

Abstract
Objective. Assessment of associations of nailfold videocapillaroscopy (NVC) scleroderma (systemic sclerosis; SSc) (“early,” “active,” and “late”) with novel future severe clinical involvement in 2 independent cohorts.
Methods. Sixty-six consecutive Belgian and 82 Italian patients with SSc underwent NVC at baseline. Images were blindly assessed and classified into normal, early, active, or late NVC pattern. Clinical evaluation was performed for 9 organ systems (general, peripheral vascular, skin, joint, muscle, gastrointestinal tract, lung, heart, and kidney) according to the Medsger disease severity scale (DSS) at baseline and in the future (18–24 months of followup). Severe clinical involvement was defined as category 2 to 4 per organ of the DSS. Logistic regression analysis (continuous NVC predictor variable) was performed.
Results. The OR to develop novel future severe organ involvement was stronger according to more severe NVC patterns and similar in both cohorts. In simple logistic regression analysis the OR in the Belgian/Italian cohort was 2.16 (95% CI 1.19–4.47, p = 0.010)/2.33 (95% CI 1.36–4.22, p = 0.002) for the early NVC SSc pattern, 4.68/5.42 for the active pattern, and 10.14/12.63 for the late pattern versus the normal pattern. In multiple logistic regression analysis, adjusting for disease duration, subset, and vasoactive medication, the OR was 2.99 (95% CI 1.31–8.82, p = 0.007)/1.88 (95% CI 1.00–3.71, p = 0.050) for the early NVC SSc pattern, 8.93/3.54 for the active pattern, and 26.69/6.66 for the late pattern versus the normal pattern.
Conclusion. Capillaroscopy may be predictive of novel future severe organ involvement in SSc, as attested by 2 independent cohorts.
- NAILFOLD VIDEOCAPILLAROSCOPY
- PREDICTION
- ORGAN INVOLVEMENT
- DISEASE SEVERITY MEDSGER SCALE
- SYSTEMIC SCLEROSIS
The clinical expression and course of scleroderma (systemic sclerosis; SSc) may be coupled with serious morbidity and mortality1. No therapies have been proven through randomized controlled trials to halt the natural evolution of the disease or to efficaciously treat organ complications. If preventive therapy for organ involvement ever becomes available, it would be beneficial to know which patients are prone to developing certain organ complications. Ideally, treatment could be initiated in a timely fashion in such a population. Consequently, effort is being put into investigating possible biomarkers. Capillaroscopy may be a candidate as a possible biomarker. Recently, we attested prediction of future severe organ involvement (e.g., peripheral vascular disease) in a SSc population [regardless of presence of organ involvement at baseline (initial evaluation)] by baseline capillaroscopic patterns2. The 3 aims of our study are to (1) assess whether strictly novel future severe clinical involvement in any of the possible affected organ systems (9 organ systems according to the Medsger disease severity scale) in SSc can be predicted by baseline capillaroscopic patterns3; (2) determine whether this finding can be validated in an independent cohort; and (3) determine whether prediction per separate organ system can be attested.
MATERIALS AND METHODS
Patients
Sixty-six consecutive patients with SSc, visiting the Scleroderma Clinic of the Ghent University Hospital, were enrolled (Appendix 1).
A validation cohort consisted of 82 consecutive Italian SSc patients (Appendix 2).
Collection and blinding of the NVC images
In short, the nailfolds of the second, third, fourth, and fifth fingers were examined bilaterally in each patient using an optical probe videocapillaroscope equipped with a 200× magnification contact lens and connected to image analysis software (Videocap; DS MediGroup). The images were made anonymous before being assessed. Four consecutive fields, extending over 1 mm in the middle of the nailfold, were studied per finger4.
