

Abstract
Objective. Black Africans currently experience a distinctly low frequency of atherosclerotic cardiovascular disease. Whether this protection persists in those with rheumatoid arthritis (RA) is unknown. We compared the carotid atherosclerosis burden and its relationships with cardiovascular (CV) risk factors between Africans with RA from a developing black and developed CV population.
Methods. We performed high resolution B-mode ultrasonography and assessed CV risk factors in 243 patients with established RA, of whom 121 were black and 122 white. Data were analyzed in age, sex, and healthcare center-adjusted regression models.
Results. The mean ± SD common carotid intima-media thickness (cIMT) was 0.694 ± 0.097 mm in black and 0.712 ± 0.136 mm in white patients (adjusted p = 0.8). Plaque prevalence was also similar in black compared to white cases (35.5% and 44.3%, respectively; adjusted OR 0.83, 95% CI 0.32–2.20, p = 0.7). Interactions between population grouping and several CV risk factors were independently associated with cIMT and plaque. In stratified analysis, that is, in each population group separately, risk factors associated with cIMT or/and plaque comprised the systolic blood pressure (p = 0.02), serum cholesterol/high-density lipoprotein cholesterol ratio (p = 0.004), C-reactive protein concentrations (p = 0.01), and the presence of extraarticular manifestations (p = 0.01) in whites but, contrastingly, the Arthritis Impact Measurement Scales tension score (p = 0.04) and use of nonsteroidal antiinflammatory agent (p = 0.03) in black patients. The Framingham score was significantly associated with atherosclerosis only in whites (p < 0.0001).
Conclusion. The carotid atherosclerosis burden is similar in black compared to white Africans with RA, but relationships between modifiable CV risk factors and atherosclerosis vary substantially among Africans with RA.
Rheumatoid arthritis (RA) is a chronic inflammatory and destructive joint disease that is recognized to enhance the risk for atherosclerotic cardiovascular disease (CVD) events about 2-fold1. The standardized CV mortality ratio is increased by 50% in RA and thereby accounts for most of the excess overall mortality caused by this disease2.
CVD in RA is brought about by traditional and nontraditional CV risk factors or disease characteristics, particularly inflammation3,4,5,6,7,8,9,10. Importantly also in this context, whereas genetic factors contribute substantially to CVD in the population at large11, the same likely applies in RA. Indeed, genetic polymorphisms that are implicated in inflammatory pathways such as the TNFA-308 (rs1800629)12 and the CCR5Δ32 variant13 and metabolic pathways including the acid phosphatase locus 1*C allele14 were recently shown to be associated with CVD in patients with RA. Further, genes that influence RA susceptibility can influence CVD15 and its conventional risk factors in RA16. These findings may enable elucidation of the molecular mechanisms involved, discovery of new therapeutic targets, and optimization of risk assessment in RA-related CVD.
Our knowledge of CVD in the general population and even more in persons with chronic inflammatory diseases such as RA largely derives from studies that were performed in developed populations17,18. However, ∼80% of CVD now arises in middle and low-income groups or in developing countries17. Further, the effect of individual CV risk factors on CV events may differ in the developing compared to the developed nations18,19,20.
South Africa, a sub-Saharan country with 50 million inhabitants, has become the most unequal society in the world21. A minority of South Africans follow a westernized lifestyle, live in modern cities, and represent a developed and mostly white population, whereas the majority still follow a more traditional lifestyle, live outside these cities, and typify a developing and predominantly black population20,22,23. Accordingly, these populations are at different stages of the epidemiological health transition, and the incidence of CVD is still distinctly uncommon in black compared to white sub-Saharan Africans18,20,22. However, whether this protection is present in black Africans in the face of established RA is unknown. The South African Heart Association recommends the European Society of Cardiology and European Atherosclerosis Society guidelines on CV risk assessment and management irrespective of population grouping or socioeconomic factors24. In keeping with an earlier epidemiological transition stage, we recently identified several disparities in individual CVD risk factor profiles between blacks and other Africans with RA (whites, Asians, and people of mixed ancestry) but the overall traditional and nontraditional CVD risk burden was similar in both populations18. In our present study, we compared the ultrasonographically determined carotid atherosclerosis burden, a predictor of CVD events in the general population and in patients with RA24,25,26, in black and white Africans with RA. Additionally, we investigated whether disparities exist in the relationships of modifiable CVD risk factors with carotid atherosclerosis between the 2 populations.
