

To the Editor:
Systemic fluoroquinolones have been known to cause tendinopathy. Since 2008, the US Food and Drug Administration has required a “black-box” warning on all systemic fluoroquinolones because of the risk of tendinopathy and tendon rupture1. Fluoroquinolone-associated tendinopathy symptoms have been documented from as early as 2 hours after the initial exposure to as late as 6 months after discontinuation of therapy2. However, in contrast to systemic fluoroquinolones, no reported cases of tendinopathy have been associated with the use of ophthalmic fluoroquinolones. Further, there is no black-box label for this formulation. We describe a case of tendinopathy following topical ophthalmic fluoroquinolone treatment.
A 56-year-old man with a history of hypothyroidism and cataracts underwent cataract surgery and was administered daily moxifloxacin ophthalmic drops. On day 14 of therapy, he noted severe pain in his left knee followed by similar pain in his left Achilles tendon. Four days after the pain started, moxifloxacin was discontinued. A couple of days later, he developed right knee and right Achilles tendon pain. He indicated that he had received a steroid injection for a herniated disc at least 2 months prior to the cataract surgery. He also reported a history of short prednisone courses for bronchitis, with the most recent course 1 year prior to treatment with moxifloxacin ophthalmic drops. His only active medication was levothyroxine. He denied any exposure to tobacco, alcohol, or recreational drugs. There was no history of recent infection, psoriasis, uveitis, or other manifestations that would suggest a seronegative spondyloarthropathy. The physical examination was unremarkable, except for tenderness to palpation over bilateral Achilles tendons, right > left 2 cm from distal insertion proximally 5 cm, with negative Thompson test and minimal tendon swelling, as well as pain with plantar and dorsiflexion of the ankles. Bilateral knees showed no effusion and had minimal patellar tendon tenderness.
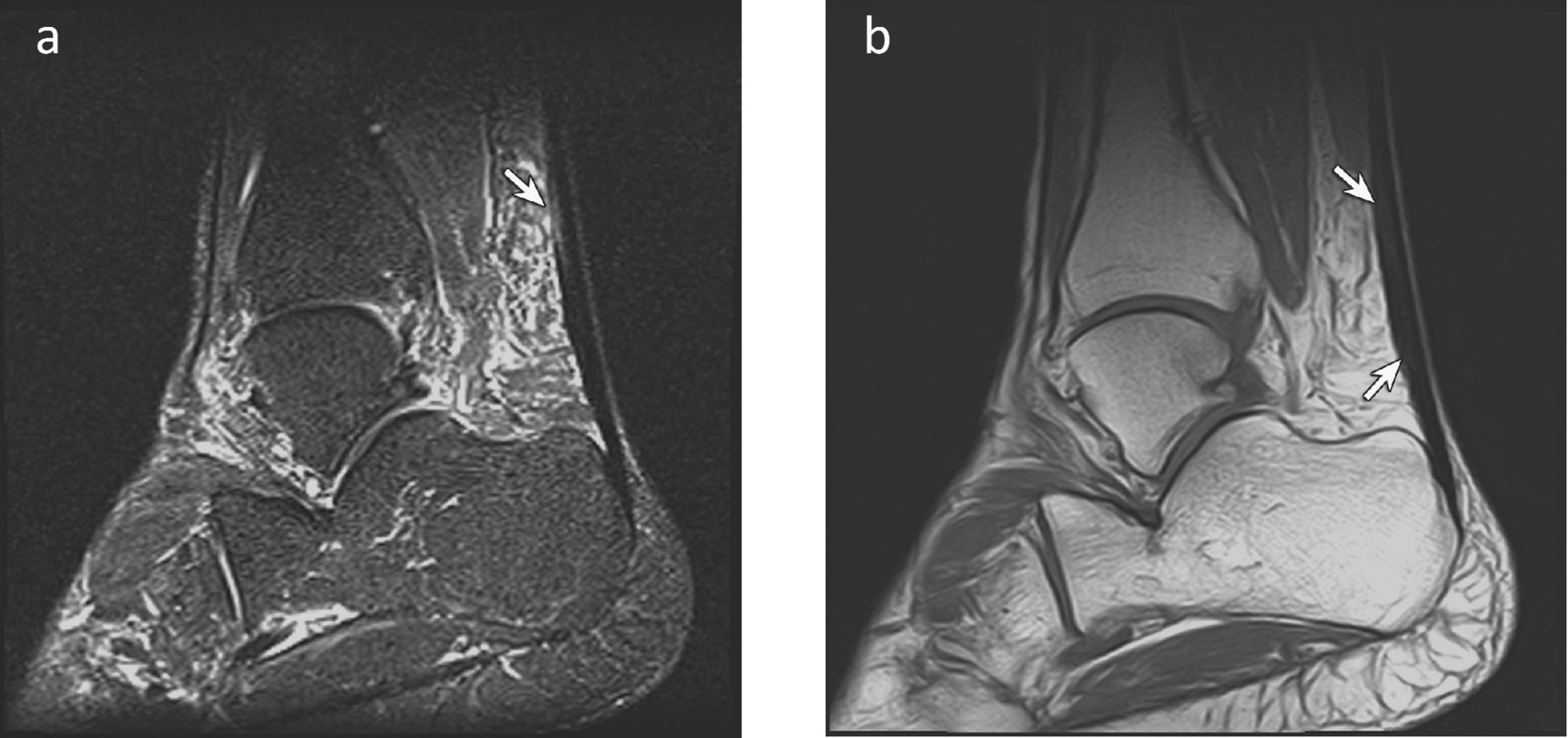
He was evaluated by his primary care physician, who performed magnetic resonance imaging (Figure 1) confirming tendinopathy, and recommended 3 months of rest and the use of an immobilizing walking boot. The pain did not improve with this regimen and physical therapy ensued for a few months with no relief. He was then referred to a rheumatologist 6 months later for evaluation of his persistent symptoms. A trial of nonsteroidal antiinflammatory drugs was unsuccessful, and a trial of low-dose oral steroids caused increased pain.