Classification of capillaroscopic images
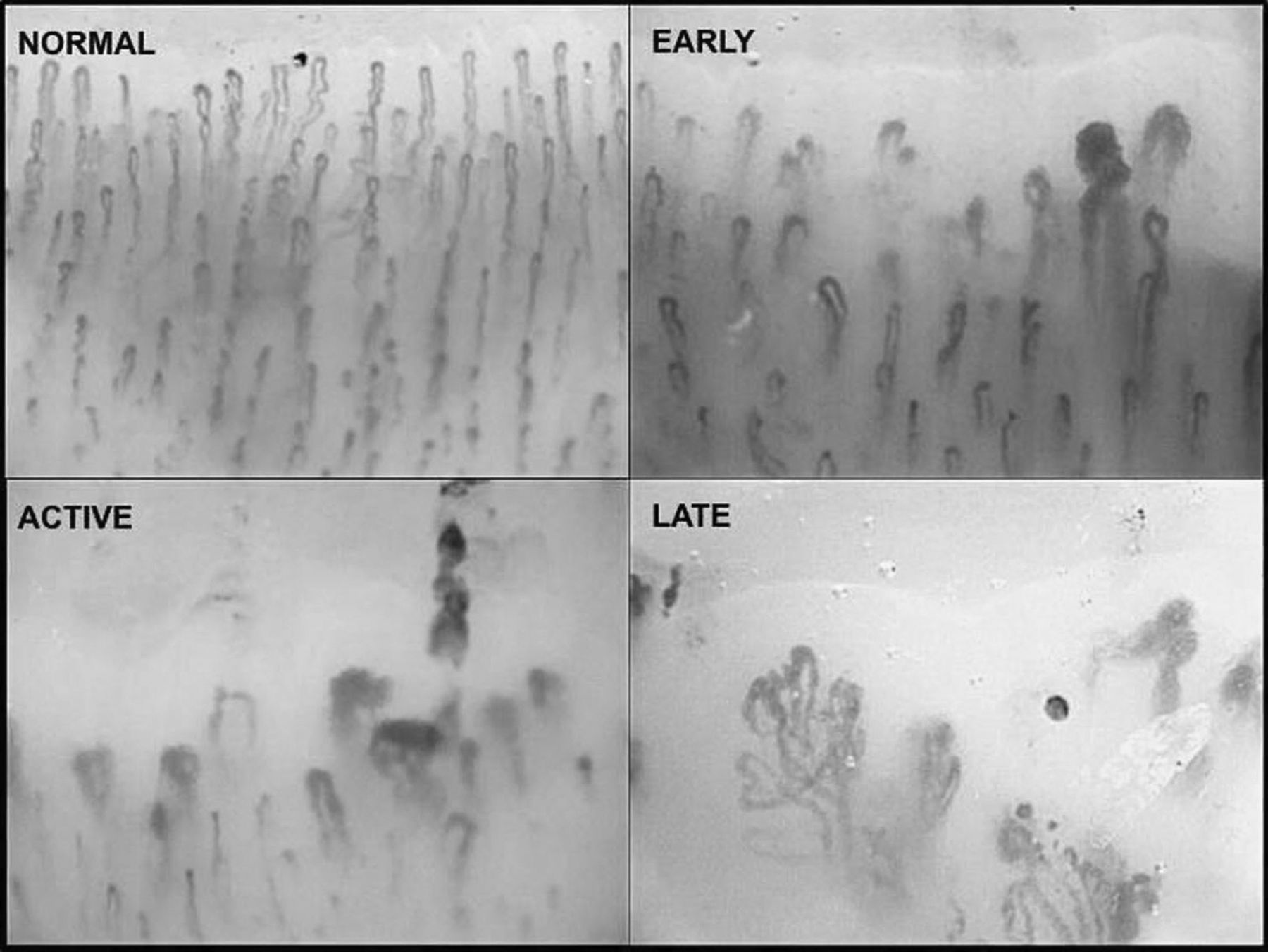
Images were classified into the “early,” “active,” or “late” SSc patterns or “normal and aspecific changes,” as described (Figure 1)5,6. Early NVC SSc pattern was defined as the combination of a few enlarged/giant capillaries, few capillary microhemorrhages, a relatively well-preserved capillary distribution, and no evident loss of capillaries. Active NVC SSc pattern was defined as frequent giant capillaries, frequent capillary microhemorrhages, moderate loss of capillaries, mild disorganization of the capillary architecture, and absent or mild ramified capillaries. Late NVC SSc pattern was defined as irregular enlargement of the capillaries, few or absent giant capillaries and microhemorrhages, severe loss of capillaries with large avascular areas, disorganization of the normal capillary array, and ramified/bushy capillaries. Normal NVC pattern was defined as a regular distribution of the capillaries without capillary loss and a morphology without specific changes or aspecific changes.

