

Article Figures & Data
Figures
- Figure 1.
Normal magnetic resonance imaging of the temporomandibular joint (TMJ). Coronal (A) and sagittal (B) postcontrast T1-weighted fat-saturated images of the TMJ. The condylar heads (labeled C) are well situated in their respective fossae.
- Figure 2.
Active temporomandibular joint synovitis. Sagittal T2-weighted fat-saturated (FS) precontrast (A) and T1-weighted postcontrast FS (B) images show synovial fluid (A, arrows) and enhancement (B, large arrows). Erosive changes at the condylar head are also evident on B (small arrows).
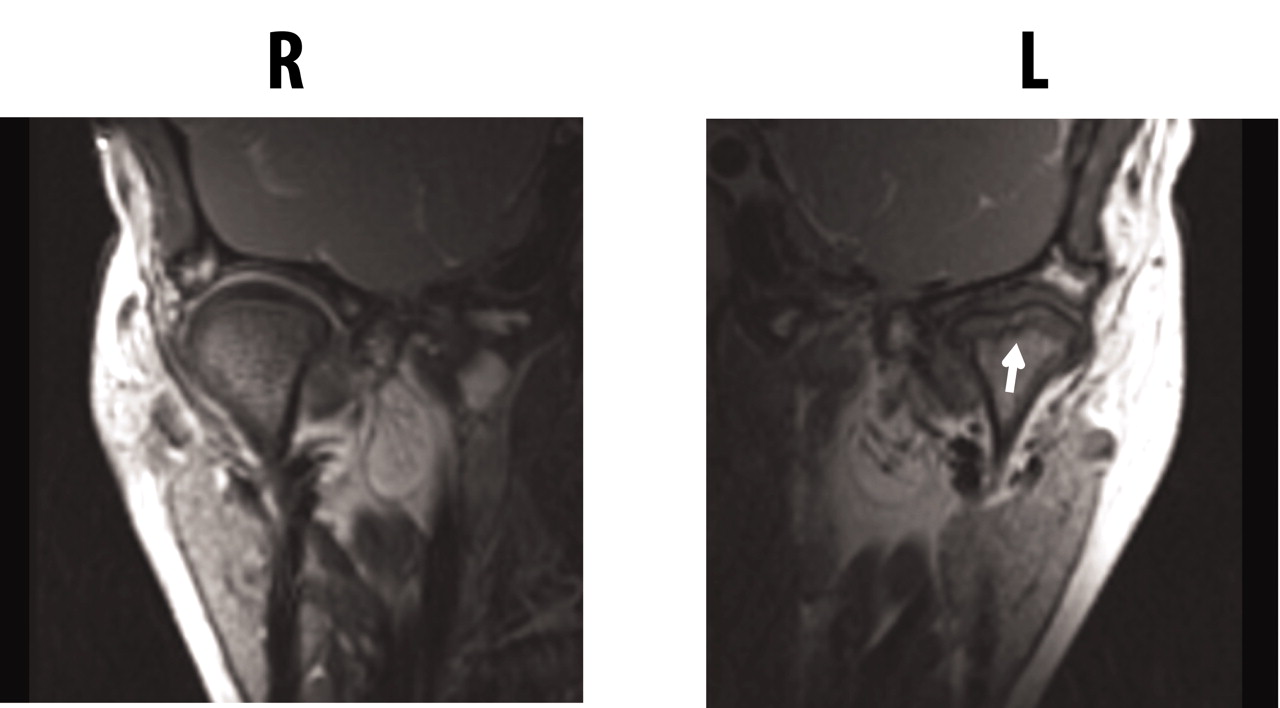
- Figure 3.
Destructive changes of the temporomandibular joint (TMJ). Coronal T1-weighted image of the TMJ shows flattening and erosive changes of the left condylar head (arrow); the right TMJ is normal.
- Figure 4.
Percentage of patients with abnormal MRI of the TMJ, by JIA subtype. Current results are compared with those published by Cannizzaro, et al16. Oligo: oligoarticular JIA; poly: polyarticular JIA.