MATERIALS AND METHODS
Study populations
We enrolled patients during the period March 23 to November 25, 2009, who met the American College of Rheumatology criteria for RA27, at the Charlotte Maxeke Johannesburg Academic Hospital (public healthcare) and Milpark Hospital (private healthcare) in Johannesburg (Table 1). None of the recorded data have been reported previously. Only patients that had used disease-modifying agents were included; 4 invited patients refused to participate and those known to be infected with the human immunodeficiency virus (HIV) were excluded. Considering the aims of the investigation, we also excluded patients of mixed ancestry and Asians with RA because they are not consistently at the same epidemiological transition stage as either black or white Africans20. The HIV prevalence in South Africans aged 50 years and older is currently 5.7%28; and Asians and people of mixed ancestry comprise 11% and 8%, and 8% and 5% of patients with RA in our public and private healthcare centers, respectively18.
African patients (n = 243) with RA by sex and healthcare center.
Whereas patients attending South African public healthcare centers currently have no access to use of biological agents for RA, this intervention was employed in 10 private-care patients (tumor necrosis factor-α blockade in 9 and rituximab in 1), all whites. Biological and nonbiological disease-modifying antirheumatic drugs (DMARD) were grouped into the same single variable for the purpose of our data analysis. Nonsteroidal antiinflammatory drugs (NSAID) used in black and white patients comprised nonselective cyclooxygenase (COX) inhibitors (indomethacin and ibuprofen) in the former and both traditional NSAID (ibuprofen, diclofenac, and meloxicam) and selective COX-2 inhibitors (celecoxib and etoricoxib) in the latter.
The study was approved by the Ethics Committee for Research on Human Subjects (Medical) of the University of the Witwatersrand. Written informed consent was obtained from each patient.
Assessments
CV risk factors that were assessed are presented in Table 2. Data were missing in < 5% for any of the recorded characteristics. All patients fasted for at least 8 h prior to blood sampling. Hypertension was defined as average systolic blood pressure ≥ 140 mm Hg or/and diastolic blood pressure ≥ 90 mm Hg or/and current use of antihypertensive medications. Serum total cholesterol and low and high-density lipoprotein (LDL, HDL) concentrations were determined by enzymatic assays, serum triglyceride concentrations by the glycerol phosphate oxidase method, and C-reactive protein (CRP) concentrations by nephelometry. Dyslipidemia was diagnosed when the atherogenic index, i.e., cholesterol/HDL cholesterol ratio, was > 4, and the proatherogenic non-HDL concentrations were calculated by subtracting HDL cholesterol from total cholesterol concentrations18,29,30. Current smoking status was assessed. Diabetes was defined as plasma glucose concentration ≥ 7 mmol/l or/and use of glucose-lowering agents. We recorded alcohol use (at least 1 unit per month), exercise (at least once per month and including time spent in walking, that is, to reach public transport), marital status, education level (years of education), body mass index (BMI), waist circumference, and the waist-hip ratio. Symptoms of tension and depression were estimated by the Arthritis Impact Measurement Scales (AIMS)31.
Cardiovascular risk factor profiles in black compared to white patients with RA. Dichotomous variables are expressed as proportions or percentages and continuous characteristics as mean ± SD. Significant associations are shown in bold type.
RA characteristics evaluated as potential CV risk factors comprised the rheumatoid factor status, extraarticular manifestations (see below), use of antirheumatic agents including NSAID, prednisone, and number of prescribed DMARD, RA duration, the Disease Activity Score in 28 joints (DAS28), serum CRP concentrations, the Stanford Health Assessment Questionnaire Disability Index, and the number of deformed joints18,32. Extraarticular manifestations included current or previously recorded (hospital record review) presence of pericarditis, pleuritis, Felty’s syndrome, cutaneous vasculitis, neuropathy, scleritis or episcleritis, retinal vasculitis, glomerulonephritis, vasculitis affecting other organs, amyloidosis, keratoconjunctivitis sicca, xerostomia, Sjögren’s syndrome, pulmonary fibrosis, bronchiolitis obliterans organizing pneumonia, cervical myelopathy, and subcutaneous nodules and rheumatoid nodules in other locations32,33.
