

Abstract
Objective. The pathophysiology of shrinking lung syndrome (SLS) is poorly understood. We sought to define the structural basis for this condition through the study of pulmonary mechanics in affected patients.
Methods. Since 2007, most patients evaluated for SLS at our institutions have undergone standardized respiratory testing including esophageal manometry. We analyzed these studies to define the physiological abnormalities driving respiratory restriction. Chest computed tomography data were post-processed to quantify lung volume and parenchymal density.
Results. Six cases met criteria for SLS. All presented with dyspnea as well as pleurisy and/or transient pleural effusions. Chest imaging results were free of parenchymal disease and corrected diffusing capacities were normal. Total lung capacities were 39%–50% of predicted. Maximal inspiratory pressures were impaired at high lung volumes, but not low lung volumes, in 5 patients. Lung compliance was strikingly reduced in all patients, accompanied by increased parenchymal density.
Conclusion. Patients with SLS exhibited symptomatic and/or radiographic pleuritis associated with 2 characteristic physiological abnormalities: (1) impaired respiratory force at high but not low lung volumes; and (2) markedly decreased pulmonary compliance in the absence of identifiable interstitial lung disease. These findings suggest a model in which pleural inflammation chronically impairs deep inspiration, for example through neural reflexes, leading to parenchymal reorganization that impairs lung compliance, a known complication of persistently low lung volumes. Together these processes could account for the association of SLS with pleuritis as well as the gradual symptomatic and functional progression that is a hallmark of this syndrome.
Shrinking lung syndrome (SLS) was first described as a complication of systemic lupus erythematosus (SLE) by Hoffbrand and Beck1. The term identifies a constellation of respiratory manifestations including dyspnea, reduced lung volumes, and/or elevated hemidiaphragms on chest radiograph, and a restrictive ventilatory defect assessed by pulmonary function tests (PFT). Serial chest radiographs demonstrate steadily declining lung volumes as patients with SLS become more dyspneic, rendering the impression that the lungs are vanishing. SLS is rare, with an estimated prevalence of < 1% among patients with SLE, although some reports have suggested a higher prevalence2,3,4. The syndrome has been reported in other rheumatologic disorders including systemic sclerosis, Sjögren’s syndrome, rheumatoid arthritis, and undifferentiated connective tissue disorder5,6,7,8.
The pathogenesis of SLS remains unknown. Chest imaging shows no evidence of interstitial lung disease or vascular pathology, although chest pain and small pleural effusions are common9. While patients may become markedly dyspneic, mortality is rare. The literature contains a single autopsy report of a patient with SLS who expired following prolonged mechanical ventilation for pneumonia, making findings difficult to interpret10,11. Because pathologic data are unavailable, theories of the etiology of SLS are speculative and include surfactant deficiency1, diaphragmatic myopathy12, phrenic neuropathy13, and chest wall dysfunction9,14,15.
The hallmark abnormality in SLS is restrictive lung disease with a marked reduction in total lung capacity (TLC). The physiological basis for this restriction is unclear. Pulmonary restriction may arise through parenchymal changes that impair lung compliance (intrinsic restriction). Alternatively, restriction may originate outside the lung (extrinsic restriction), reflecting either structural limits on the chest wall (e.g., obesity, scoliosis, pleural adhesions) or functional compromise due to muscle disease, neuropathy, or reflex inhibition of muscle engagement.
Conventional PFT fail to discriminate among mechanisms of ventilatory restriction because pressure measured at the mouth reflects both the force generated by the chest wall and the ability of the lung to expand. This limitation is addressed by concomitant esophageal manometry. Because the esophagus is thin-walled, pressure within the distal esophagus mirrors the pressure in the adjacent pleural space, permitting direct measurement of the maximal inspiratory force developed by the chest wall (MIPes)16. Lung compliance can be determined by coupling MIPes data with measurement of airflow and pressure at the mouth. Importantly, MIPes can be assessed over a range of lung volumes, and changes across the volume spectrum have diagnostic significance. Low MIPes values throughout the lung volume range suggest a respiratory myopathy. In contrast, MIPes values that are normal at low lung volumes but decreased at high volumes indicate either constrained chest wall expansion or inhibition of respiratory muscle activation by volitional or reflex mechanisms, as occurs in pleurisy. Thus, esophageal manometry permits definition of the contributions of intrinsic and extrinsic factors to pulmonary restriction.