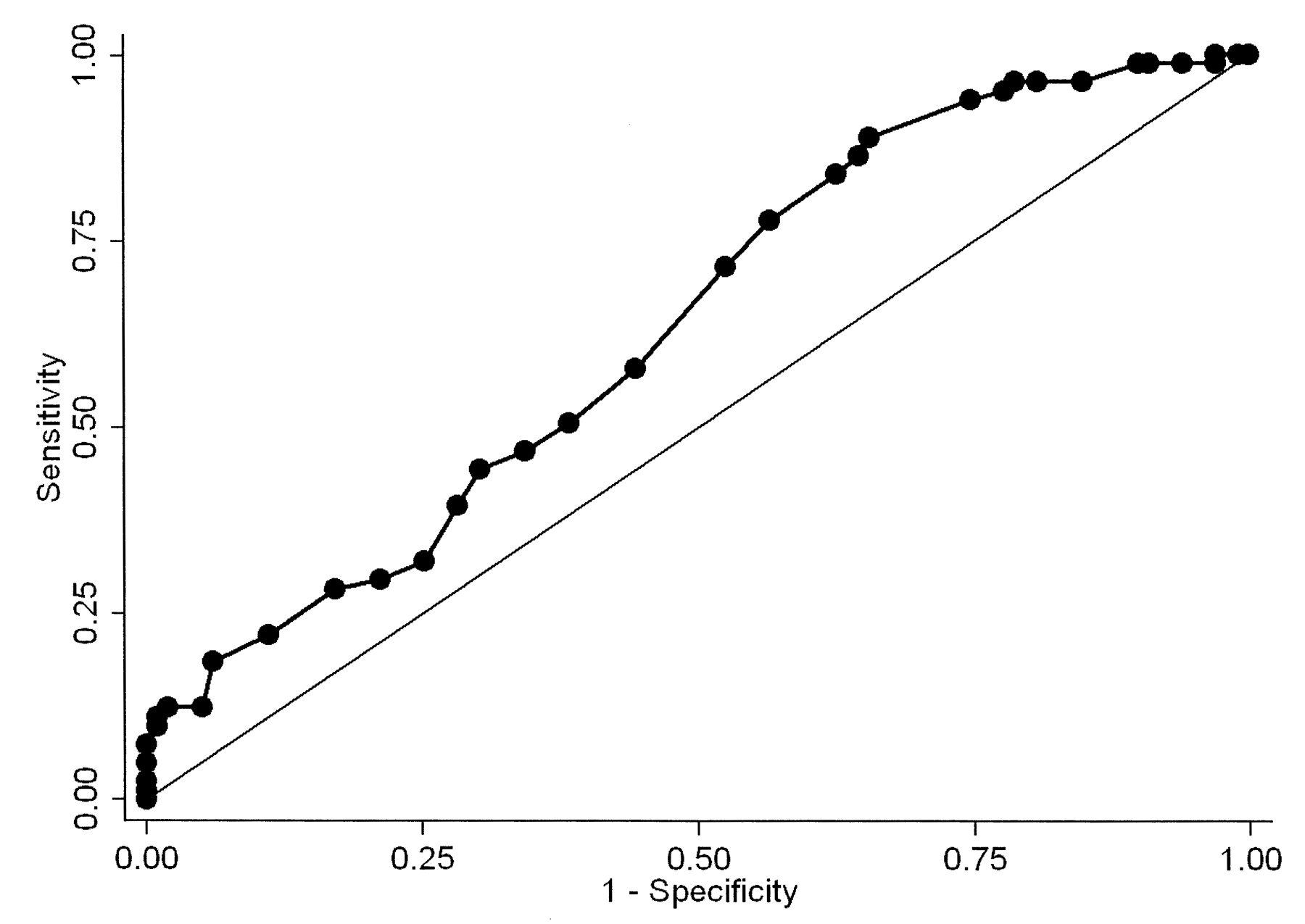
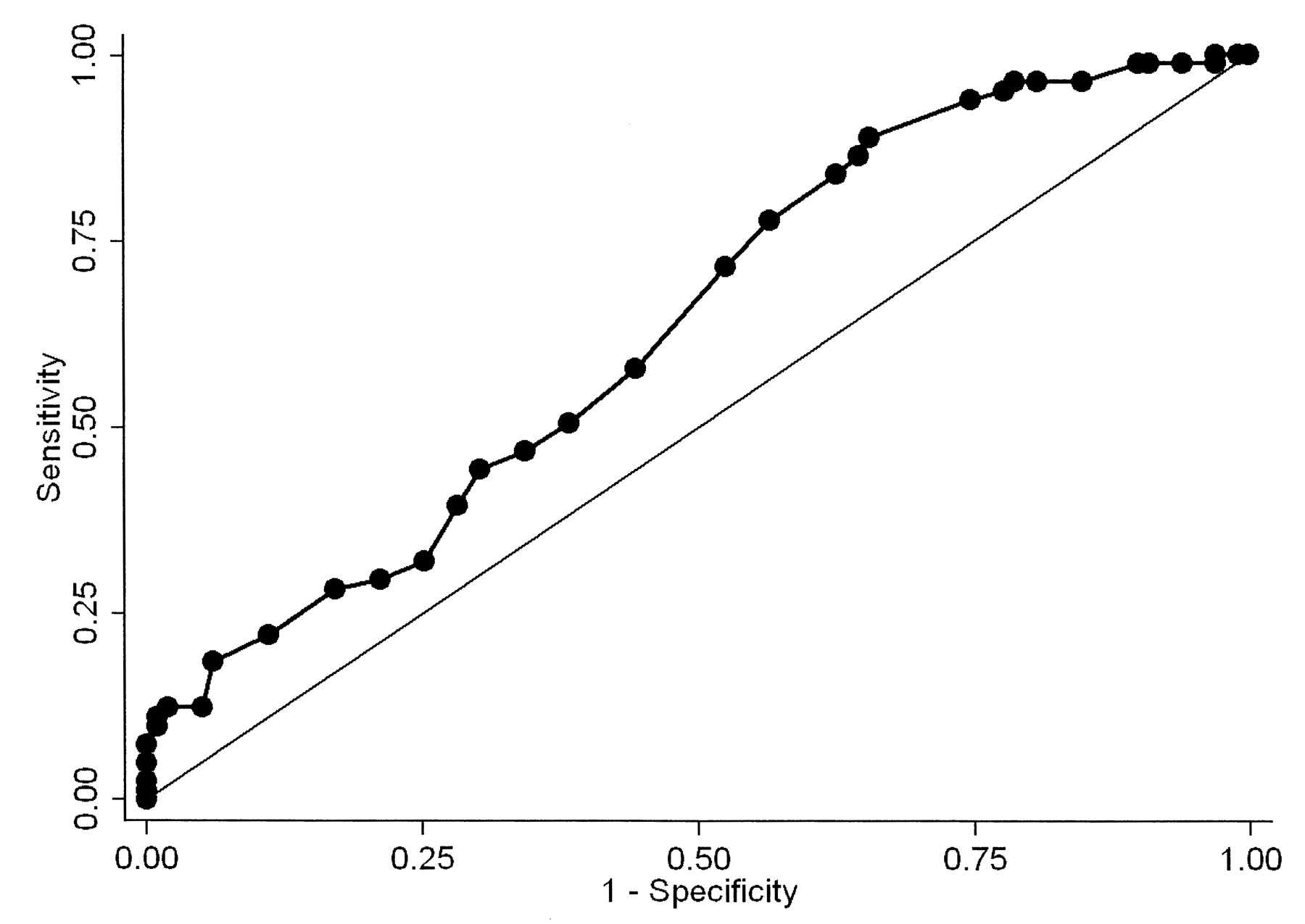
- Figure 5.
Receiver-operator curve analysis for the ability of maximal incisal opening to predict TMJ arthritis.




Tables
- Table 1.
Patient population. Statistically significant differences (p < 0.05) are depicted in bold type.
Feature Entire Group, n = 187 TMJ Arthritis-negative, n = 106 TMJ Arthritis-positive, n = 81 p Demographics Age at diagnosis, yrs; mean, SEM, range 6.7, 0.31, 1–15 6.0, 0.40, 1–15 7.6, 0.46, 1–15 0.006 Disease duration*, yrs; mean, SEM, range 2.5, 0.3, 0–17 3.1, 0.38, 0–14 1.6, 0.31, 0–17 0.005 Newly diagnosed (< 3 mo) 56, 30 28, 26 28, 35 0.228 Age at study, yrs; mean, SEM, range 9.1, 0.34, 1.7–21 9.1, 0.50, 1.7–2.1 9.2, 0.45, 2–18 0.794 Female, n, % 116, 62 63, 59 53, 65 0.402 Race, n (%) 0.981 White 162, 87 92, 87 70, 86 African-American 23, 12 13, 12 10, 12 Other 2, 1.0 1, 0.9 1, 1.2 JIA subtype, n, % 0.251 Oligoarticular JIA 56, 30 31, 29 25, 31 RF– polyarticular JIA 35, 19 18, 17 17, 21 RF+ polyarticular JIA 3, 1.6 1, 0.9 2, 2.5 Psoriatic JIA 37, 20 23, 22 14, 17 Enthesitis-related arthritis 40, 21 25, 24 15, 18 Systemic-onset JIA 12, 6.4 8, 7.5 4, 4.9 Undifferentiated 4, 2.1 0 4, 4.9 Laboratory studies Positive ANA 39/164, 24 23/92, 25 16/72, 22 0.678 Positive RF 6/118, 5.1 3/63, 4.8 3/55, 5.5 1.000 ACPA 4/50, 8.0 1/23, 4.3 3/27, 11 0.617 Positive HLA-B27 17/104, 16 11/54, 20 6/50, 12 0.249 