Two authors (BAS, AS) performed the carotid artery ultrasound measurements in private and public healthcare patients, respectively. Both operators obtained images of at least 1-cm length of the distal common carotid arteries for measurement of the intima-media thickness of the far wall from an optimal angle of incidence, defined as the longitudinal angle of approach where both branches of the internal and external carotid artery are visualized simultaneously34. They used high-resolution B-mode ultrasound (Image Point, Hewlett Packard, Andover, MA, USA, and SonoCalc IMT, Sonosite Inc., Bothell, WA, USA; used by BAS and AS, respectively) with linear array 7.5-MHz probes. Details of the methodology used by BAS were as reported3. The equipment used by AS involved application of a unique semiautomated border detection program that was found to provide highly reproducible results34. The intima-media thicknesses in the left and right common carotid artery were measured; carotid intima-media thickness (cIMT) was defined as the mean of these. Carotid artery plaque was defined as a focal structure that encroaches into the arterial lumen by at least 0.5 mm or 50% of the surrounding intima-media thickness value, or demonstrates a thickness of > 1.5 mm as measured from the media-adventitia interface to the intima-lumen interface35. Both operators were blinded to the CV risk profiles of the patients. Repeat ultrasound examinations by both operators on 23 patients revealed Spearman correlations between repeat cIMT measurements of 0.983 for BAS and 0.956 for AS, and the correlation between measurements made by BAS and AS was 0.926. Both operators identified carotid artery bulb or/and internal carotid artery plaque in 11 of these 23 patients with full agreement.
Statistical methods
We grouped the CV risk factors into 3 categories18 (Table 2): (1) the major modifiable conventional risk factors of hypertension, dyslipidemia, smoking, and diabetes that feature in the Framingham score; (2) other CV conventional risk or predisposing factors including alcohol use, exercise, marital status, education level, BMI, waist circumference, waist-hip ratio, serum triglyceride concentrations, and the AIMS tension and depression scores; and (3) nonconventional risk factors consisting of RA characteristics.
Dichotomous variables are expressed as proportions or percentages and continuous variables as mean ± SD. Non-normally distributed characteristics were logarithmically transformed prior to statistical analysis and for these variables geometric means ± SD are given. The selection of potential confounders in multivariate regression models was based on biological plausibility.
Relationships between population grouping, or in the present context, also ethnic grouping (EG) and CV risk factors were investigated in multivariable logistic and linear regression models as appropriate and with consistent adjustment for age, sex, and healthcare center attendance. Prescribed antihypertensive therapy and statin use were further adjusted for when assessing associations with blood pressure and lipid variables, respectively.
The mean ± SD cIMT was compared between black and white patients by the Student t test and in age, sex, and healthcare center-adjusted linear multivariate logistic regression analysis; plaque prevalence was compared in univariate and age, sex, and healthcare center-adjusted multivariate logistic regression models.
To determine whether there were disparities in the relationships of modifiable CV risk factors with atherosclerosis in black compared to white patients, we assessed the associations of interactions between EG and the recorded risk factors with cIMT and plaque in multivariable regression models in which age, sex, and healthcare center and the individual terms were adjusted for, and subsequently performed stratified analysis.
The study was 95% powered to detect a significant (p < 0.01) difference in mean cIMT of 0.100 mm (the expected increase per 10-year age increment36) in multiple regression analysis with inclusion of 3 covariates between black and white Africans with RA. Statistical computations were made using the GB StatTM program (Dynamic Microsystems, Silver Spring, MD, USA).
RESULTS
Patient characteristics
Patient characteristics are shown in Tables 1 and 2. A total of 243 patients comprising 121 blacks and 122 whites were investigated. Black patients were more often women (p = 0.02) and were on average 2.4 years younger (p = 0.08) than their white counterparts. About 97% of black patients and 82% of whites were seen in public and private care, respectively.
Antihypertensives were used more frequently in black patients (54.6% vs 41.8%; OR 1.67, 95% CI 1.00–2.78) and statins more often in whites (36.1% vs 19.0%; OR 2.40, 95% CI 1.33–4.33). In confounder-adjusted analysis (Table 2), compared to whites, black patients experienced a higher prevalence of hypertension and had a higher diastolic blood pressure, but smoked less; their mean serum total cholesterol concentration was lower, but with concurrent numerically lower HDL cholesterol concentrations the total cholesterol/HDL cholesterol ratio was similar. These results translated into an overall major conventional CV risk burden, as estimated by the number of major risk factors and the Framingham score, that was similar in black and white patients. Disparities in other conventional CV/predisposing risk factors (Table 2) included a higher BMI, less frequent alcohol use, and a lower education level in black compared to white patients.
Among the nonconventional or predisposing CV risk factors shown in Table 2, black patients experienced extraarticular manifestations less often than their white counterparts. Although the geometric mean CRP concentrations were substantially higher (2.7 mg/l) in black compared to white patients (p = 0.002 in univariate analysis), this difference was not significant (p = 0.9) in age, sex, and healthcare center-adjusted analysis.
