 0.0001). ES for DAS28-CRP(4) was 1.2 ± 1.1 versus 1.1 ± 1.1 for DAS28-CRP(3) (p < 0.0001). Compared to DAS28-CRP(4), DAS28-CRP(3) categorized 33% fewer patients as having a high level of disease activity, 8% fewer patients as good responders, and 12% more patients as nonresponders.
Conclusion. Mean values of DAS28-CRP(4) and DAS28-CRP(3) agreed well, but in the individual patient the difference between the scores and their responses may be substantial.
The Disease Activity Score (DAS) is a composite measure of disease activity in rheumatoid arthritis (RA). The original DAS was based on an equation that incorporated weighted values of the Richie Articular Index, a swollen joint count (based on a 44-joint count), erythrocyte sedimentation rate (ESR), and patient global assessment (PGA)1,2. The need for a more practical score led to the development of the DAS28, with tender and swollen 28-joint counts replacing the Richie Articular Index and the 44-joint count3,4. Further modifications have substituted C-reactive protein (CRP) measurements for ESR and have substituted constant values in place of PGA5,6. The DAS28 has a continuous scale ranging from 0 to 9.4, and usually shows a Gaussian distribution in RA populations7. A DAS28 score > 5.1 implies active disease, ≤ 3.2 well-controlled disease, and < 2.6 minimal disease activity (previously termed remission)7,8,9. The DAS and DAS28 have also provided the basis for the European League Against Rheumatism (EULAR) response criteria. These criteria classify individual patients as non-, moderate, or good responders, depending on the extent of change and the level of disease activity achieved. Thresholds for improvements are ≤ 0.6 and ≤ 1.210.
Although the DAS and the DAS28 were developed in cohorts of patients with early RA, both scores have been found to be valid in cohorts of patients with more longstanding RA and to perform comparably to the American College of Rheumatology (ACR) criteria for improvement in clinical trials11. Moreover, DAS-driven therapy has been shown to improve clinical outcome and possibly the suppression of joint damage progression compared to routine care12. Since its development, the DAS28 has been widely used as an outcome measure in therapeutic trials13. The DAS28 is also frequently used in clinical practice to assess and monitor the disease activity of patients with RA14. However, because 7 different versions of the DAS are accessible8, it has been critically commented that the many versions may lead to confusion and improper use of the DAS in daily clinic15. Little or no consensus exists regarding the most appropriate version of the DAS.
DAS28 based on CRP (DAS28-CRP) may be calculated using 3 or 4 variables. DAS28-CRP(4) is computed using 4 variables: swollen and tender joint counts (SJC and TJC), CRP, and PGA. DAS28-CRP(3) comprises only SJC, TJC, and CRP8. Although thresholds for low and high disease activity and for improvements are the same for the 2 scores8, data from the Danish registry for biological treatment in rheumatology, DANBIO, have shown that DAS28-CRP(3) in comparison with DAS28-CRP(4) on average underestimates disease activity in patients just before biological treatment is initiated16. The 2 DAS scores and their responsiveness have not yet been compared in patients undergoing biological treatment. The aim of the study was to compare these 2 DAS scores regarding sensitivity to change and to assess the agreement between the scores and their changes on group and subject level after initiation of biological treatment, based on registry data from the daily clinic.
MATERIALS AND METHODS
Patients, disease activity measures, and DAS28-CRP calculations
Baseline and 12-week data from 239 patients with RA followed during their first course of biological treatment were extracted from DANBIO17. DANBIO was approved by the Danish Data Registry in 2000 (registrations 2007-58-0014 and 2007-58-0006) and has served as a national quality registry of the National Board of Health since 2006 (no. 7-201-03-12/1). Only data from patients receiving standard dosages and who had received at least 1 infusion or injection were included. In cases of withdrawal or missing data, the observation closest to 12 weeks was chosen for analysis. Based on expert opinion, all patients had failed treatment with at least 1 synthetic disease-modifying antirheumatic drug (DMARD) and had been selected for biological treatment after consensus of senior staff physicians. Data on SJC, TJC, CRP, physician global assessment (PHGA), PGA of disease activity, and Health Assessment Questionnaire (HAQ) score were available in the database. The Clinical Disease Activity Index (CDAI) and Simplified Disease Activity Index (SDAI) were assessed. Remission thresholds were defined as ≤ 2.8 and ≤ 3.3, respectively18.
