

Abstract
Objective. To investigate the features of ankylosing spondylitis (AS) and nonradiographic axial spondyloarthritis (nr-axSpA) in a Canadian cohort of 639 patients with AS and 73 patients with nr-axSpA.
Methods. Clinical and laboratory data were compared for patients with AS and nr-axSpA enrolled in a longitudinal SpA cohort.
Results. The proportion of male patients was higher in AS than in nr-axSpA (76.2% vs 47.9%; p < 0.0001). There was no difference in the presence of HLA-B27 between AS (78.9%) and nr-axSpA (72.5%) patients, nor in age at the time of diagnosis, although AS patients were younger at the time of symptom onset (23.9 yrs vs 26.4 yrs; p = 0.03). Disease duration at the time of last clinic visit was longer for AS than for nr-axSpA patients (17.7 yrs vs 12.1 yrs; p = 0.0002). Acute-phase reactants were higher in AS than in nr-axSpA (C-reactive protein 11.4 vs 5.2, p < 0.0001; erythrocyte sedimentation rate 13.7 vs 9.9, p = 0.02). The Bath Ankylosing Spondylitis Metrology Index was higher in patients with AS (2.84 vs 1.35, p < 0.0001).
Conclusion. Patients with nr-axSpA were more likely to be female and to have lower inflammatory markers than patients with AS. When restricted to female patients only, acute-phase reactants did not differ significantly between AS and nr-axSpA. The evidence provides indirect support for the concept that nr-axSpA may represent an early form of AS, but that also has features of a distinct disease entity with significant burden of symptoms.
Historically, ankylosing spondylitis (AS) has been defined by the modified New York classification criteria1, which require the presence of radiographic sacroiliitis. More recently the use of magnetic resonance imaging (MRI) for earlier detection of inflammation in the sacroiliac joints has led to the identification of patients with features of axial spondyloarthritis (SpA) who do not fulfill the modified New York criteria (nonradiographic axial SpA; nr-axSpA). The Assessment of Ankylosing Spondylitis International Society (ASAS) has developed criteria for the classification of patients with axial SpA, including those with nr-axSpA2,3. However, the natural history of axial SpA is not completely understood.
It has been proposed that nr-axSpA may represent a form of AS that is seen at an earlier stage of what is essentially a single disease entity4. This notion is supported by the finding that some patients do progress to AS over time. An early study of 54 patients with suspected AS but nondiagnostic sacroiliac joint radiographs demonstrated that over 10 years, 59% progressed to radiographic AS5. In a study of undifferentiated SpA, the progression to AS was 10% over 2 years and 23.3% over 5 to 10 years6,7. Analysis of the German Spondyloarthritis Inception Cohort (GESPIC) found that of 95 patients with nr-axSpA, 11.6% progressed to AS over 2 years. Elevated CRP was the strongest predictor of progression to AS8.
However, there remain a number of patients who have not progressed to AS over the duration of these studies. This observation, along with the identification of genetic and other differences between the 2 groups, has led to the concept of nr-axSpA as a distinct disease entity. Data supporting this proposal are drawn largely from European cohorts and are summarized in a recent review9. A lower frequency of HLA-B27 in nr-axSpA was observed in GESPIC7 and in 2 trials of adalimumab in nr-axSpA, 1 performed in Germany10 and 1 an international multicenter trial11. Sex differences between the 2 groups have been demonstrated in 3 German studies with the percentage of males ranging from 31% to 43% in nr-axSpA compared with 65% to 77% in AS8,12,13. In general, disease activity and burden of symptoms did not differ although CRP levels were lower in nr-axSpA12.
In our study, we aimed to expand the current understanding of axial SpA by describing the commonalities and differences between subgroups of axial SpA in a longitudinal prospective North American SpA cohort.
MATERIALS AND METHODS
Patients attending the Toronto Western Spondylitis Clinic were invited to be registered in the SpA database. All patients provided written consent and the study was approved by Toronto University Health Network research ethics board. Clinical, laboratory, and radiological data are collected annually. Data were analyzed for all patients enrolled between January 2003 and December 2012 meeting modified New York criteria for AS or ASAS classification criteria for nr-axSpA. All patients had a clinical diagnosis of axial SpA made by a rheumatologist and were subsequently classified according to the criteria above. Statistical analyses were performed using GraphPad Prism 6 software. Categorical variables were compared using Fisher’s exact test with 2-tailed p values. For continuous variables, a mean patient value was calculated based on all visits for that patient. Variables were compared using t tests.
RESULTS
Six hundred and thirty-nine patients with AS and 73 patients with nr-axSpA were included. Of the patients with nr-axSpA, 40 demonstrated inflammation on MRI and 33 were classified according to ASAS clinical criteria for axial SpA (of whom 15 had MRI showing no inflammation and 18 did not have MRI performed). Patient and disease characteristics are summarized in Table 1.
Disease characteristics of the axial spondyloarthritis (SpA) population.