T1-weighted (a) and fluid-sensitive (b) sagittal magnetic resonance images of the Achilles tendon show increased signal (arrows) within the Achilles tendon. Note edema anterior to Achilles tendon within Kager fat pad.
It is unclear how fluoroquinolones induce tendinopathy. On histologic examination, fluoroquinolone-associated tendinopathy is similar to that observed following athletic overuse injury and is characterized by abnormal fiber structure, hypercellularity, fibrotic areas, increased extra-cellular matrix, and neovascularization3,4. Proposed mechanisms include direct effects of fluoroquinolones on fibroblasts5, induction of increased matrix metalloproteinase-3 expression6, and oxidative stress7. Treatment options remain limited. Some suggest that coadministration of coenzyme Q10, magnesium, or antioxidants may help decrease the incidence of tendinopathy with systemic fluoroquinolones4.
To our knowledge, there have been no reported cases of tendinopathy induced by ophthalmic fluoroquinolones, and this complication is not listed as a side effect on the label, likely because of the low peak plasma concentrations of the drug following ophthalmic administration. However, a study in horses showed significant serum levels of moxifloxacin after topical administration of ophthalmic moxifloxacin, as compared to ophthalmic ciprofloxacin, which resulted in undetectable levels in the serum8. Risk factors associated with systemic fluoroquinolone-induced tendon disorders include age > 60 years, history of corticosteroid therapy, renal failure, diabetes mellitus, and a history of musculoskeletal disorders9. This patient’s previous use of corticosteroids may have increased the risk for tendinopathy. This case suggests that incapacitating tendinopathy may develop with ophthalmic fluoroquinolones in predisposed individuals. It is important to be aware of this possibility when prescribing ophthalmic fluoroquinolones.








{kind=link}