

Abstract
Objective. To evaluate homocysteine levels in patients with Takayasu arteritis (TA) and in controls, and to analyze associations between homocysteine levels and paraoxonase 1 (PON1) activity, cysteine levels, methotrexate use, disease activity, extent of arterial involvement, and ischemic events in patients with TA.
Methods. A cross-sectional study was performed with 29 patients with TA and 30 controls who underwent clinical evaluation and blood sample collection in the fasting state.
Results. Among patients with TA, active disease was observed in 9 (31.0%) and previous arterial ischemic events in 10 (34.5%). Therapy with methotrexate was prescribed to 9 (31.0%) patients and it was associated with folic acid in 8 cases. Median homocysteine level was higher in patients with TA [10.9 μmol/l, interquartile range (IQR) 9.6–14.8] than in controls (6.9 μmol/l, IQR 5.1–11.9; p < 0.001). No difference was found regarding mean homocysteine levels between those using methotrexate and those under other therapies (12.8 ± 5.3 μmol/l vs 12.1 ± 3.2 μmol/l, respectively; p = 0.662). TA patients with active disease presented lower homocysteine levels (10.4 ± 2.1 μmol/l) compared to TA patients in remission (13.1 ± 4.2 μmol/l) (p = 0.034). A significant correlation was found between cysteine and homocysteine levels in patients with TA (ρ = 0.676, p < 0.0001), while there was no correlation between homocysteine and PON1 activity (ρ = 0.214, p = 0.265). Median homocysteine levels were higher in patients with ischemic events (13.2 μmol/l, IQR 10.9–17.5) compared to patients with no ischemic events (9.8 μmol/l, IQR 8.7–14.7; p = 0.027) and were associated with arterial ischemia in patients with TA (OR 1.31, 95% CI 1.01–1.71, p = 0.041).
Conclusion. Patients with TA presented higher homocysteine levels than controls and homocysteine was associated with an increased risk of arterial ischemic events in TA.
Takayasu arteritis (TA) is a chronic idiopathic vasculitis that predominantly affects large vessels including the aorta, its main branches, and pulmonary and coronary arteries. Vessel wall inflammation may lead to stenosis, occlusion, dilation, or aneurysm formation1,2. Arterial thrombotic events are frequently found in patients with TA and include ischemic stroke in 5.0%–15.8%, transient ischemic attacks (TIA) in 3.0%–6.3%, and acute coronary syndromes in 7.3%–17.0%3,4,5,6,7,8. Although abnormal arterial anatomy and atherosclerotic lesions may partially account for the increased risk of thrombotic ischemic events in TA, a hypercoagulable state has been described and it is mainly related to enhanced platelet and coagulation activities9,10,11,12.
Homocysteine is a sulfur-containing intermediate amino acid produced during the metabolism of methionine. It is classically elevated in patients with genetic defects of enzymes involved in its metabolism, in nutritional deficiency of vitamin cofactors such as folate, vitamin B6 and vitamin B12, and in conditions including chronic renal failure, cancer, hypothyroidism, and pernicious anemia. Certain drugs may cause elevations in homocysteine levels, especially methotrexate (MTX)13,14,15. High plasma homocysteine is an independent risk factor for coronary artery disease, cerebrovascular disease, and peripheral vascular occlusive disease16,17. Some mechanisms proposed to explain how high homocysteine levels may contribute to the development of cardiovascular disease are endothelial dysfunction through the antagonizing nitric oxide effects, the production of oxygen-reactive species, impairment of paraoxonase 1 (PON1) activity, activation of smooth muscle cells, and increased thrombogenicity through deposition of fibrin on arterial walls18. Cysteine is a semi-essential amino acid with structure and metabolic pathways similar to homocysteine, and both amino acids participate in the redox-thiol state that is important for antioxidant protection and in cardiovascular disease19.
To our knowledge, no study has evaluated homocysteine levels in TA and its association with disease activity, MTX use, and arterial ischemic events. Our aims were to evaluate whether patients with TA present higher levels of homocysteine compared to controls, and to analyze the correlation between plasma homocysteine levels and cysteine levels, PON1 activity, MTX and folate use, disease activity, extent of arterial involvement, and ischemic arterial events in patients with TA.