Medications, n, % NSAID 125, 67 77, 73 48, 59 0.054 MTX 110, 59 68, 64 42, 52 0.090 Sulfasalazine 2, 1.1 0 2, 2.5 0.186 Leflunomide 2, 1.1 2, 1.9 0 0.506 Any anti-TNF 84, 45 50, 47 34, 42 0.479 Anakinra 9, 4.8 5, 4.7 4, 4.9 1.000 Combination DMARD 80, 43 49, 46 31, 38 0.276 MTX and anti-TNF 70, 37 42, 40 28, 35 0.479 MTX and anakinra 8, 4.3 5, 4.7 3, 3.7 1.000 Any DMARD 126, 67 76, 72 50, 62 0.150 Oral corticosteroids 32, 17 19, 18 13, 16 Physical examination, n, % Mouth opening deviation 53, 28 13, 12 40, 49 < 0.001 MIO, mm; mean, SEM, range Age 0–7.9 41.3, 0.74, 23–54 43.1, 0.86, 34–54 38.9, 1.2, 23–49 0.004 Age 8+ 45.8, 0.77, 30–65 47.8, 1.1, 31–65 43.6, 0.97, 30–62 0.005 Low MIO for age** 48, 27 21/99, 21 27/81, 33 0.067 Mouth opening deviation or low MIO 81, 43 30, 28 51, 63 < 0.001 Overall joint count†; mean, SEM, range 2.2, 0.32, 0–34 2.0, 0.31, 0–16 2.6, 0.61, 0–34 0.358 Joint count 0† 73, 39 37, 35 36, 44 0.185 Joint count 1 or lower† 115, 62 63, 59 52, 64 0.507 Joint count 4 or lower† 165, 88 94, 89 71, 88 0.829 -
↵* Elapsed time between diagnosis of JIA and the initial MRI.
-
↵** Defined as < 2 SD below norm for age20.
-
↵† Total joint count is exclusive of the TMJ itself. TMJ: temporomandibular joint; ANA: antinuclear antibody; ACPA: anticitrullinated protein antibodies; DMARD: disease-modifying antirheumatic drug (includes methotrexate, sulfasalazine, leflunomide, and biologic); JIA: juvenile idiopathic arthritis; MIO: maximal incisal opening; MTX: methotrexate; NSAID: nonsteroidal antiinflammatory drugs; RF: rheumatoid factor; TNF: tumor necrosis factor.