We report the result of esophageal manometry studies in SLS. One patient underwent manometry before and after treatment, affording the opportunity to determine the physiological correlates of clinical improvement. The novel insights that emerge from these studies suggest a new pathophysiologic model of SLS.
MATERIALS AND METHODS
Case definition
SLS was defined as encompassing patients with a systemic rheumatic disease who presented with (1) dyspnea; (2) decreased lung volumes on chest radiography; (3) PFT demonstrating a restrictive ventilatory defect with normal diffusing capacity of the lung for carbon monoxide (DLCO) corrected for alveolar volume and hemoglobin concentration; and (4) absence of parenchymal pathology on chest computed tomography (CT). Rheumatic disease categorization was by American College of Rheumatology definitions17. Patients who met criteria for SLS and underwent pulmonary evaluation with esophageal manometry between 2007 and 2011 were identified at the Brigham and Women’s Hospital and Boston Children’s Hospital. All diagnoses of SLS were confirmed through chart review by an outside reviewer with expertise in SLE (CS). Clinical data were obtained from medical records. Patients with active SLS evaluated during this time interval but who had not undergone pulmonary mechanics evaluation were identified at Boston Children’s Hospital by a survey of attending rheumatologists and at Brigham and Women’s Hospital through an electronic search of rheumatology clinic notes for the term “shrinking lung.” This study was performed in accord with the Partners Institutional Review Board (2010P002092).
Esophageal balloon manometry
Pulmonary studies were conducted by a single investigator (SHL). Measurements were made with the patient awake and seated. An esophageal balloon catheter (Jaeger-Toenneis; Viasys) was passed by nose to position the tip of the balloon at 35–40 cm from the nares. The balloon was 10 cm long, 2 cm in perimeter, and inflated with 0.5 ml air. Correct placement of the catheter in the distal esophagus was confirmed by negative pressure deflections during inspiration and a negligible change in transpulmonary pressure during inspiratory or expiratory efforts against an occluded airway. Flow measured with a pneumotachograph (Fleisch no. 2; Phipps & Bird) was integrated to indicate relative volume. Pressures, flow, and volume were recorded using custom-made software (Npulmo, by E. Millet) and commercial hardware (Dataq Instruments). Static deflation curves of the lung measured during interrupted expiration from TLC were used to estimate static lung compliance (Cst) near functional residual capacity (FRC). Dynamic lung compliance (Cdyn) was measured while the subject breathed at 20 breaths per minute to a metronome. Chest wall function and ventilatory muscle strength were assessed by measurement of MIPes at lung volumes from FRC to TLC.
Chest CT reformatting
All available chest imaging was reviewed for parenchymal pathology by a single radiologist (RRG). Chest CT digital imaging and communication in medicine data were post-processed on the Vitrea Enterprise suite 6.0 (Vital Images) to generate volume-rendered images depicting lung volume and density in Hounsfield units (HU). A 2-dimensional image was generated from 3-dimensional volume data by classification and composition of individual sample points of the view-aligned proxy geometry slices, allowing quantification of lung volume and density18,19,20.
