

Abstract
Objective. To assess the effects on bone mineral density (BMD) of prolonged anti-tumor necrosis factor (anti-TNF) therapy in patients with spondyloarthritis (SpA); to compare the BMD changes to those observed in SpA patients not treated with anti-TNF; and to identify the predictors of these changes.
Methods. Fifty-nine patients with SpA according to the European Spondylarthropathy Study Group criteria who were treated with anti-TNF therapy for at least 4 years were included. Thirty-four patients with SpA from an international longitudinal observational study (OASIS cohort) were used as a control group. Lumbar spine and hip BMD were measured by dual-energy x-ray absorptiometry at baseline, after 1 year, and after at least 4 years.
Results. Over an average 6.5 years’ followup, the increase in BMD was 11.8% (± 12.8%) at the lumbar spine (p < 0.0001) and 3.6% (± 9.3%) at the great trochanter (p = 0.0001) in patients treated with anti-TNF. At the lumbar spine, the increase was similar in patients with and those without syndesmophytes. BMD changes were significantly higher in the anti-TNF group than in the control group at lumbar spine (p < 0.0001), at femoral neck (p = 0.002), and at trochanter (p = 0.011), but not at total hip (p = 0.062). Multivariate analysis showed that the predictors of lumbar spine BMD changes in the total population were the use of anti-TNF (p < 0.0001) and, in the anti-TNF therapy group, the 1-year lumbar spine BMD change (p = 0.007).
Conclusion. This study shows that prolonged anti-TNF therapy increases lumbar spine and trochanter BMD. This effect should be taken into account before introducing antiosteoporotic treatment in these patients.
Spondyloarthritis (SpA) is a group of inflammatory arthritis that consists of ankylosing spondylitis (AS), reactive arthritis, arthritis/spondylitis associated with psoriasis (PsA), and arthritis/spondylitis associated with inflammatory bowel diseases. Bone manifestations of AS are well studied. AS is a chronic inflammatory disease that primarily affects the axial skeleton. The disease is characterized by new bone formation, which leads to the formation of syndesmophytes and ankylosis of the spine and sacroiliac joints. AS is also associated with systemic osteoporosis that can be observed in early stages of disease1,2,3,4. Patients with AS have an increased risk of vertebral fracture, but not nonvertebral fractures5,6,7,8,9,10. Prevalence of osteoporosis is 14% to 27% at the spine and 4% to 14% at the hip5,9,11,12. Bone loss in AS is related to active disease13 and is observed in AS in patients with sustained inflammation, as assessed by C-reactive protein (CRP)14. Significant correlations between the markers of bone turnover, levels of proinflammatory cytokines, and acute-phase reactants such as CRP and erythrocyte sedimentation rate (ESR)5,14,15 suggest that the systemic inflammatory mediators are involved in the pathogenesis of osteoporosis in patients with AS. Reduction of physical activity, decreased spinal mobility related to pain, subclinical gut involvement, and vitamin D deficiency contribute to osteoporosis. In patients receiving anti-tumor necrosis factor (anti-TNF) therapy, in parallel with significant improvement of symptoms and decrease of the inflammation, a significant increase in lumbar spine and hip BMD has been reported16,17,18. Studies assessing the effect of prolonged anti-TNF therapy on bone mineral density (BMD) in SpA are lacking.
The aims of our study were to assess the BMD effects of prolonged anti-TNF therapy in patients with SpA, to compare these BMD changes to those measured in patients with active SpA without anti-TNF therapy, and to identify the predictors of changes of BMD.
MATERIALS AND METHODS
Study design
This was a retrospective study in a tertiary care center.
Patient populations. Anti-TNF therapy group
Patient selection was based on the following inclusion criteria: diagnosis of SpA according to the European Spondylarthropathy Study Group criteria19, anti-TNF therapy for at least 4 years, and availability of BMD measurements at baseline. Among 469 patients with a diagnosis of SpA who received anti-TNF in our department in 2009, 64 fulfilled these criteria.