DAS28-CRP(4) and DAS28-CRP(3) were calculated according to the DAS Website8:
where TJC28: 28-tender joint count; SJC28: 28-swollen joint count; and PGA: patient global assessment on a 100-mm visual analog scale.
Patients with DAS28 improvements ≤ 0.6 were considered nonresponders and those with DAS28 > 1.2 good responders. Negative changes in DAS28 correspond to improvements.
According to Danish law, informed consent and ethical approval were not required.
Statistics
Data are given as mean ± SD. Differences between the DAS28-CRP(4) and DAS28-CRP(3) scores were assessed by Student's t test. Bland-Altman plots were used to show the differences between the paired scores plotted against the mean of the scores. Limits of agreement (LoA) were estimated as the mean difference between paired measurements (the bias) ± 1.96 SD, where SD was the standard deviation of all the paired differences. Thus 95% of the differences would lie between these limits19,20; 95% CI around the bias and the agreement limits were calculated19. Associations between pairs of variables were characterized by Pearson's r data. Linear regression analyses were used to assess prediction intervals and standard errors of estimations for these associations. Multiple linear regression analyses (stepwise selection) were used to study the predictability of DAS28-CRP(3) and DAS28-CRP(4) responses by changes in SJC, TJC, CRP, PHGA, PGA, and HAQ score as independent variables. Multiple squared correlation coefficients (R2), partial standardized regression coefficients (beta), and partial correlation coefficients (rp) were derived from the analyses. Sensitivity to change of the DAS scores was characterized by Cohen's effect size (ES) calculated as mean DAS change/SD baseline21 and the standardized response mean (SRM) calculated as mean DAS change/SD change22. To allow statistical comparison of ES for DAS28-CRP(4) and DAS28-CRP(3), ES was also calculated for each individual patient as ESi = DAS changei/SDi baseline, where i = individual. ES and SRM can be seen as signal-to-noise ratios. Higher values of ES and SRM point to better sensitivity to change or responsiveness of a particular measure. There is no consensus whether ES or SRM is the better responsiveness statistic22. Cohen's ES > 0.8 is considered large, < 0.2 is considered small21. Calculations were performed using SPSS/PC+ Statistics V. 4.01. Two-tailed p values < 0.05 were considered statistically significant.
RESULTS
Mean age of the patients was 56.5 ± 13.8 years and female/male ratio was 181/58. One hundred thirty-two patients (55%) were treated with infliximab, 48 (20%) with adalimumab, 28 (12%) with etanercept, 16 (7%) with rituximab, and 15 (6%) with another biological agent. All patients received combination therapy with methotrexate or another DMARD. Mean followup was 12 ± 4 weeks (median 13 wks, range 2–18 wks).
Results for DAS28-CRP(4), DAS28-CRP(3), and single measures of disease activity at baseline and at 12 weeks, and the corresponding improvements and effect sizes, are given in Table 1. Baseline and followup values for CDAI were 25.3 ± 11.5 and 12.4 ± 9.5, respectively, (p < 0.0001) and for SDAI 28.0 ± 12.9 and 13.8 ± 10.4 (p < 0.0001). Results of Bland-Altman analyses of the agreement between the 2 DAS indices and between their changes after 12 weeks are shown in Table 2 and Figure 1. The degree of agreement between the indices at baseline was previously analyzed in detail for a larger sample of DANBIO patients (n = 319)16.