RESULTS
Clinical presentation of SLS
Nine patients met the criteria for active SLS from 2007 to 2011. The age at onset of SLS ranged from 12 to 56 years, with the wide span reflecting the demographic population of the participating study centers, i.e., one adult and one pediatric hospital. Of the 9 patients with SLS, 6 (4 female and 2 male) underwent pulmonary mechanics evaluation as part of routine clinical care (Table 1). Three patients were not studied. Of these, 2 presented before pulmonary mechanics evaluation became routine, and the third presented at the end of the study period and was not evaluated because of concomitant acute medical issues; however, the 3 patients not studied were clinically similar to the 6 cases evaluated (Appendix 1). All studied patients presented with dyspnea lasting from 6 to 15 months; 2 were also dyspneic at rest. There was evidence of pleural inflammation in all patients: 5 reported pleuritic chest pain and 5 had transient, typically small pleural effusions, including the patient without pleuritic chest pain (video available from the authors upon request). Anti-Ro antibodies have been documented in high percentages of patients with SLS, and anti-RNP antibodies are associated with earlier pulmonary damage in SLE2,15. Four patients included in our study had extensive autoantibody testing, and all were positive for either anti-Ro (3/4) or anti-RNP (3/4) antibodies. Chest imaging revealed decreased lung volumes without evidence of interstitial lung disease or pulmonary adhesions. Chest fluoroscopy or ultrasound performed in 4 patients demonstrated decreased diaphragmatic excursion bilaterally. In Case 6, a dedicated chest ultrasound scan was performed to look for adhesions between the lung and diaphragm or chest wall; no evidence for adhesive restriction of diaphragm motion was found. The mean TLC was 45% of predicted, and the corrected DLCO was normal in all patients (Table 2). All cases had normal muscle enzymes at presentation with SLS.
Presentation of shrinking lung syndrome (SLS). Six subjects had active SLS symptoms during the study interval and underwent evaluation of pulmonary mechanics.
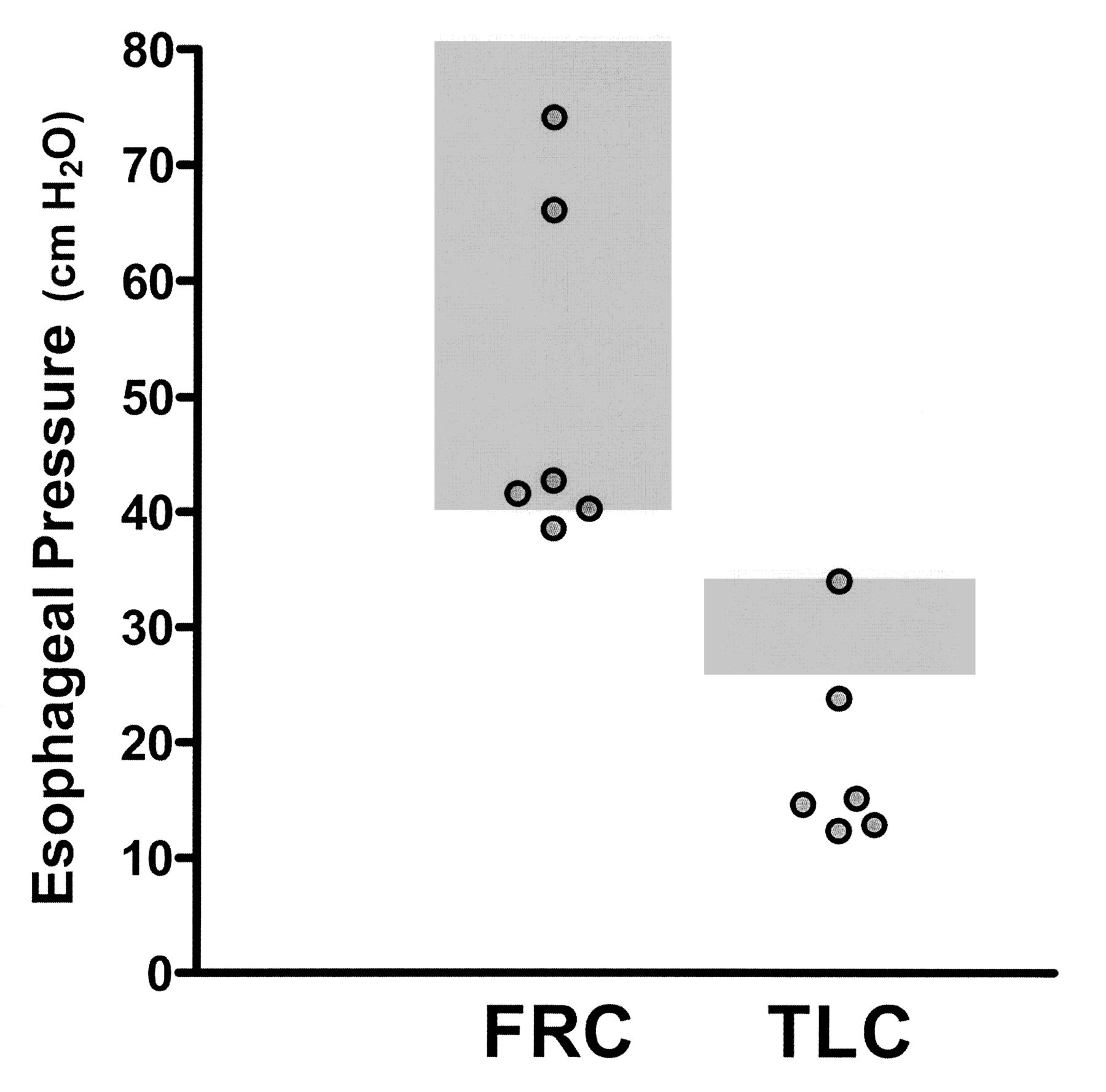