Patient demographics
The proportion of male patients was higher in AS than in nr-axSpA (76.2% vs 47.9%; p < 0.0001). There was no difference in age at the time of diagnosis but patients with AS were younger at the time of symptom onset (23.9 yrs vs 26.4 yrs; p = 0.03). Disease duration at the time of last clinic visit was longer for AS than for patients with nr-axSpA (17.7 yrs vs 12.1 yrs; p = 0.0002).
Disease characteristics
There was no significant difference in the presence of HLA-B27 between patients with AS (78.9%) and patients with nr-axSpA (72.5%). Acute-phase reactants were higher in AS than in nr-axSpA [C-reactive protein (CRP) 11.4 vs 5.2, p < 0.0001; erythrocyte sedimentation rate (ESR) 13.7 vs 9.9, p = 0.02). The Bath Ankylosing Spondylitis Metrology Index was higher in patients with AS (2.84 vs 1.35; p < 0.0001). Higher rates of fibromyalgia (FM) were seen in nr-axSpA than in AS. There was a trend for more unemployment due to disability in patients with AS.
Medication usage
The proportion of patients having ever or currently using a biologic drug were similar, as were the proportion treated with nonsteroidal antiinflammatory drugs, disease-modifying antirheumatic drugs, and glucocorticoids.
Role of sex and inflammation
Further investigation of sex, inflammation, and radiographic severity revealed that almost one-third (31.9%) of patients with a normal CRP were female, compared to only 14.6% of patients with an elevated CRP (p < 0.0001). When data were analyzed for the female patients only (n = 191), the difference in acute-phase response between AS and nr-axSpA lost significance (CRP 9.4 vs 5.2, p = 0.09; ESR 16.3 vs 11.5, p = 0.07). The difference in Bath Ankylosing Spondylitis Metrology Index remained significant (2.1 vs 1.3, n = 0.02).
DISCUSSION
We have described a cohort of patients with nr-axSpA enrolled in a longitudinal prospective study. These data add to the current understanding of the spectrum of SpA and raise questions about the concept of nr-axSpA, described in Figure 1.
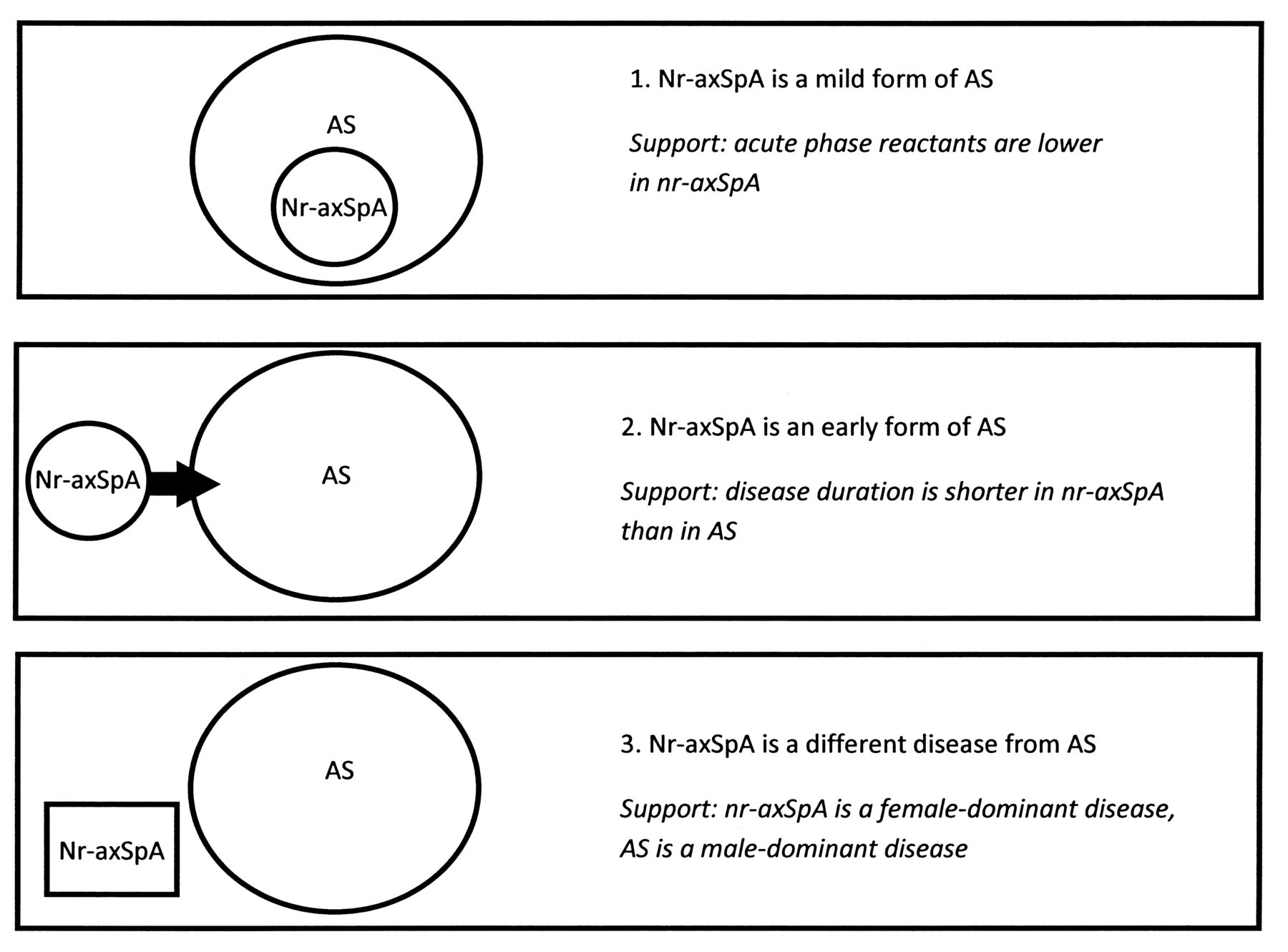
The concept of nonradiographic axial spondyloarthritis (nr-axSpA): 3 theories. AS: ankylosing spondylitis.