Qualitative assessment of capillaroscopic images (200×): normal capillary pattern, early capillary pattern, active systemic sclerosis (SSc) pattern, and late SSc pattern.
Definition of more severe SSc patterns
Because SSc is recognized to be a progressive obliterative microvasculopathic disease, the borders between the consecutive NVC patterns are delineated, between others, by gradually more severe capillary loss. To reflect this, as described, the terminology “more severe” NVC patterns is used throughout our article2,7,8,9.
SSc-specific antibody detection
Anticentromere and antitopoisomerase were detected by the INNO-LIA ANA Update (Innogenetics). Anti-RNA polymerase III and anti-PM/Scl were identified by the Systemic Sclerosis (Nucleoli) Profile Euroline (IgG) lineblot assay (Euroimmun)10.
Clinical measurements
Clinical evaluation was performed for 9 organ systems at baseline and at the future visit (18–24 months of followup). Nine organ systems (general, peripheral vascular, skin, joint, muscle, gastrointestinal tract, lung, heart, and kidney) were investigated according to the Medsger disease severity scale (DSS: scale with categories 0, 1, 2, 3, and 4)3. Lung involvement was additionally subdefined as pulmonary arterial hypertension (PAH) or interstitial lung disease (ILD) (Appendix 3).
Novel future severe disease for any of the organ systems was defined as having, at the future visit (18–24 months of followup), a category 2 or higher in any of the 9 organ systems assessed according to the Medsger DSS or a novel PAH or ILD, which had been nonexistent at the baseline visit2.
Statistical methods
Prediction of novel future severe organ involvement in any of the 9 organ systems by the NVC patterns was investigated by simple and multiple logistic regression analysis in the Belgian cohort and reported as OR. To validate these findings, this analysis was afterward reperformed separately in an independent Italian cohort. In line with the small sample size of a pilot study, likelihood ratio p-values were reported, because reporting these is appropriate when dealing with small sample sizes11. In line with the characteristic gradual capillary loss of the disease, reflected in the definition of the SSc patterns, a linear effect in the natural logarithmic odds for novel future organ involvement was assumed when statistically meaningful.
Given the similar OR from the Belgian and Italian dataset for prediction of organ involvement in any of the 9 organ systems, these datasets were combined to investigate those separate organ systems in which enough events were present to have enough power to detect possible predictive associations.
Statistical analyses were performed using SPSS version 19 (SPSS Inc.) and R version 2.13.0 (R Foundation for Statistical Computing).
RESULTS
Prediction of novel future severe organ involvement in the Belgian cohort
Descriptives of the Belgian patients are in Appendix 1. In the Belgian cohort, 25/55 patients (45%) had novel future severe organ involvement in any of the 9 organ systems (Appendix 4). A statistically significant and clinically meaningful association was found between the baseline NVC patterns and novel future severe organ involvement in any of the 9 organ systems in the Belgian cohort, with higher prevalences of novel future severe organ involvement according to more severe NVC patterns (Appendix 5). The estimated OR, after simple and multiple logistic regression analysis (adjusting for disease duration, Leroy subset, and vasoactive medication), to develop novel future severe organ involvement was stronger according to more severe NVC patterns (Table 1). These OR pointed in the same direction as the ones attested to by the independent analysis on a separate Italian cohort.
Similar OR in the Belgian cohort and an independent Italian validation cohort to predict novel future severe organ involvement based on baseline SSc patterns.