Pulmonary mechanics. Maximal inspiratory esophageal pressures (MIPes) are recorded by the esophageal balloon catheter method as negative pressures because they are measured in the thorax during inspiration; however, per convention, the absolute value is reported.
Esophageal manometry
MIPes obtained at FRC offer an assessment of inspiratory muscle strength. Conventional normal values at FRC are > 50 cm H2O, with 40–50 cm H2O representing marginal strength. Measurements < 30 cm H2O are considered clearly abnormal21,22,23. In all subjects, MIPes at FRC were marginal or normal, ranging from 38.5 to 74 cm H2O (Figure 1, Table 2). In contrast, inspiratory force at higher lung volumes was markedly reduced. MIPes at TLC were low in all but 1 subject, ranging from 12.2 to 23.7 cm H2O (normal 25–35 cm H2O; Figure 1, Table 2)24,25. This pattern of relatively well-preserved MIPes at FRC but reduced MIPes at TLC indicates limited lung expansion not due to intrinsic lung disease or respiratory myopathy but rather to either mechanical limitation of chest wall expansion or decreased respiratory muscle engagement.

Maximal inspiratory pressures measured by esophageal manometry at low and high lung volumes, i.e., at functional residual capacity (FRC) and at total lung capacity (TLC). Gray boxes represent normal values for maximal inspiratory pressures as measured by the esophageal balloon method (MIPes). MIPes are recorded by the esophageal balloon catheter as negative pressures because they are measured in the thorax during inspiration; however, the absolute value is reported.
Static (Cst) and dynamic (Cdyn) lung compliances were assessed to determine parenchymal distensibility. Cst, measured during periods of zero airflow from airway occlusions during passive exhalation beginning at TLC, is insensitive to airway resistance, while Cdyn, measured during spontaneous breathing, reflects a component of airway resistance from air flow26. Cst ranged from 55.2 to 165.8 ml/cm H2O. Normal values for Cst near FRC range from 226 to 428 ml/cm H2O (Table 2)27. Cdyn was reduced in all patients, ranging from 28.5 to 115.3 ml/cm H2O (normal 150–390 ml/cm H2O)27. The results confirm “stiff lungs” in these patients despite the absence of parenchymal disease on imaging.