Characteristics of 239 patients with rheumatoid arthritis selected for biological treatment (data are mean ± SD).
Agreement between DAS28-CRP(4) and DAS28-CRP(3) and between their responses in 239 patients with RA 12 weeks after initiating biological treatment. Bias and lower and upper limits of agreement are shown.

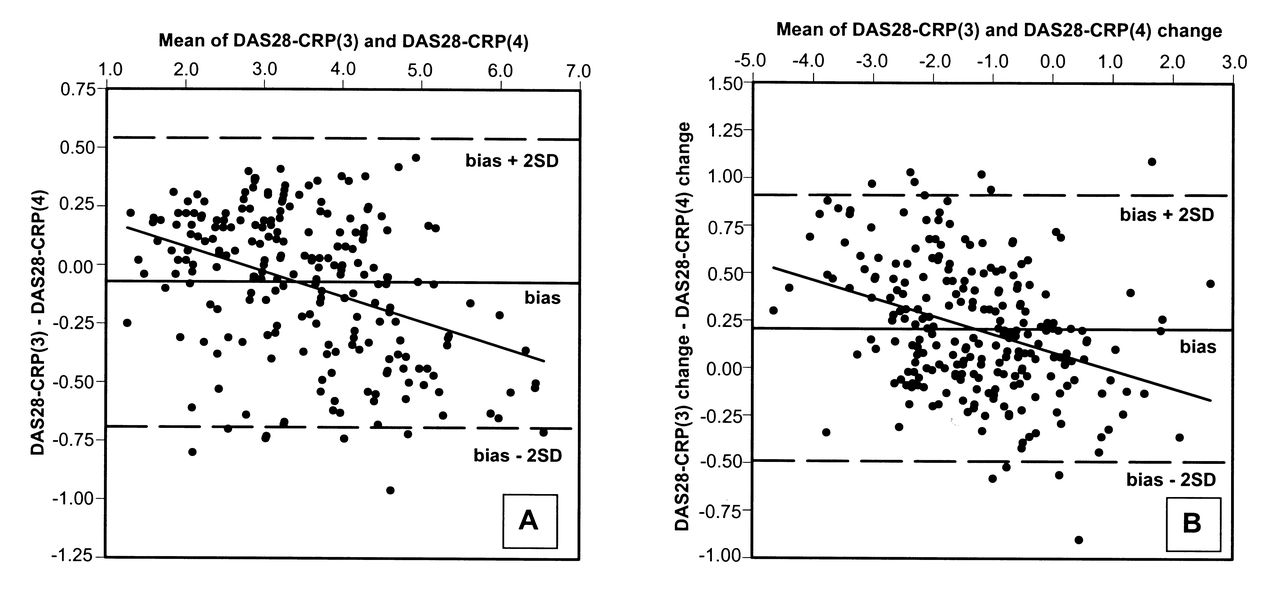
Bland-Altman plots comparing (A) Disease Activity Score-28-C-reactive Protein 3 [DAS28-CRP(3)] and DAS28-CRP(4) and (B) change in DAS28-CRP(3) and DAS28-CRP(4) 12 weeks after start of biological treatment. Bias is illustrated by a solid line and the upper and lower limit of agreement (bias ± 2 × SD) by broken lines. The regression line is also shown. The regression equation, standard error of estimate (SEE), and correlation coefficient (r) for (A): y = −0.11x + 0.29, SEE = 0.28, r = −0.40, p < 0.0001; and for (B): y = −0.09x + 0.08, SEE = 0.33, r = −0.35, p < 0.0001.