Prediction of novel future severe organ involvement in the Italian cohort
For descriptives of the Italian cohort see Appendix 2. In the independent Italian cohort a similar percentage, 39% of patients (31/79), as in the Belgian cohort, had novel future severe organ involvement in any of the 9 organ systems (Appendix 6). In the Italian cohort, parallel with the Belgian cohort, a statistically significant and clinically meaningful association was found between the baseline NVC patterns and novel future severe organ involvement in any of the 9 organ systems, with higher prevalences of novel future severe organ involvement according to more severe NVC patterns (Appendix 7). Also, the OR to develop novel future severe organ involvement were in accordance with the Belgian cohort (Table 1).
Prediction of novel future peripheral vascular involvement in the combined Italian-Belgian cohort
Even though in both cohorts baseline capillaroscopy independently attested an overall prediction in any of the 9 organ systems, neither the Belgian cohort by itself nor the Italian cohort was powered to statistically correctly perform prediction analyses per separate organ system. Combining the 2 databases (which was statistically allowable given the comparable percentage of novel future severe events and similar odds) gave one of the 9 organ systems, more specifically the peripheral vascular organ system, enough events to be able to perform logistic regression analysis (Table 2a and 2b).
Novel future severe organ involvement [9 organ systems according to the Medsger disease severity scale and lung subdefined into interstitial lung disease (ILD) and pulmonary arterial hypertension (PAH)] in the Italian-Belgian (n = 148) cohort.
Association between baseline nailfold videocapillaroscopy (NVC) patterns and novel future (month 18–24) severe organ involvement in the peripheral vascular organ system in the Italian-Belgian cohort.
In this way, 19/140 patients (14%) had novel future severe peripheral vascular involvement in the combined Italian-Belgian cohort.
Again, higher prevalences of novel future severe peripheral vascular involvement occurred according to more severe NVC patterns. In this way, 0/13 patients (0%) with a normal NVC pattern, 2/33 (6%) with an early, 8/46 (17%) with an active, and 9/48 (19%) with a late NVC pattern had novel future severe peripheral vascular disease. In simple logistic regression analysis, the OR in the Italian-Belgian cohort was 1.90 (95% CI 1.08–3.65, p = 0.02) for the early, 3.60 for the active, and 6.86 for the late NVC SSc pattern versus the normal pattern.
In multiple logistic regression analysis, adjusting for disease duration, subset, and vasoactive medication, the OR was 2.96 (95% CI 1.45–7.05, p = 0.002) for the early, 8.78 for the active, and 26.01 for the late NVC SSc pattern versus the normal pattern.
DISCUSSION
Our study demonstrates that qualitative assessment of capillaroscopy, performed at a baseline consultation, may be able to predict which patients with SSc may develop novel future severe organ involvement in any of the 9 organ systems, as described by Medsger1,3,12,13,14.
The value of our study is varied. First, these findings allow capillaroscopy to position itself as a candidate biomarker in SSc. Second, the findings of the Belgian study were replicated in an independent, consecutive, Italian cohort, which is an indirect validation of the findings. Third, both cohorts were underpowered to also investigate whether capillaroscopy may be predictive in any of the separate organ systems. Nevertheless, after combination of the 2 cohorts, capillaroscopy could indeed attest to the predictive ability of novel future severe peripheral vascular involvement in patients with SSc. Fourth, this study highlights the heterogeneous aspect of the disease. In this way, not all patients develop novel future severe organ involvement. More specifically, even though 14% of all patients developed novel future severe peripheral organ involvement, 86% did not. Given this heterogeneity, tools identifying those patients at risk, as was attested in our study, are very welcome in rheumatology.
Three conclusions can be made. One, capillaroscopy may pinpoint those patients with a more severe disease course. This will have implications once disease-modifying drugs for this disease are available. In this way, patients ideally will be able to be treated before the severe disease course sets in. Two, capillaroscopy may pinpoint those patients who will have novel severe peripheral vascular involvement in the future. Three, large, consecutive, longitudinal studies are needed, with enough statistically significant events per organ system to investigate whether capillaroscopy may be predictive of any other organ involvement in SSc.