Chest CT reformatting
In all patients with available digital CT imaging, lung volumes near TLC were markedly low compared with predicted values (Appendix 2)18. Lung density was increased uniformly throughout the lung fields, a finding also evident in both SLS patients with available CT data who were not studied with esophageal manometry. Increased lung density is indicative of pulmonary edema, atelectasis, or parenchymal remodeling28,29.
Clinical course
Clinical outcome data were available for 4 patients (Table 1). After treatment, SLS symptoms resolved in Cases 1, 2, and 5. Case 1 is discussed further below. Case 2 improved after therapy with cyclophosphamide and theophylline, having failed rituximab. Case 5 improved with corticosteroids and mycophenolate mofetil. Case 6 remains symptomatic, rituximab and cyclophosphamide having failed. Cases 3 and 4 were lost to followup.
Manometry data both before and after successful therapy were available for Case 1, an adolescent with mixed connective tissue disease. After failure to respond to intravenous methylprednisolone, oral corticosteroids 80 mg/day, and theophylline, she received rituximab 1 g intravenously, methylprednisolone 100 mg, and oral corticosteroids. Her dyspnea improved within 7 weeks of therapy. Repeat study when she was asymptomatic (22 months after initial evaluation) found that her TLC had increased from 50% to 66% of predicted. MIPes at FRC increased from 42.6 to 84.4 cm H2O, and MIPes at TLC from 14.5 to 21.6 cm H2O, reflecting an increase in respiratory muscle strength and improved chest wall expansion at high lung volumes. However, Cst and Cdyn remained low (85.7 ml/cm H2O and 47.3 ml/cm H2O, respectively). Repeat chest imaging showed resolution of the right-side pleural effusion; lung volumes increased and parenchymal density decreased but failed to normalize (Figure 2, Appendix 2).

Chest computed tomography reformatted, volume-rendered images depicting lung volumes during symptomatic SLS and after recovery in Case 1. Irregularity of the surface of both lungs during symptomatic disease (left panel) reflects reduced lung volumes due to pleural effusions and potentially other factors. Resolution of pleural effusions in the recovery phase (right panel) was accompanied by improved lung volumes and densities.
DISCUSSION
SLS is a recognized complication of SLE and related autoimmune disorders, but its pathophysiology remains essentially unknown. We found several concurrent respiratory abnormalities in almost all patients studied. These included significantly impaired inspiratory pressures at TLC in 5 patients and reduced lung compliance in all. Thus, patients exhibited both intrinsic (parenchymal) and extrinsic (extrapulmonary) causes of restrictive lung disease. Importantly, in each case, pleural inflammation was evident early in the disease course.
As noted, extrinsic restriction can be either structural or functional. Structural causes of extrinsic restriction include chest wall deformities (not present in these patients) or pleural adhesions as seen after pleurodesis or in asbestos-related fibrosis30,31. Such patients typically have radiographically obvious pleural disease31. Although most patients in our series had small pleural effusions at some point in their course, as is typical for SLS, no patient exhibited chronic pleural findings. Additionally, 3 cases followed through recovery had resolution of dyspnea and improvement in TLC, weighing against fixed adhesions. Finally, in 1 case, adhesions between the lung and diaphragm or chest wall were specifically excluded by ultrasound imaging. Based on these observations, we conclude that the extrinsic restriction observed in our patients was not structural.