MATERIALS AND METHODS
A cross-sectional study was performed in female patients who fulfilled the American College of Rheumatology classification criteria for TA20 and were undergoing regular followup at the Vasculitis Unit of the Universidade Federal de São Paulo (Unifesp/EPM). Thirty-five patients with TA were screened for our study and 29 agreed to participate. Thirty age-matched and sex-matched controls were evaluated as well. The study protocol was approved by the Institutional Ethics Committee and all participants gave informed consent (protocol CEP 0134/11). In patients with TA, information was collected about demographic features, disease manifestations, angiographic lesions in aorta and its main branches by magnetic resonance angiography performed in the last year, current therapy, and previous ischemic events; in controls, information was collected on demographic features, comorbidities, ischemic events, and medical therapy. Arterial ischemic events recorded in our study included acute myocardial infarction, unstable angina, stroke, transient ischemic attack, limb ischemia, and abdominal angina according to established criteria21,22,23,24,25,26. A 12-hour fasting blood sample was collected for laboratory measurements that included the Westergren erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), creatinine, homocysteine and cysteine levels, and PON1 activity in patients with TA; in the control group, creatinine and homocysteine levels were recorded. CRP was detected by immunonephelometry, while total plasma homocysteine and cysteine levels were measured by high-performance liquid chromatography using fluorimetric detection and isocratic elution27. Hyperhomocysteinemia was considered if homocysteine levels were > 15 μmol/l13,27. PON1 activity was determined by spectrophotometry using paraoxon as substrate (paraoxonase activity) in the presence of 1 M sodium chloride, and the arylesterase activity of PON1 was measured using phenylacetate as a substrate, as described28,29. Paraoxonase and arylesterase activity of PON1 are presented as U/ml.
Active disease in TA was considered if the patient presented new lesions in vascular imaging studies or at least 2 of the following features were present: (1) new onset of carotidynia or pain over other large arteries, (2) transient ischemic episodes not attributed to other factors, (3) new bruit or new asymmetry in pulses or blood pressure, (4) systemic symptoms in the absence of infection, or (5) an increase in the ESR3. The angiographic classification of the International TA conference in Tokyo 1994 was used to classify the distribution of arterial lesions in 6 types as follows: type I (only the branches of the aortic arch are involved); type IIa (involvement of the ascending aorta, arch, and its branches); type IIb (involvement of the ascending aorta, arch with its branches, and thoracic descending aorta); type III (involvement of the thoracic descending aorta, abdominal aorta, and/or renal arteries); type IV (only the abdominal aorta and/or renal arteries involved); and type V (combined features of type IIb and IV)30. Angiographic type V was regarded as the most extensive arterial involvement in TA.
Statistical analysis
SPSS 18.0 software was used for statistical analysis and GraphPad Prism 5 software was used to build graphs. Categorical variables are presented as total number (percentage) while continuous data are presented as mean (SD) when variables were normally distributed, or as median [interquartile range (IQR)] in case of non-normal distribution. Comparison between groups was performed using chi-square test or Fisher’s exact test for categorical variables and Student’s t test or Mann-Whitney U test for continuous data. Correlations between numerical variables were analyzed using Spearman correlation coefficient. Univariate logistic regression analysis models were performed to verify associations between homocysteine and cysteine levels with ischemic events in patients with TA, whereas a multivariate analysis evaluated the association of age, disease duration, and homocysteine levels as independent risk factors for ischemic events in TA. Results are expressed in OR and 95% CI. The accepted significance level was 5% (p < 0.05).
RESULTS
Patients with TA and controls
Demographic features were comparable between 29 patients with TA and 30 controls for median age at the time of the study [38.0 yrs (IQR 27.5–48.5) vs 34.0 yrs (IQR 27.0–49.5), respectively; p = 0.826] and the frequency of white individuals (41.4% vs 43.3%; p = 0.879). All study participants were female. Table 1 describes the disease features presented by patients with TA and therapy used at study. All but one patient taking weekly MTX received concomitant 5 mg of folate weekly. Serum creatinine levels were similar between patients and controls [0.88 mg/dl (IQR 0.73–1.22) vs 0.80 mg/dl (IQR 0.71–0.89); p = 0.203] and between patients with active TA disease and those in remission (Table 2). Only 2 patients with TA (6.8%) had endstage renal disease and were receiving regular hemodialysis, while the other patients had normal renal function.
Disease features and therapeutic modalities of patients with Takayasu arteritis. Numerical data are presented as mean ± SD or as median (interquartile range) unless otherwise indicated.