Acknowledgment
The authors thank their colleagues for sending their patients to the Scleroderma Clinic. We also thank our senior professors for making this collaboration possible.
APPENDIX 1. Descriptives of the Belgian cohort (n = 66).
APPENDIX 2. Descriptives of the Italian cohort (n = 82).
APPENDIX 3.
Pulmonary arterial hypertension (PAH)
As previously described in the Ghent cohort, patients were classified into the “PAH category” if, on right heart catheterization, the mean pulmonary arterial pressure was 25 mm Hg at rest or 30 mm Hg during exercise with a mean pulmonary arterial wedge pressure < 15 mm Hg1. Decision to perform right heart catheterization was made in consensus with the cardiologist (since 2009: mostly a tricuspid regurgitation ≥ 31 mm Hg in combination with a dyspnea New York Heart Association class II, before 2009 a systolic pulmonary arterial pressure of 40 mm Hg on echocardiography). Of note, in the Ghent University Hospital all systemic sclerosis patients are evaluated by a multidisciplinary team with a dedicated rheumatologist, cardiologist and pulmonologist. All patients are seen on baseline, month 6, month 18, and then yearly after. At each visit they are screened by lung function and echocardiography.
In the Italian cohort right heart catheterization was performed upon a systolic pulmonary arterial pressure of 40 mm Hg on echocardiography.
Interstitial lung disease (ILD)
Patients were included in the “new future ILD” category if they met the following criteria: a forced vital capacity ≤ 70% or 10% lowering of the forced vital capacity since the baseline capillaroscopic visit and/or alveolitis or fibrosis on high resolution scan. Exclusion criteria: patients with a forced expiratory/forced vital capacity volume < 65% (exclusion of significant airflow obstruction) or patients with PAH or on treatment with endothelin receptor antagonists, phosphodiesterase type 5 inhibitors, or prostanoids as pulmonary-vascular therapy.
REFERENCE
- 1.↵
APPENDIX 4. Novel future severe organ involvement [9 organ systems according to the Medsger disease severity scale and lung subdefined into interstitial lung disease (ILD) and pulmonary arterial hypertension (PAH)] in the Belgian (n = 66) cohort.
APPENDIX 5. Association between baseline capillaroscopy patterns and novel future severe organ involvement in the Belgian (n = 66) cohort.
APPENDIX 6. Novel future severe organ involvement (9 organ systems according to the Medsger disease severity scale) in the Italian (n = 82) cohort.
APPENDIX 7. Association between baseline capillaroscopy patterns and novel future severe organ involvement.
Footnotes
-
Supported by a grant from the Fonds voor Wetenschappelijk Reuma Onderzoek/Fonds de la Recherche Scientifique en Rhumatologie and by the fund for Scientific Research, Flandres to Vanessa Smith; and by a grant from the Nationale Vereniging voor Steun aan Gehandicapte Personen to Saskia Decuman.
- Accepted for publication August 8, 2013.
In this issue








{kind=link}
Jump to section
- Article
- Abstract
- MATERIALS AND METHODS
- RESULTS
- DISCUSSION
- Acknowledgment
- APPENDIX 1. Descriptives of the Belgian cohort (n = 66).
- APPENDIX 2. Descriptives of the Italian cohort (n = 82).
- APPENDIX 3.
- APPENDIX 4. Novel future severe organ involvement [9 organ systems according to the Medsger disease severity scale and lung subdefined into interstitial lung disease (ILD) and pulmonary arterial hypertension (PAH)] in the Belgian (n = 66) cohort.
- APPENDIX 5. Association between baseline capillaroscopy patterns and novel future severe organ involvement in the Belgian (n = 66) cohort.
- APPENDIX 6. Novel future severe organ involvement (9 organ systems according to the Medsger disease severity scale) in the Italian (n = 82) cohort.
- APPENDIX 7. Association between baseline capillaroscopy patterns and novel future severe organ involvement.
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
- References
- eLetters