The mean DAS28-CRP(4) at baseline was 4.8 ± 1.2 versus 4.6 ± 1.1 for DAS28-CRP(3) (p < 0.0001). After 12 weeks of treatment, the scores for DAS28-CRP(4) and DAS28-CRP(3) had improved by −1.39 ± 1.34 (p < 0.0001) and −1.18 ± 1.22 (p < 0.0001), respectively. The mean difference between the 2 DAS scores [DAS28-CRP(3) – DAS28-CRP(4)] at baseline and at 12 weeks was −0.28 ± 0.32 (p < 0.0001) and −0.07 ± 0.31 (p < 0.0001). The difference between the 2 DAS scores was significantly higher at baseline than at 12 weeks (p < 0.0001). The mean difference between the changes in the scores [ΔDAS28-CRP(3) – ΔDAS28-CRP(4)] was +0.21 ± 0.35 (p < 0.0001) (Table 2 and Figure 1).
The differences between the 2 DAS scores were correlated with the mean of the DAS scores at baseline and at 12 weeks, with r values of −0.30 (p < 0.0001) and −0.40 (p < 0.0001), respectively. Differences in DAS change between the 2 scores were correlated with the mean of DAS changes (r = −0.35, p < 0.0001), as shown in scatterplots in Figure 1. The 2 DAS scores were intercorrelated at baseline (r = 0.96, p < 0.0001) and at 12 weeks (r = 0.97, p < 0.0001). As well, the changes in the 2 DAS scores were intercorrelated (r = 0.97) (p < 0.0001) (Figure 2).
ES and SRM were slightly higher for DAS28-CRP(4) compared to DAS28-CRP(3); Table 1. ESi for DAS28-CRP(4) was 1.2 ± 1.1 compared to 1.1 ± 1.1 for DAS28-CRP(3) (p < 0.0001). Compared to DAS28-CRP(4) and according to the DAS28 thresholds, DAS28-CRP(3) categorized about 33% fewer patients as having a high level of disease activity both at baseline and at 12 weeks, whereas the number of patients with moderate disease activity was overestimated, with 37% and 16% at the 2 timepoints. DAS28-CRP(3) underestimated the number of good responders by 8% and overestimated the number of nonresponders by 12% (Table 3 and Figure 2).
Patients categorized according to DAS28-CRP thresholds for disease activity and treatment response. Minimal disease activity: DAS28-CRP < 2.6; low disease activity: 2.6 ≤ DAS28-CRP ≤ 3.2; moderate disease activity: 3.2 < DAS28-CRP ≤ 5.1, high disease activity; DAS28-CRP > 5.1.

Correlation plots showing the association between (A) Disease Activity Score-28-C-reactive Protein 3 [DAS28-CRP(3)] and DAS28-CRP(4) and (B) change in DAS28-CRP(3) and DAS28-CRP(4) 12 weeks after start of biological treatment. The regression line, 95% CI (solid lines), and 95% prediction interval (broken lines) are shown. The regression equation, standard error of estimate (SEE), and correlation coefficient (r) for (A): y = 0.87x + 0.37, SEE = 0.27, r = 0.97, p < 0.0001 and (B): y = 0.88x + 0.04, SEE = 0.31, r = 0.97, p < 0.0001. DAS thresholds for disease activity and responses are illustrated by vertical and horizontal solid lines. Numbers of patients in the different disease activity and response categories shown in Table 3 have been added.
When the CDAI criteria for remission was used as the gold standard and DAS28-CRP < 2.6 was considered to reflect remission, DAS28-CRP(3) misclassified 33% more patients as being in remission at baseline and 17% more at followup than did the DAS28-CRP(4). For the SDAI remission criteria, the corresponding numbers were 29% and 13%. When the ACR/EULAR Boolean-based definition of remission was used as the gold standard9, DAS28-CRP(3) misclassified 42% more patients as being in remission at baseline and 28% more at followup than did DAS28-CRP(4). It must be stressed, however, that a DAS threshold is no longer regarded as useful to classify remission9.