Exclusion criteria were previous or current antiosteoporotic treatments (n = 5) at inclusion and the use of another biological therapy (rituximab, n = 1) during followup. The 59 patients remaining formed the study group.
Control group
Subjects in the anti-TNF therapy group were matched with French patients with AS (n = 34) enrolled in the OASIS cohort, an international longitudinal observational study on outcome in AS according to the New York criteria20 conducted before anti-TNF marketing. Followup visits were performed according to a fixed protocol21, including BMD measurements, which were available at baseline and at 1 and 5 years.
For comparison with this group, we retrospectively checked the number of patients from the anti-TNF therapy group who fulfilled the New York criteria: 57 of 59 (96.6%) patients met the criteria, and presence of sacroiliitis was doubtful for 2 patients. All patients in both groups fulfilled the Assessments in Ankylosing Spondylitis Working Group (ASAS) axial spondyloarthropathy criteria22.
Clinical and laboratory assessment
Baseline clinical assessment included age, disease duration, extraarticular manifestations (uveitis, psoriasis, and inflammatory bowel disease), and risk factors for osteoporosis such as smoking, alcohol intake (≥ 2 U/day) and presence of menopause. Height and weight were measured at baseline and during followup using a calibrated machine at the densitometry center.
Current therapies
Use of nonsteroidal antiinflammatory drugs (NSAID), oral corticosteroids, and disease-modifying antirheumatic drugs (DMARD; methotrexate, sulfasalazine) was assessed at baseline and during the followup. Use of antiosteoporotic treatment (bisphosphonates, teriparatide, strontium ranelate) during followup was assessed. Prevalence of vitamin D supplementation was available only during the followup and not at baseline.
The activity and severity of the disease were assessed at baseline and at the final visit using the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functional Index (BASFI), CRP (mg/dl), and ESR (mm/h).
BMD and body composition measurements
BMD (g/cm2 and T scores) and body composition were measured by dual-energy x-ray absorptiometry (DEXA) at baseline, at 1 year [for all patients of the SpA control group and 45/59 patients of the anti-TNF therapy group (14 missing data)], and at the final visit, i.e., after at least 4 years (mean 6.5 ± 1.6 yrs) in the anti-TNF therapy group and after 5 years in the SpA control group. In the anti-TNF therapy group, 7 (11.9%), 15 (25.4%), 22 (37.3%), 8 (13.6%), and 7 (11.9%) patients had performed their final BMD measurement between ≥ 4 and ≤ 5 years, > 5 and ≤ 6 years, > 6 and ≤ 7 years, > 7 and ≤ 8 years, and > 8 and ≤ 10 years, respectively. BMD was determined at the lumbar spine (second to fourth vertebrae) and the upper part of the left femur (total femur, trochanter, and femoral neck). Measurements were taken using a Hologic QDR2000 instrument until November 2001 and afterward with a Hologic Delphi (Hologic Corp.). Comparison of the 2 devices was done for 14 patients on the same day in 2001. Mean differences between BMD measurements were + 1.8% (± 2.0%) for lumbar spine, + 1.8% (± 2.4%) for total hip, + 0.9% (± 1.4%) for trochanter area, and + 0.2% (± 3.0%) for femoral neck. This correction factor was applied to all the measurements performed with Hologic QDR2000 (9 patients in the anti-TNF therapy group at baseline, all patients in the SpA control group at baseline, and for 21 patients at 1 year).
Osteopenia was defined as a T score between −1 and −2.5 standard deviations (SD) and osteoporosis as a T score ≤ −2.5 SD by the World Health Organization (WHO). Changes in BMD after 1 year and at the end of the followup were expressed as relative changes of BMD (%) compared with baseline BMD. Body composition [fat mass (kg and %) and lean mass (kg)] was measured using DEXA from the whole-body scan. Appendicular lean mass and fat mass were derived from regional analysis of the whole-body scans. Body composition measurements were repeated under identical technical conditions during the followup. All examinations were performed according to the manufacturer’s recommendations. Quality control of both devices using the manufacturer’s spine phantom was performed daily during the followup.