Comparison between Takayasu arteritis patients with active and inactive disease. Numerical data are presented as mean ± SD or as median (interquartile range) unless otherwise indicated.
Homocysteine, cysteine levels, PON1 activity
Patients with TA had higher median plasma homocysteine levels [10.9 μmol/l (IQR 9.6–14.8) vs 6.9 μmol/l (IQR 5.1–11.9); p < 0.001; Figure 1] and a higher prevalence of hyperhomocysteinemia compared to controls (20.7% vs 3.3%; p = 0.039). Homocysteine and cysteine levels were significantly lower in those with active disease. On the other hand, inflammatory measures such as ESR and CRP were higher in patients with active disease, but the difference was significant only for ESR values (Table 2).

Median homocysteine levels were significantly higher in patients with Takayasu arteritis than in controls matched for age and sex.
Mean homocysteine levels were similar in patients with TA taking MTX and in those being treated with other immunosuppressive agents (12.8 ± 5.3 μmol/l vs 12.1 ± 3.2 μmol/l, respectively; p = 0.662). Regarding the extent of arterial involvement, no differences regarding mean homocysteine levels were found in TA patients with angiographic type V in comparison to other angiographic types (12.7 ± 4.2 μmol/l vs 11.0 ± 2.6 μmol/l; p = 0.342). Paraoxonase activity and arylesterase activity of PON1 were similar between TA patients with active disease and TA patients in remission (Table 2).
A significant positive correlation was found between homocysteine and cysteine levels (ρ = 0.676, p < 0.0001), whereas a negative correlation was found between homocysteine and ESR (ρ = −0.415, p = 0.025). There was no correlation between homocysteine levels and CRP values (ρ = 0.043, p = 0.824) or between homocysteine levels and the weekly dose of MTX (ρ = 0.062, p = 0.873). Homocysteine levels were positively correlated with serum creatinine levels (ρ = 0.361, p = 0.026), whereas no correlation was found between cysteine and serum creatinine levels (ρ = 0.104, p = 0.612). Plasma homocysteine levels were not correlated to either paraoxonase or to arylesterase activity (ρ = 0.214, p = 0.265, and ρ = 0.219, p = 0.254, respectively).