Functional extrinsic restriction arises from impaired activity of the respiratory muscles. Diffuse respiratory myopathy is unlikely since our patients had normal muscle enzymes, no clinical evidence for concurrent myositis elsewhere, and adequate inspiratory strength at FRC. Rather, inspiratory pressures were impaired selectively at high lung volumes, suggesting an alternative pathophysiology. Respiratory muscle function is regulated not only by volition but also through neuronal reflex arcs. These include the intercostal-phrenic and pleural-phrenic reflexes, which are activated by stimulation of intercostal and pleural afferents, respectively, leading to phrenic nerve inhibition32,33,34,35,36,37,38. In animals, the intercostal-phrenic reflex can be triggered by chest wall compression and rib vibration. After such stimuli, phrenic nerve electrical activity and diaphragm electromyographic recordings are decreased37. The pleural-phrenic reflex can also be activated by exposure of the pleura to inflammatory cytokines38. These reflexes have been documented in humans and may be responsible for decreased inspiratory capacity in post-operative patients39. They are particularly potent at higher lung volumes37. Since all cases had evidence of pleuritis, an observation noted in other series9,14,15, pleural inflammation appears the most likely basis for engagement of these neural arcs, resulting in reflex (and potentially volitional) limitation of chest expansion. This possibility is supported by the observation that recovery in 3 patients coincided with resolution of pleuritic chest pain and effusions on chest imaging, and with normalization of MIPes at TLC measurement in the single patient retested in remission.
Importantly, lung compliance was reduced in all individuals, and lung density was increased in all patients evaluated by chest CT reformatting. The basis for these findings is uncertain. Because all patients had intact corrected DLCO values and radiographically normal lung parenchyma, substantial interstitial lung disease is unlikely. Elevated lung density may simply reflect lower lung volumes. However, impairment of lung compliance, not explained by interstitial disease or atelectasis, has been observed in patients who are chronically restricted to lower lung volumes due to spinal cord injury or muscular dystrophy; tissue remodeling with changes in elasticity is proposed as the underlying pathophysiology40,41,42. Such hypoinflation-induced decrease in compliance could contribute to the progressive expression of SLS, since stiff lungs are more difficult to inflate. Notably, the single patient with intact MIPes at TLC had the lowest lung compliance, suggesting that the contribution of different aspects of respiratory dysfunction in SLS may vary from patient to patient.