Vertebral assessment. Syndesmophyte assessment
Presence of syndesmophytes was assessed at the end of followup, by standard lumbar radiograph for the control group [modified Stoke Ankylosing Spondylitis Spine (mSASS) score obtained from the OASIS database].
For the anti-TNF therapy group, presence of lumbar syndesmophytes was assessed using Vertebral Fracture Assessment (VFA) software on the DEXA device. The diagnosis was directly assessed on the screen by 2 independent readers (AD, JF) using all available techniques of image quality improvement if necessary.
Vertebral fracture
Using VFA, vertebral fractures from T4 to L4 were quantified using the Genant semiquantitative approach23. The severity of the fracture was quantified from grades 1 to 3 for a reduction in anterior, middle, and/or posterior vertebral height of 20% to 25%, 25% to 40%, and > 40%, respectively. Patients were considered as having a fracture over 1 vertebra with at least one grade 1 deformity of osteoporotic origin. The diagnosis was directly assessed on the screen by 2 independent readers blinded to patients’ characteristics.
Anti-TNF treatment
Patients required anti-TNF therapy because of persistent active disease despite optimal NSAID treatment and/or treatment with DMARD according to either criteria of the ASAS or the physician’s opinion. Therapy was interrupted or stopped according to the clinical rules and protocols of the department.
At the beginning of followup patients received either infliximab (5 mg/kg/infusion at Weeks 0, 2, 6, and every 8 weeks; n = 26), etanercept (50 mg/week; n = 29), or adalimumab (40 mg per 2 weeks; n = 4). Time between diagnosis and the initiation of anti-TNF therapy was 11.8 ± 9.3 years.
Thirty-eight patients received the same anti-TNF treatment during followup; 21 changed anti-TNF therapy once (n = 10), twice (n = 9), 3 (n = 1), or 4 times (n = 1). At the end of followup (mean 6.5 ± 5 yrs), 19 patients received infliximab, 27 patients etanercept, and 13 patients adalimumab. Among 59 patients, 51 had continuous anti-TNF therapy, whereas 8 patients had therapy interruption of ≥ 4 months (maximum 24 months).
Statistical analysis
Between-group comparisons were carried out using the Wilcoxon test for continuous variables and the Fisher exact test for categorical variables. Within-group relative changes (%) from baseline in lumbar spine, hip BMD (femoral neck, trochanter area, and total hip), and body weight and body composition (lean and fat mass) were stated as descriptive statistics, with comparisons from baseline values by t tests or Wilcoxon signed rank-sum tests, as appropriate. Analyses were performed to explain the variation of longterm BMD (%) using the Spearman correlation coefficient for explanatory variables assessed at baseline (ESR, CRP, lumbar spine, femoral neck and total hip T scores, body weight, lean and fat masses).
Predictor analysis for longterm BMD changes was performed in all patients and in both groups, using multivariate analysis logistic regression with inclusion of variables with p value ≤ 0.2 in univariate analysis. As longterm changes in BMD, body weight, and body composition are continuous variables, and for a better understanding for clinicians, we dichotomized the longterm changes in BMD, body weight, and body composition at the median to predict the variables “change > median (yes/no)” by logistic regression. The dependent variable was the increase in BMD [> median increase (%); yes/no] at the end of the followup at either lumbar spine or hip site. We performed 2 multivariate analyses, including only baseline variables and then including baseline and followup variables. Baseline independent variables included in the analysis were age, sex, disease duration, history of inflammatory bowel disease, steroid use, smoking, alcohol intake (≥ 2 U/day), menopausal status, current use of DMARD therapy, BASFI, BASDAI, ESR, CRP, lumbar spine, femoral neck and total hip T scores, body weight, and lean and fat masses. Followup independent variables were the CRP, ESR, BASDAI, and BASFI changes during the followup, the use of vitamin D supplementation, longterm body weight, lean and total fat mass changes, 1-year lumbar spine BMD changes, and presence of syndesmophytes at final visit. The accuracy of the multivariate models was measured by the area under the curve (AUC).