Our data support previous findings that levels of inflammation as reflected by acute-phase reactants are lower in nr-axSpA than in AS12, providing support for the theory that in some cases, nr-axSpA may represent a mild form of AS.
The relatively long mean duration of disease (over 12 yrs) in the nr-axSpA population at the time of the last clinic visit suggests that many of these patients will never progress to radiographic AS, but further work is required to investigate predictors of progression. Disease duration at last clinic visit was shorter in nr-axSpA than AS, providing some indirect support to the notion that nr-axSpA may represent a subset of axial SpA seen earlier in the course of the disease than AS.
Patients with nr-axSpA, in contrast to those with AS, were predominantly female, as was observed in GESPIC13, where 57.1% of patients with nr-axSpA were female. Overall there is a significant difference in markers of inflammation, as reflected in CRP and ESR, between nr-axSpA and AS. This difference persisted when female nr-axSpA and female AS patients were compared, although significance was lost, probably because of small patient numbers. The basis for the lower levels of inflammation in females has not yet been resolved. Exogenous estrogens in the form of oral contraceptives are associated with earlier age of onset of AS in women with AS14, whereas pregnancy in general does not seem to alter the clinical course of AS15.
We did not find a lower rate of HLA-B27 positivity in the nr-axSpA population, but positivity for HLA-B27 was a requirement for inclusion in the study of patients classified according to clinical criteria. Comparison of HLA-B27 carrier frequencies between subsets of patients is problematic when positivity is a requirement for the classification of a subgroup. However, the similarities in frequency of HLA-B27 and extraarticular manifestations (uveitis, psoriasis, and inflammatory bowel disease) among AS and nr-axSpA patients support the theory that nr-axSpA and AS are not different diseases, but represent variable phenotypes within the same disease spectrum.
We noted a comparable delay from symptom onset to diagnosis in both patient groups. The delay to diagnosis in AS may be as long as 10 years16 and is often attributed to the slow development of radiographic sacroiliitis. However, we did not find that patients with nr-axSpA were diagnosed any sooner after symptom onset than AS patients, despite reliance on features other than radiographic sacroiliitis for the diagnosis. This observation highlights the need for increased awareness in the medical community of the clinical features of SpA and for strategies to improve detection.
Our study is limited because the data represent a tertiary SpA center and may not be generalizable to the SpA population as a whole. About one-third of all patients were taking biologic therapy, which would affect disease outcome measures including acute-phase reactants. However, the proportion of patients taking biologic therapy was similar between the 2 groups and the differences seen in levels of inflammation are, therefore, likely to be independent of biologic use. Excluding patients treated with biologic therapy, as has been done in previous studies12, would restrict the analysis to patients with mild disease or recent disease onset. Biologic use appears to fall off with time in nr-axSpA, with 42% of patients ever taking a biologic, but 34% currently taking a biologic. The prevalence of FM was twice as high in nr-axSpA as in AS and this might explain the apparent lower persistence with biologics. It would be interesting to compare the features and outcomes within the nr-axSpA subset according to MRI positivity or negativity, but MRI data were not available for all patients in this observational study.
The symptomatic burden of disease is comparable for axSpA subsets, but modifying factors such as sex appear to affect the structural consequences for the spine in nr-axSpA. The evidence provides indirect support for the concept that nr-axSpA may represent an early form of AS, but that also has features of a distinct disease entity with a significant burden of symptoms.
Footnotes
-
D. Wallis was partly funded by an Assessment of Ankylosing Spondylitis International Society fellowship and received research fellowship support from Janssen Pharmaceuticals.
- Accepted for publication August 13, 2013.








{kind=link}