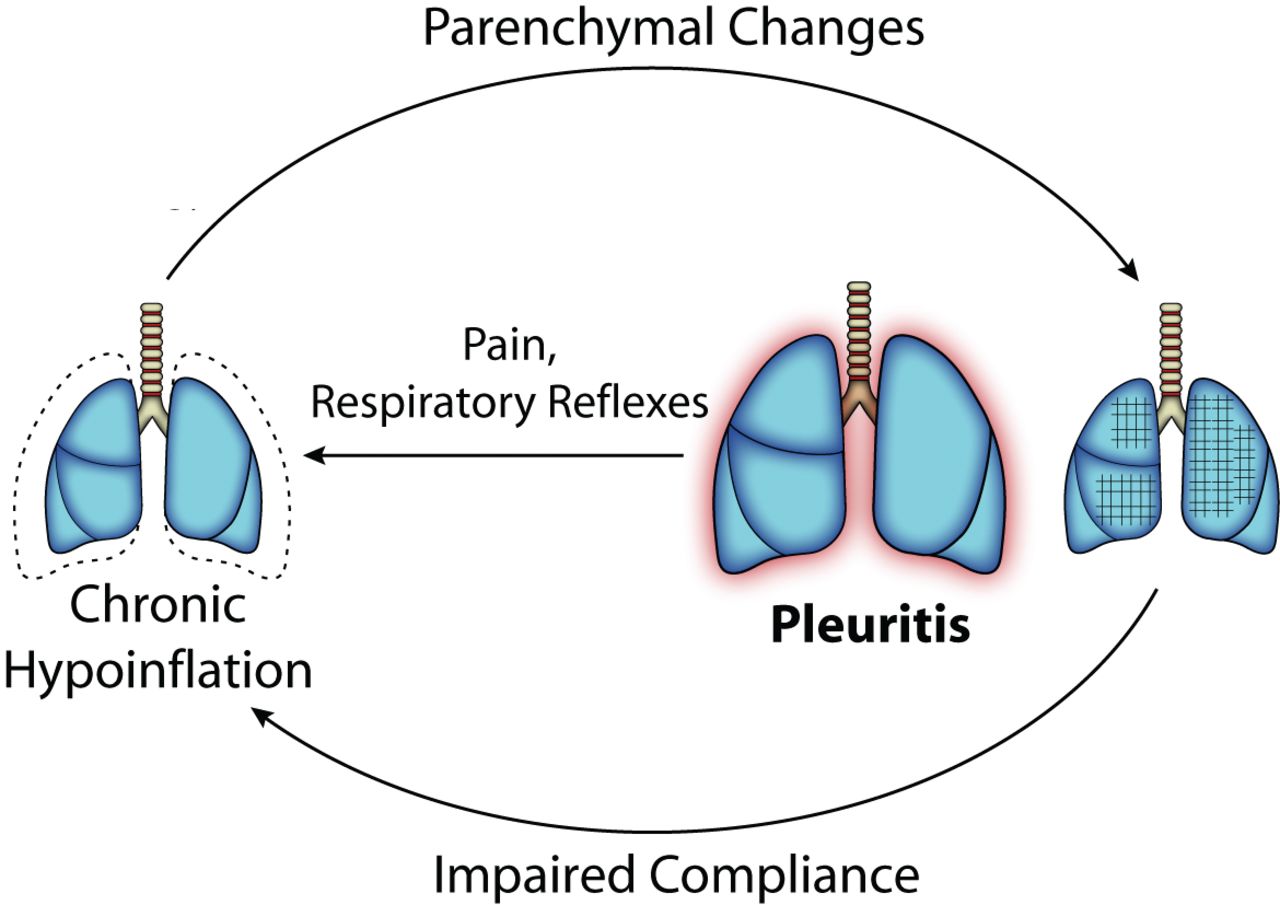
Together, these physiologic findings suggest a new model of the pathogenesis of SLS (Figure 3). Pleural inflammation triggers inhibition of deep inspiration by neural reflexes and pain (demonstrated by decreased MIPes at TLC) resulting in chronic lung hypoinflation, which in predisposed patients leads to parenchymal remodeling that decreases lung compliance. Impaired compliance worsens hypoinflation, initiating a positive feedback loop that helps to explain the gradual progression of SLS. Since this defect is primarily functional, the patient’s ventilatory drive would be expected to limit further respiratory deterioration, accounting for the low mortality of SLS despite its alarming clinical presentation.

Model of the pathophysiology of shrinking lung syndrome (SLS). We propose that SLS begins with pleural inflammation due to the underlying rheumatic disease. Activation of local neural reflexes and/or volitional splinting because of pain leads to chronic hypoinflation of the lung, which gradually impairs lung compliance through undefined parenchymal changes. The less compliant lung is more difficult to inflate, leading to a slowly progressive spiral of declining inflation until the positive feedback cycle is halted, likely by the patient’s central respiratory drive.
Our results are inconsistent with conventional hypotheses implicating isolated diaphragmatic weakness or phrenic dysfunction in the pathogenesis of SLS. While it has been suggested that SLS may arise from extrinsic restriction mediated by neuronal reflexes9,14,15, our study is the first to provide physiologic evidence supporting this hypothesis, through documentation of reduced MIPes at TLC. Additionally, we have demonstrated that patients with SLS have impaired pulmonary compliance, a key new finding that implicates parenchymal remodeling in SLS, and without which the gradual deterioration characteristic of SLS would remain unexplained. Lung compliance in patients with SLS did not necessarily normalize even in patients who had symptomatically recovered. This result suggests that structural changes may persist even after symptomatic recovery, a new concept in SLS that will need to be considered in future research.