All statistical analyses were performed using SAS software, version 9.1. Statistical significance was considered at p < 0.05.
RESULTS
Baseline characteristics
Demographic, clinical, and BMD characteristics of the anti-TNF therapy group (n = 59) and control group (n = 34) are given in Table 1. The 2 groups were different for sex, disease duration, baseline disease activity (CRP, ESR, and BASDAI), and functional disease index (BASFI), with longer disease duration and higher baseline disease activity in the anti-TNF-treated group (Table 1). Three women (1 in the anti-TNF group, 2 in the control group) were menopausal.
Baseline characteristics of patients with spondyloarthritis (SpA) who have received, or not received, anti-tumor necrosis factor (TNF) during the followup period of the study.
Mean baseline T score was lower at femoral neck in the anti-TNF therapy group (−1.7 ± −1.1) than in the control group (−1.1 ± 1.0; p = 0.026) and was similar between the 2 groups at the lumbar site and at total hip, with a mean T score of −1.1 ± 1.6 and −1.1 ± 1.0 (anti-TNF therapy group), and −1.0 ± 1.4 and −0.8 ± 0.8 (control group), respectively.
Fifteen (31%) patients and 8 (24%) patients were osteoporotic in the anti-TNF therapy group and in the control group, respectively (p = 0.597). Patients with syndesmophytes at the end of the study in both groups had higher baseline lumbar BMD than patients without syndesmophytes (data not shown).
Sixteen (17.2%) patients received vitamin D during the followup in the anti-TNF therapy group and none in the control group. No patients received antiosteoporotic treatment during the followup.
BMD and body composition changes; anti-TNF therapy group (Figure 1)
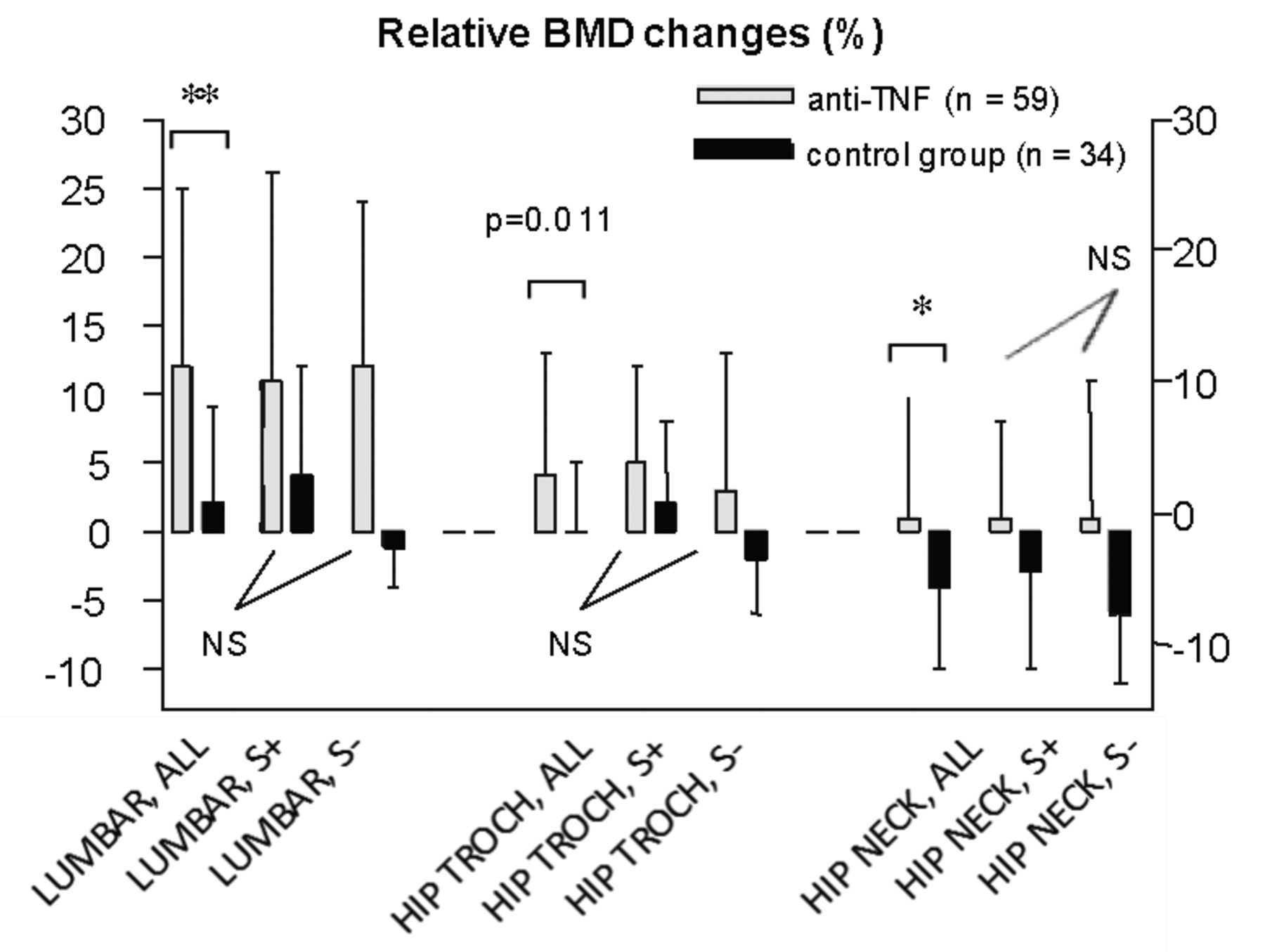