Multiple regression analysis showed that the DAS28-CRP(4) response was most strongly explained by change in TJC (beta = 0.47, rp = 0.74, p < 0.0001), followed by change in PGA (beta = 0.36, rp = 0.63, p < 0.0001), in SJC (beta = 0.18, rp = 0.39, p < 0.0001), in CRP (beta = 0.15, rp = 0.35, p < 0.0001), and in PHGA (beta = 0.12, rp = 0.23, p < 0.001), with R2 = 0.88 (p < 0.0001). The DAS28-CRP(3) response was also mostly strongly explained by change in TJC (beta = 0.57, rp = 0.75, p < 0.0001), but in this case followed by change in SJC (beta = 0.22, rp = 0.40, p < 0.0001), in CRP (beta = 0.17, rp = 0.34, p < 0.0001), in PHGA (beta = 0.14, rp = 0.22, p < 0.001), and in PGA (beta = 0.10, rp = 0.17, p < 0.05), with R2 = 0.82 (p < 0.0001). Change in HAQ score did not add significantly to the prediction of the DAS responses.
DISCUSSION
The original DAS was based on ESR, but modifications of DAS and DAS28 led to equations including CRP instead5,8. Using CRP for calculation of the DAS28 is an attractive alternative to ESR, as CRP is routinely measured in clinical practice14,23, is a more direct measure of inflammation than ESR, is more sensitive to short-term changes24,25, is associated with radiological progression in RA26, and is considered at least as valid as ESR to measure RA disease activity27,28.
The equations for DAS28-CRP with 3 and 4 variables were formulated to “give good estimations of DAS28-ESR values on a group level”8. The possibility of switching between different types of DAS scores in daily clinical practice has been questioned15,29, but only a few studies have actually investigated the agreement between the different DAS instruments. Data analyses from large cohort databases showed that DAS28-CRP(4) and DAS28-ESR are well correlated, but disease activity tends to be underestimated when DAS28-CRP(4) is used30,31. In support of this, the DAS28-ESR and DAS28-CRP(4) definitions differed substantially in classifying patients with RA as having moderate or high disease activity, with the CRP definition resulting in a lower proportion of high DAS28 scores, especially in women29. DAS28-CRP(4) also produced lower values than DAS28-ESR in patients with early RA32. Further, a comparison of the 2 scores after 6 months of treatment with a biological agent also showed a tendency for lower scores using the DAS28-CRP(4)20.
Although these disagreements between the CRP and ESR DAS28 definitions have been established, DAS28-CRP(4) has been widely accepted as an alternative to DAS28-ESR. In contrast, the DAS28-CRP(3) seems to have escaped much attention. DAS28-CRP(3) is, however, more manageable than DAS28-CRP(4), as it comprises only 3 variables. Moreover, it may be considered to be a more objective measure of disease activity, because it is not influenced by PGA. When DAS28-CRP(4) is used for treatment decisions (also involving biologics) in individuals, it must be recognized that it may represent a challenge that some patients have a very low and others a very high threshold for complaints. In daily clinical practice it is in fact frequently observed that patients score higher on the PGA than would be expected on the basis of their clinical disease activity33. Accordingly, it has been shown that patients do not always present a PGA ≤ 1 (which is mandatory to satisfy the ACR/EULAR Boolean-based definition of remission in RA9) despite a good clinical disease state34. Because thresholds for the different versions of DAS28 are identical, it would be tempting to use DAS28-CRP(3) or to use DAS28-CRP(3) and DAS28-CRP(4) interchangeably in the daily clinic. On the other hand, because PGA has been substituted with constant values in the equation for DAS28-CRP(3)8, the 2 scores cannot agree perfectly in all individual patients. Using cross-sectional data from DANBIO, it was previously shown that the 2 scores agreed rather well on a group level, with a small underestimation of DAS28-CRP(3) compared to DAS28-CRP(4), but disagreement may be significant in individuals16. No other studies have evaluated DAS28-CRP(3) against other DAS scores.