Our study has several limitations. Most significantly, the series is small. While a small sample size typically raises concern about sampling error and generalizability, we are reassured by several considerations. First, SLS is an extremely rare condition in most surveys of SLE and related autoimmune diseases, and the cases studied in detail represented two-thirds of all the cases seen by > 50 practicing rheumatologists in 2 large tertiary care referral centers over the course of 4 years. The 3 cases not studied were phenotypically similar to the studied cases; both the patients not studied who had CT data exhibited lung density findings concordant with those of patients receiving esophageal manometry; and the grounds for failure to study the 3 missed patients are well understood and do not raise concern for selection bias. Second, among SLS patients studied fully, our findings were remarkably consistent: 5 of 6 had selectively impaired inspiratory force at high lung volumes, while all 6 had markedly impaired parenchymal compliance in the absence of abnormalities on conventional high-resolution CT imaging. Among the 5 patients for whom reformatted CT scans were available, all 5 exhibited abnormally high lung density, confirming the parenchymal abnormality identified through manometry. Therefore, despite a small sample size, our results are highly likely to reflect the physiology of most patients with SLS, at least as seen at similar referral centers.
Other limitations of our study arise out of the methodology used to evaluate patients. As pleural adhesions can be masked on imaging by the presence of pleural effusions, direct thoracoscopic visualization of the pleura would have been preferable, but was not considered clinically justified. Further, pulmonary physiologic tests are dependent on patient effort, and it would have been of interest to assess maximal respiratory muscle strength by magnetic phrenic nerve stimulation and diaphragmatic electromyography. However, such studies performed in SLS have demonstrated no limitations, justifying their omission here9,43.
Several key questions remain unanswered. Pleuritis is common in rheumatologic and nonrheumatologic conditions, yet SLS is rare. Lupus pleuritis usually responds to corticosteroids, while corticosteroids are often ineffective in SLS44. It may be that the duration of pleural inflammation, the location of the inflammation within the pleura (apical vs the zone of apposition), intersubject variability in the potency of respiratory reflexes, or differential susceptibility to hypoinflation-induced parenchymal changes could explain these observations. The character of the changes in pulmonary compliance and its potential reversibility remain unknown. Pathologic samples from patients with active SLS and in remission will be essential to understand these alterations in the lung parenchyma.
Our data support the hypothesis that SLS represents an unusual complication of pleuritis, whereby inhibited respiratory muscle engagement limits inflation and thereby leads to progressive loss of lung compliance. The proposed model of SLS has implications for future research and therapy. If the primary driver of the disease is pleuritis, then antiinflammatory therapy should be implemented early. If impaired lung expansion contributes to impaired lung compliance, pleuritic chest pain should be addressed with analgesia and pulmonary rehabilitation. These possibilities will require clinical validation.
Acknowledgment
We are grateful to Dr. Bartolome Celli for careful review of the manuscript and to Dr. Luis Leon for graphic assistance with Figure 3.
Appendix
Presentation of shrinking lung syndrome (SLS) in 3 female subjects who did not undergo evaluation of pulmonary mechanics. Subjects A and B presented before esophageal manometry was routine at our institutions; Subject C had comorbidities that rendered study impractical. The results demonstrate that these subjects were phenotypically similar to the 6 patients tested.
Appendix
Total lung volume and lung densities. Chest computed tomography reformatting results are provided for 5 cases included in the series (digital image data were unavailable for Case 2) as well as for Subjects B and C, who were both seen over the study interval but who did not undergo esophageal manometry. Predicted total lung volumes are based on normalized values for total lung capacity obtained through helium dilution or plethysmography. Repeat imaging with reformatting was available for Case 1 during remission and for Case 5 during symptom improvement but not full recovery. Lung density was measured in Hounsfield units (HU) from the reformatted images; this scale is used to describe radiodensity, with lower values representing less dense images.
Footnotes
-
Dr. Nigrovic is supported by the Cogan Family Fund and the Samara Jan Turkel Center for Autoimmune Diseases. Dr. Dellaripa participates in clinical trials conducted by Genentech; however, no financial support was provided for this work. Dr. Loring was supported by HL52586 from the US National Institutes of Health. Dr. Liao is supported by K08 AR060257 from the National Institutes of Health and the Katherine Swan Ginsburg Fund.
- Accepted for publication November 6, 2012.








{kind=link}
{kind=link}
{kind=link}