Bone mineral density (BMD) changes in the anti-TNF therapy group (mean duration of 6 years; n = 59) and the control group (mean duration of 5 years; n = 34) fail to show any influence of syndesmophytes. *p ≤ 0.001; **p ≤ 0.0001. ALL: total group; S+: subgroup with syndesmophytes; S–: subgroup without syndesmophytes; NS: not significant.
Compared to baseline, there was a significant increase in BMD at the lumbar spine, by a mean of 11.8% ± 12.8% (p < 0.0001), after a mean followup of 6.5 ± 1.6 years. The increase was also significant after the first year (5.2% ± 5.8%; p < 0.0001). Femoral neck and total hip BMD did not change significantly after 1 year and at the end of followup (+0.9% ± 6.6% and +1.1% ± 9.3%). In contrast, trochanter BMD, which reflects a trabecular bone site, increased significantly by a mean of 3.6% ± 9.3% (p = 0.0001) at the end of the followup. BMD changes between the first-year assessment and the last one were not significant.
At the end of followup, 21 (36.2%) of 58 patients had lumbar syndesmophytes. The longterm lumbar spine BMD increase was similar in patients with (11% ± 15%) and in those without (12% ± 12%) lumbar syndesmophytes. Femoral neck and total hip BMD changes were similar in patients with (+1.3% ± 7.2% and +1.9% ± 4.5%) and without (1.0% ± 10.3% and +0.3% ± 17.5%) lumbar syndesmophytes.
Longterm followup changes in lumbar spine BMD (%) were positively correlated with baseline values of CRP (r = 0.38, p = 0.004), ESR (r = 0.28, p = 0.045), and lean mass (r = 0.31, p = 0.017). Femoral neck and total hip BMD changes were not correlated with any variable (data not shown).
Compared to baseline, there was a significant increase in body weight (mean +4.5 ± 7.1 kg, i.e., 0.06% ± 0.1%; p ≤ 0.0001), in total lean mass (mean +2.6 ± 7.5 kg, i.e., 0.21% ± 1.27%; p = 0.0004), and in total fat mass (mean 2.5 ± 4.7 kg, i.e., 0.12% ± 0.3%; p = 0.0002), in these patients receiving anti-TNF therapy.