Arterial ischemic events
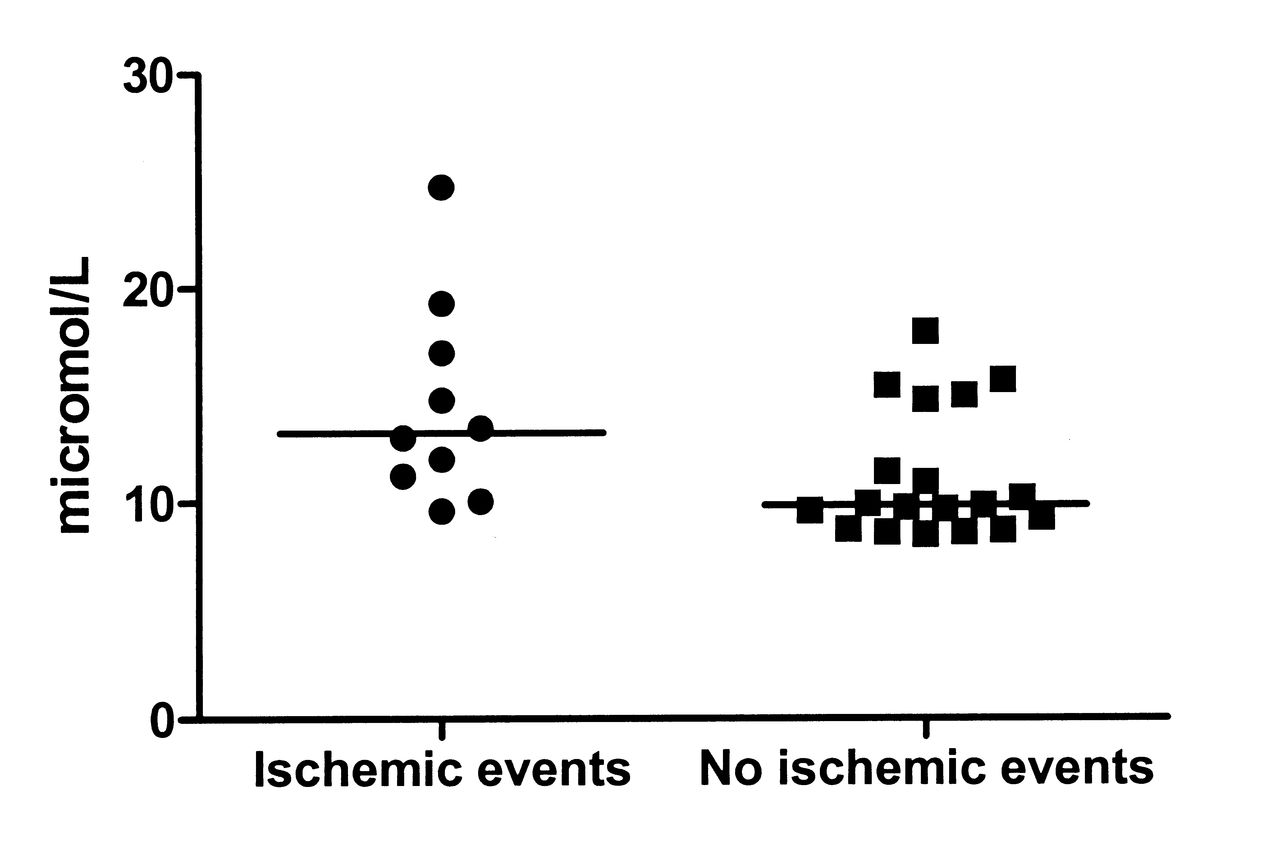
Previous ischemic events were found in 10 patients with TA (34.5%) and in none of the controls (p < 0.001). Acute coronary syndromes were observed in 6 patients, while stroke, transient ischemic attacks, and abdominal angina were found in 2 patients each. One patient developed lower limb ischemia due to an atherosclerotic plaque rupture in the left femoral artery, resulting in thrombosis and distal embolism. Median homocysteine levels were significantly higher in patients with previous ischemic events compared to those without [13.2 μmol/l (IQR 10.9–17.5) vs 9.8 μmol/l (IQR 8.7–14.7), respectively; p = 0.027; Figure 2] as well as mean cysteine levels (545.1 ± 63.5 μmol/l vs 478.2 ± 84.9 μmol/l; p = 0.038). No differences were found between TA patients with and those without arterial ischemic events regarding paraoxonase activity [356.0 U/ml (IQR 96.6–580.25) vs 263.0 U/ml (IQR 99.0–413.0); p = 0.195] and arylesterase activity (71.0 ± 13.3 U/ml vs 66.4 ± 31.1 U/ml; p = 0.666).
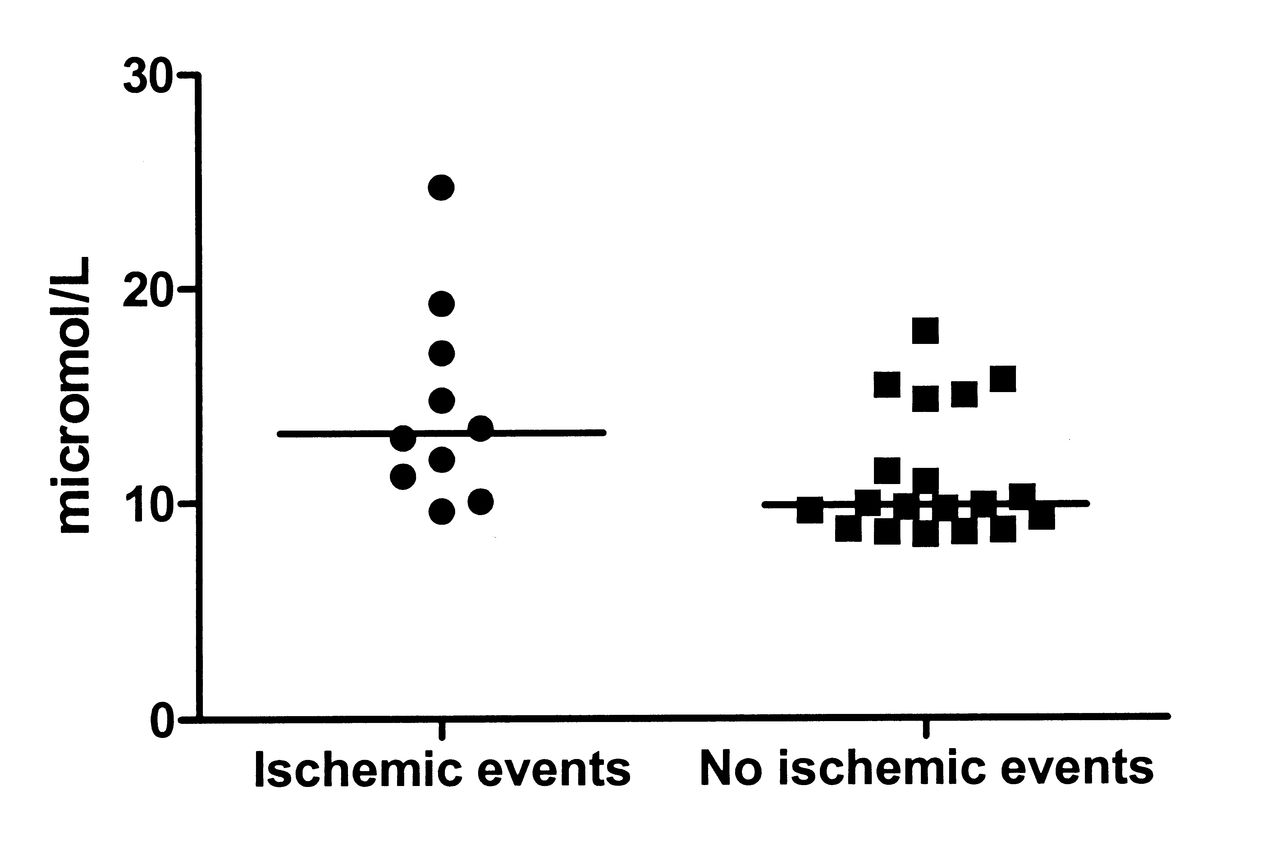
Patients with Takayasu arteritis who had previous ischemic events presented significantly higher median homocysteine levels compared to those without a record of arterial ischemia.
In a univariate logistic regression analysis, the increase of 1 μmol/l of homocysteine plasma levels was associated with ischemic events in TA (OR 1.28, 95% CI 1.00–1.63, p = 0.049), while in the multivariate model that included age, disease duration, and homocysteine levels, both age and 1-μmol/l increase in plasma homocysteine levels were independently associated with ischemic events in TA (Table 3). Using the univariate model the increase in cysteine levels was not significantly associated to an increased risk of ischemic events in patients with TA (OR 1.12, 95% CI 1.00–1.25, p = 0.051).