The present study was the first to compare the 2 DAS28-CRP scores regarding sensitivity to change, and to assess agreement between the scores and their changes after initiation of biological treatment and to assess differences between the scores regarding categorization of disease activity. Agreement between the scores was assessed according to Bland and Altman. This measure has a direct interpretation that can be applied not only to groups of patients but also to individual patients19. The 2 scores agreed well at a group level at 12 weeks, with only a small mean inter-score difference, and agreed better at 12 weeks than at baseline, where DAS scores were higher. Further, the bias between the scores and between their changes during treatment tended to move in a negative direction with increasing DAS values. This is in accord with our previous cross-sectional finding that the bias is more pronounced and more negative when DAS scores are high16. The reason for this is that the equation for DAS28-CRP(3) substituted constant values for the PGA in a way that leads inevitably to increasing underestimation of DAS28-CRP(3) [compared to DAS28-CRP(4)] with increasing PGA. This can easily be seen using a DAS calculator. As PGA is positively associated with the DAS score, DAS28-CRP(3) conforms more closely to DAS28-CRP(4) for lower DAS scores.
On the individual level, differences between the DAS versions varied widely not only at baseline but also at 12 weeks. The potential clinical implication was clearly revealed when the disease activity level was categorized according to DAS thresholds. No less than one-third of those patients who had a high disease activity, defined as DAS28-CRP(4) above 5.1, were categorized as belonging to a group with a lower disease activity by DAS28-CRP(3). This was the case both at baseline and at 12 weeks. Compared to SDAI and CDAI remission thresholds and the ACR/EULAR Boolean-based definition of remission9, DAS28-CRP(3) overestimated more patients as being in remission (using the previously mentioned DAS threshold for remission that is now regarded as obsolete) than did DAS28-CRP(4). This may indicate that DAS28-CRP(3) is a less appropriate measure than DAS28-CRP(4), at least for minimal disease activity. Regarding response to treatment, Cohen's effect sizes and SRM were found to be similar for the 2 scores (and rather high), but compared to the DAS28-CRP(4), DAS28-CRP(3) overestimated the number of nonresponders, while the number of good responders was underestimated. Thus, altogether it may be critical whether the clinician chooses DAS28-CRP with 3 or with 4 variables as a tool for making treatment decisions and evaluating treatment responses because the 2 scores may lead to different conclusions for the patient.
It is important for the clinician's interpretation of the DAS score and the DAS score response to know how it is influenced by the score components and other measures of disease activity. Because of these ties, measures that are not included in the DAS may also contribute to the prediction16. In the present study, TJC was the most important predictor of DAS28-CRP(3) and DAS28-CRP(4) at baseline as well as at 12 weeks. PGA was the second most important predictor of DAS28-CRP(4), but it had no influence on DAS28-CRP(3)16. Similarly, DAS28-CRP(4) and DAS28-CRP(3) responses were most strongly influenced by change in TJC. Change in PGA was the second most important predictor of DAS28-CRP(4) response, but had only a minor influence on the response of DAS28-CRP(3), reflecting the more objective nature of this score.
The study provided baseline and 12-week data. It did not provide information on the agreement between DAS28-CRP(3) and DAS28-CRP(4) in individual patients or groups of patients regarding absolute DAS scores or achievement of remission after longer periods of treatment. Comparisons of the 2 scores were not possible regarding longterm predictability of outcome measures such as radiological progression, physical function, and quality of life. Further studies are needed to clarify the value of DAS28-CRP(3) compared to DAS28-CRP(4).
After 12 weeks of biological treatment, sensitivity to change was similar for DAS28-CRP(3) and DAS28-CRP(4), but in individual patients the difference between the scores and between their responses may be substantial. Using DAS28-CRP(3) in place of DAS28-CRP(4), a considerable proportion of the patients was misclassified regarding category of disease activity and response to treatment.
- Accepted for publication December 18, 2012.








{kind=link}
{kind=link}