If we excluded the 8 patients that had therapy interruption ≥ 4 months, BMD and body composition changes were similar to those of the total population and changes remained significant from baseline.
BMD and body composition changes; control group (Figure 1)
Compared to baseline, mean BMD changes were not significant over 5 years at the lumbar spine (1.9% ± 7.0%) and total hip (−1.0% ± 3.4%), whereas femoral neck BMD decreased significantly over 5 years (−4.2% ± 6.3%; p = 0.0004). 1-year BMD changes were not significant at either site. BMD changes between the first year assessment and the last one were not significant except for the femoral neck (−3.1% ± 8.0%; p = 0.026).
At the end of followup, 19 (55.9%) of 34 patients had syndesmophytes. Mean lumbar spine BMD change was similar in patients with and in those without syndesmophytes. Mean BMD changes tended to be higher in patients without syndesmophytes than in patients with them, at femoral neck (−6.2% ± 5.2% vs −2.6% ± 6.9%; p = 0.063) and at total hip (−2.4% ± 2.7% vs +0.2% ± 3.5%; p = 0.051). Trochanter BMD did not significantly change over 5 years.
Compared to baseline there was a significant increase in body weight (mean +1.5 ± 3.8 kg, i.e., 0.03% ± 0.07%; p = 0.041) and in total fat mass (mean +1.3 ± 4.6 kg, i.e., 0.18% ± 0.37%; p = 0.039), but not in lean mass.
The 5-year changes in femoral neck were correlated with baseline lean mass (r = −0.38, p = 0.03); BMD changes in lumbar spine and total hip were not correlated with any variable (data not shown).
Comparisons between groups
BMD changes (%) were significantly higher in the anti-TNF therapy group than in the control group at lumbar spine (p < 0.0001), femoral neck (p = 0.002), and trochanter (p = 0.011), but not at total hip (p = 0.062). At the end of the followup, the numbers of osteoporotic patients did not change significantly in the anti-TNF therapy group (31 to 25; p = 0.132) and in the control group (24 to 21; p = 0.564). Five vertebral fractures (T12, n = 4; L1, n = 1) diagnosed by VFA at the final visit, 2 cervical fractures, and 2 nonvertebral fractures (wrist, n = 1; hip, n = 1) were observed during followup in the anti-TNF therapy group. Data on incident fractures in the control group were not available. Increase in lean mass was significantly higher in the anti-TNF group than in the control group (0.21 ± 1.27 kg vs −0.01 ± 0.05 kg; p = 0.0004). Changes of body weight and total fat mass were not significant between the 2 groups.
Predictors of changes of BMD. All patients
Multivariate analysis (logistic regression) showed that the increase in lumbar spine BMD [> median increase (%); yes/no] at the end of followup was significantly explained by baseline lumbar spine T score (OR 0.50, 95% CI 0.32–0.79, p = 0.003), lean mass per 100 grams (OR 1.01, 95% CI 1.00–1.02, p = 0.030), and use of anti-TNF therapy (OR 23.95, 95% CI 4.82–118.99, p = 0.0001) with an AUC of 0.886. After inclusion of the followup variables, the predictors were baseline femoral neck T score (OR 0.43, 95% CI 0.19–0.98, p = 0.044), use of DMARD (OR 13.25, 95% CI 1.50–116.81, p = 0.02), use of vitamin D during the followup (OR 8.17, 95% CI 1.52–43.91, p = 0.014), and the 1-year lumbar spine BMD changes (OR 1.38, 95% CI 1.19–1.67, p = 0.001), with AUC = 0.916.
The trochanter BMD increase [> median increase (%); yes/no] observed at the end of followup was explained only by the use of anti-TNF therapy (OR 3.11, 95% CI 1.16–8.32, p = 0.024; AUC = 0.628). After inclusion of the followup variables, the only predictor was the baseline ESR value (OR 1.0, 95% CI 1.02–1.11, p = 0.007; AUC = 0.739).