Multivariate analysis to evaluate associations with arterial ischemic events in Takayasu arteritis.
DISCUSSION
We show for the first time, to our knowledge, that plasma homocysteine levels were higher in patients with TA in comparison to control subjects, and that among patients with TA, homocysteine levels were independently associated with acute arterial ischemic events but not with disease activity, with MTX use, or with the extent of vascular involvement. Indeed, patients with TA in remission presented significantly higher homocysteine levels than TA patients with active disease, and a negative correlation between plasma homocysteine levels and ESR value was found.
The increase in homocysteine levels in patients with TA may be multifactorial, and causes may include impaired renal function due to the involvement of renal arteries, MTX therapy, and accelerated atherosclerosis14,15,18. In our study, neither creatinine levels nor MTX use could be found to be responsible for higher homocysteine levels in patients with TA, because serum creatinine levels were similar between TA patients and controls, while patients receiving MTX did not present higher homocysteine levels in comparison to those taking other immunosuppressive agents. The use of folate associated with MTX in patients with TA may have precluded the increase in plasma homocysteine levels. Similarly, the use of folate associated with MTX in rheumatoid arthritis has been shown to prevent increases in plasma homocysteine levels in comparison to patients treated only with low-dose MTX31. Accelerated atherosclerosis is another possible cause for higher homocysteine levels among patients with TA, and although evaluation of subclinical atherosclerotic disease was not the aim of our study, Seyahi, et al observed a higher prevalence of carotid atherosclerosis in patients with TA in comparison to patients with systemic lupus erythematosus and controls32. Hence, the association between homocysteine levels and subclinical atherosclerosis in TA remains an open question.