-
- Table 2.
MRI findings of TMJ arthritis. Data are limited to patients with contrast-enhanced MRI (n = 185).
Finding n Percentage of Total Percentage of Abnormal By individual TMJ 370 NA NA Active or chronic arthritis 142 38 NA Active arthritis, any 135 36 95 Synovial fluid alone 19 5.1 14 Enhancement alone 85 23 63 Synovial fluid and enhancement 31 8.4 23 Chronic arthritis, any 26 7.0 18 Erosions alone 12 3.2 46 Condylar flattening alone 12 3.2 46 Combination of findings of chronic arthritis 2 0.5 7.6 Acute arthritis without chronic changes 115 31 81 Chronic arthritis without acute changes 6 1.6 4.2 Acute and chronic changes 20 5.4 14 By individual patient 185 NA NA Any abnormality 81 43 NA Active arthritis without chronic changes 59 32 73 Chronic arthritis without acute changes 2 1.1 2.4 Active and chronic changes 20 11 24 -
MRI: magnetic resonance imaging; TMJ: temporomandibular joint. NA: not applicable.
-
Factor Univariate OR Multivariable OR Mouth opening deviation 6.98 (3.38–14.4) 6.21 (2.87–13.4) Maximal incisal opening 0.93 (0.89–0.97) 0.94 (0.90–0.99) Age at diagnosis 1.10 (1.03–1.19) NS Disease duration 0.87 (0.79–0.96) 0.87 (0.78–0.97) -
TMJ: temporomandibular joint; NS: not significant.
-








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}