Predictors of changes of BMD. Anti-TNF therapy group
Multivariate analysis (by logistic regression) showed that the increase in lumbar spine BMD [> median (%) increase; yes/no] at the end of the followup was significantly explained by baseline lumbar spine T score (OR 0.42, 95% CI 0.25–0.70, p = 0.01) and lean mass per 100 units (OR 1.01, 95% CI 1.00–1.02, p = 0.026), with AUC = 0.850. After inclusion of the followup variables, the only predictor was the 1-year lumbar spine BMD change (OR 1.40, 95% CI 1.15–1.88, p = 0.007; AUC = 0.921).
The increase in trochanter BMD [> median increase (%); yes/no] observed at the end of the followup was explained by the presence of inflammatory bowel disease (OR 0.10, 95% CI 0.01–0.93, p = 0.043) and the BASDAI (OR 0.95, 95% CI 0.92–0.99, p = 0.020), with AUC = 0.760.
Predictors of changes of BMD. Control group
Multivariate analysis did not reveal any variable associated with 5-year changes of lumbar spine BMD. The trochanter (%) BMD increase [> median BMD increase (%); yes/no] observed at the end of followup was explained only by disease duration (OR 0.80, 95% CI 0.65–0.99, p = 0.038; AUC = 0.745).
DISCUSSION
Our study showed that prolonged anti-TNF therapy over a mean of 6.5 years improves lumbar spine BMD in patients with SpA by 12%. An increase in BMD in patients with SpA receiving anti-TNF therapy was reported over 6 months17 and over 2 years16,18, and our study extends these observations.
Increase in BMD was observed at the lumbar spine and not at the hip or femoral neck. This could be an artefact related to spinal ossifications and syndesmophytes, because 36% of our population had syndesmophytes at the final visit. However, BMD changes were similar in patients with and without syndesmophytes, and we observed a significant increase in trochanter BMD, a bone of mainly trabecular histology, suggesting a systemic effect of anti-TNF on BMD. Baseline femoral neck BMD was lower in the anti-TNF therapy group than in the control group and did not change significantly in the anti-TNF therapy group, whereas femoral neck BMD decreased in the control group. The lower baseline femoral neck BMD of the anti-TNF group can be explained by the higher level of activity and inflammation of this group, and the efficacy of anti-TNF on disease activity may explain the absence of femoral neck bone loss. A 1-year study in early SpA showed that BMD loss was preferential at hip and was related to disease activity24.
BMD changes can be explained by the antiresorptive effect of anti-TNF therapy. Previous studies showed an increase in bone resorption (reflected by elevated bone resorption markers) related to bone loss in AS11,25. We previously reported that anti-TNF therapy induces an early and sustained decrease in the serum CTX-1 bone resorption marker (−50% at 3 months and −30% at 1 year), illustrating the anti-osteoclastic effect of anti-TNF therapy26, which is expected because TNF-α stimulates osteoclastogenesis via the osteoprotegerin/receptor activator for nuclear factor-κB ligand pathway27. The increase in BMD might also be related to a positive effect of anti-TNF therapy on bone formation. Indeed, TNF-α decreases osteoblastic activity through inhibition of both Wnt and BMP pathways28. Recent data suggest that TNF-α affects the differentiation of mesenchymal precursor cells into osteoblasts, by downregulating RUNX2 expression29. Thus, anti-TNF may improve osteoblastic activity and osteoblast formation, leading to an increase in systemic bone formation with an increase in BMD30. One study in patients with AS treated with infliximab showed that high baseline osteocalcin levels and early increases in bone alkaline phosphatase, markers of bone formation, were associated with increases in BMD16. However, in our study, the early and high lumbar spine BMD increase observed after the first year (5.2%) may be related more to a pure antiresorptive effect rather than an increase in bone formation.
Loss of lean mass in the context of chronic inflammation has been described in established AS31, as well as the beneficial effect of anti-TNF over 2 years on total body weight and body composition18. We confirm in a longterm followup a significant increase in body weight in patients with SpA treated with longterm anti-TNF, related to an increase in both lean and fat masses.