The apparently unexpected finding of lower homocysteine and cysteine levels in TA patients with active disease in comparison to those in remission has also been described by Martinez-Taboada, et al in patients with giant cell arteritis (GCA) and polymyalgia rheumatica33. The use of glucocorticoids was the reason given by those authors to explain the higher homocysteine levels in patients with GCA in remission, because blood samples were collected prior to glucocorticoid therapy in all patients with active disease and a second measurement of homocysteine was performed in patients in remission and still receiving glucocorticoid therapy33. In our study, glucocorticoid use could not be considered as the cause of lower homocysteine levels in patients with active TA because the median daily prednisone dose was similar between TA patients with active and those with inactive disease, and no correlation was found between plasma homocysteine levels and daily prednisone dose (data not shown). Other factors such as age and creatinine levels that could explain the higher homocysteine levels in patients with TA in remission were similar in both active and inactive disease groups.
We observed that increased homocysteine levels were associated with acute arterial ischemic events in TA, and the risk of ischemia was observed with every 1-μmol/l increase in homocysteine levels. In a metaanalysis in the general population, a similar OR (1.32, 95% CI 1.19–1.45) for coronary artery disease was found with every 5-μmol/l increase in plasma homocysteine levels16. Although high homocysteine levels are associated with a higher risk of cardiovascular events, folate supplementation in clinical trials led to an average 25% reduction in homocysteine levels, but did not prevent cardiovascular ischemic events such as coronary syndromes or stroke in clinical trials34.
We found no association between paraoxonase activity or arylesterase activity and homocysteine levels, disease activity, and/or ischemic events. In a previous study, arylesterase activity was shown to be lower in patients with TA than in controls35. Our findings suggest that the arterial inflammatory burden of active TA may not be responsible for a decrease in paraoxonase and arylesterase activity. Holven, et al showed that individuals with hyperhomocysteinemia, especially those with extremely high levels, presented less PON1 activity compared to healthy controls36. PON1 activity plays a protective role in atherosclerotic disease, and 2 mechanisms have been proposed that include the antioxidant protection of low-density lipoprotein and the hydrolysis of homocysteine thiolactone, a toxic metabolite of homocysteine that causes protein homocysteinilation18.
Although cysteine levels were significantly higher in TA patients with previous ischemic events, no increased risk of ischemic arterial events was found with increasing cysteine levels. The association with cardiovascular events has not been studied as extensively for cysteine as it has for homocysteine. However, cysteine levels do not seem to represent a strong risk factor for cardiovascular events. In one study, cysteine levels were strongly associated with several factors included in the risk profile for cardiovascular disease such as age, total cholesterol, diastolic blood pressure, and body mass index37. Both low and high levels of cysteine have been linked to cerebrovascular disease and peripheral artery disease, whereas the relationship with coronary artery disease has not been significant37,38.
Based on results from trials on homocysteine-lowering therapy in the general population34, it is doubtful whether folate supplementation will play a role in the prevention of ischemic events in TA; indeed, studies evaluating this intervention are lacking in this large-vessel vasculitis. To date, antiplatelet therapy is the only intervention that has been shown to decrease the risk of arterial ischemic events in TA in a retrospective study8. However, control of disease activity with an eventual decrease of arterial inflammation may also be important to prevent the development of arterial anatomic abnormalities and arterial ischemic events in TA.
One limitation of our study is the relatively low number of individuals for comparisons between subgroups of patients with TA such as active disease versus remission, and patients with and without previous arterial ischemic events. Other limitations that should be taken into account are the use of criteria for disease activity in TA that have not been validated yet, and the lack of a control group with other systemic inflammatory diseases.
Patients with TA presented higher total plasma homocysteine levels than control subjects, and homocysteine was associated with an increased risk of arterial ischemic events in TA, indicating a possible additional mechanism to explain the hypercoagulable state and an association with increased subclinical atherosclerosis in TA. Although cysteine levels were also higher in TA patients with arterial ischemic events, they were not associated with an increased risk of arterial ischemic events. A negative association was found between homocysteine levels and disease activity, while no increase in homocysteine levels was observed in TA patients with more extensive arterial involvement. The addition of folate to MTX therapy apparently prevented the increase in homocysteine levels in TA. Finally, no association was found between PON1 activity and disease activity, homocysteine levels, or arterial ischemic events.
Acknowledgment
The authors thank Maria Teresa Costa for her contribution in collecting blood samples for this study.
- Accepted for publication October 29, 2012.








{kind=link}
{kind=link}