The change in lean mass was not significant in the control group; in the treated group, it can be explained by a specific effect of anti-TNF-α therapy or by the effect of inflammation control by anti-TNF-α therapy, or both. In our study, lean mass was a determinant of the lumbar spine BMD changes in all patients and in the anti-TNF therapy group as well. We could not determine how this change in muscle mass might determine part of the change of BMD, that is, either directly or through the improvement of physical activity. Use of vitamin D during followup, revealed in the multivariate analysis, influenced the changes in lumbar spine BMD in the anti-TNF therapy group and not in the control group. However, in the absence of data concerning the dose, treatment duration, and serum level of 25-OH-D, the role of vitamin D should be interpreted carefully. Gut involvement could also contribute to bone loss in SpA in our study; the presence of inflammatory bowel disease was a determinant of BMD changes at the trochanteric site in the anti-TNF therapy group.
An observation relevant for clinical practice was that longterm lumbar spine BMD changes in patients treated with anti-TNF therapy are driven mainly by baseline BMD and 1-year lumbar spine BMD changes. Indeed, the results suggest that in patients with SpA with low bone mass treated with anti-TNF therapy, the indication for an antiosteoporotic treatment, such as a bisphosphonate, should be discussed only after assessment of the bone effect of anti-TNF therapy at 1 year.
Our study had the longest duration of followup of BMD changes in anti-TNF-treated patients with SpA; its strengths are the comparison to a control group followed in a longitudinal observational study, and the assessment of syndesmophytes at final visit, necessary for the interpretation of these longterm changes. The main limitation was that the study design was not placebo-controlled, and we used a historical group of patients as controls. However, a placebo-controlled study is not possible for ethical reasons in patients requiring anti-TNF therapy. Moreover, the use of a historical group allowed assessment of changes in patients with various degrees of disease activity. Another limitation is that the influence of structural changes (syndesmophytes) on changes in BMD measurements during followup could not be completely excluded because posterior plane ankylosis (zygapophyseal joint) cannot be assessed with available imaging. Indeed, patients with AS can have more zygapophyseal joint ankylosis without anterior plane bridging syndesmophytes32, and these might contribute to a higher BMD assessed by DEXA. The use of 2 different methods for syndesmophyte assessment is also a limitation: VFA has not been evaluated for this purpose and we cannot exclude that VFA might be less sensitive than the mSASS score measured on standard radiographs to detect syndesmophytes because the techniques have never been compared. Differences in BMD changes between anti-TNF-treated SpA patients and the control group could be explained by therapy with NSAID, which may decrease bone formation, and this could explain the lower BMD changes in the control group. At the end of followup, 7 patients in the anti-TNF group and 22 in the control group used NSAID daily, but we have no information on NSAID use during followup. The remaining limitation was the multiple testing analyses precluding any definite conclusion for some correlations with borderline statistical significance.
Our study suggests that prolonged anti-TNF therapy has beneficial effects on BMD and body composition in patients with SpA. In such patients with anti-TNF therapy and low BMD, it seems logical to assess the benefit of this treatment before introducing antiosteoporotic treatment. Whether this is the effect of optimal control of inflammation or a direct effect of anti-TNF on regulation of bone formation pathways must be the subject of further studies.
Acknowledgment
We thank Laure Gossec for her support in the conception of the project.
Footnotes
-
Dr. Durnez was supported by a EULAR grant, the Belgian Fund for Scientific Research in Rheumatology (FWRO/FRSR), and a European Calcified Tissue Society grant (ECTS); and has received fees and/or honoraria from Abbott, MSD, and Pfizer. Dr. Dougados has received consultancies, fees, and/or honoraria from Pfizer, Abbott, UCB, and Roche. Dr. Roux has received consultancies, fees, and/or honoraria from Amgen, MSD, Roche, Novartis, Servier, Lilly, and Pfizer. Dr. Briot has received consultancies, fees, and/or honoraria from Amgen, MSD, Novartis, and Lilly.
- Accepted for publication June 11, 2013.








{kind=link}