Carotid atherosclerosis in black and white Africans with RA
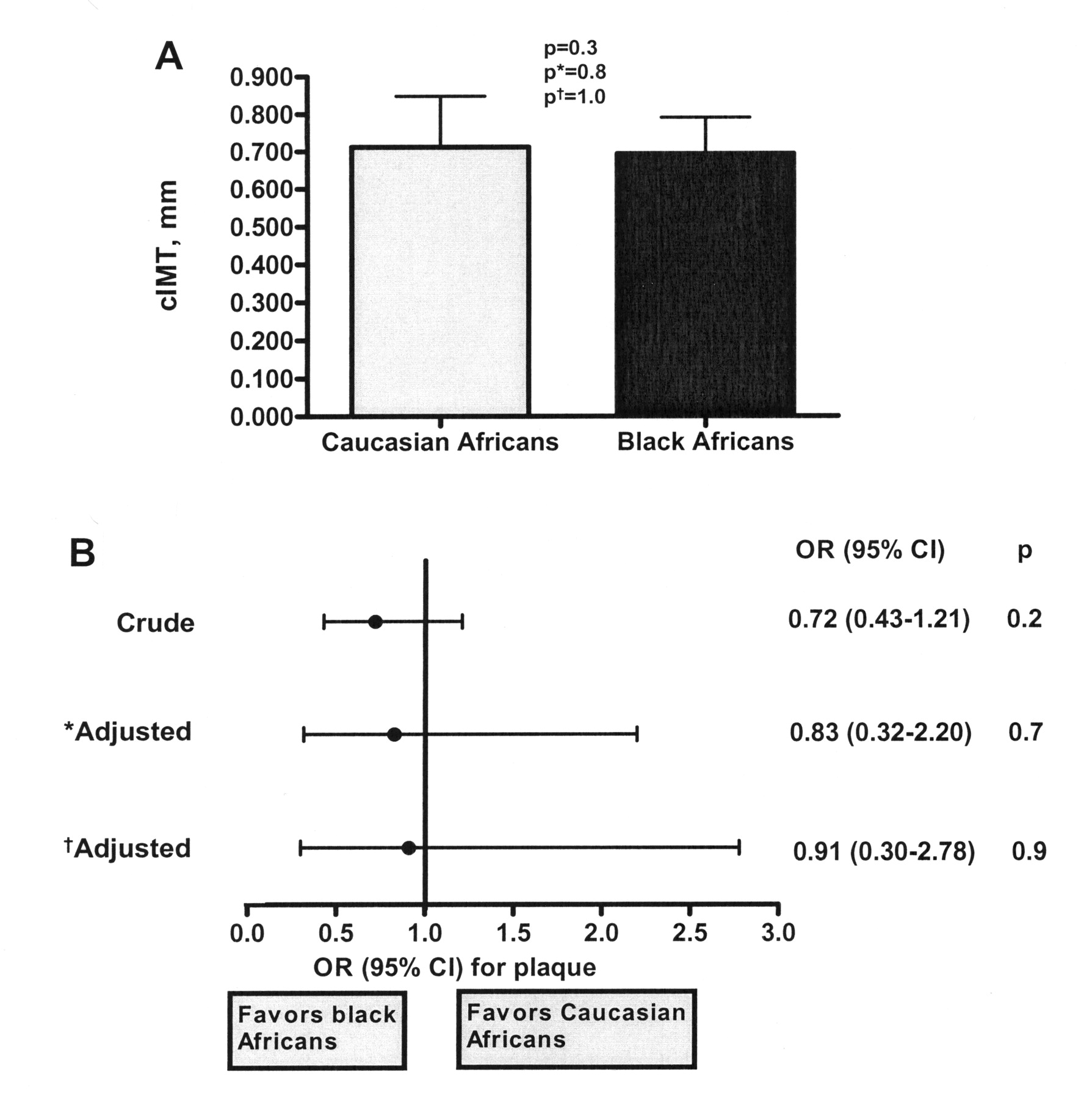
The mean cIMT was 0.694 ± 0.097 mm in black and 0.712 ± 0.136 mm in white patients with RA (p = 0.3). Forty-three of the black (35.5%) and 54 white patients (44.3%) had plaque (p = 0.3). As illustrated in Figure 1, these results were unaltered after adjustment for age, sex, and healthcare center and after further adjustment for disease duration and prednisone use as well as CV risk factors that differed between black and white patients (Table 2) and included hypertension, total and HDL cholesterol, pack-year smoking history, alcohol use, presence of extraarticular manifestations, education level, BMI, and number of deformed joints. The latter models in Figure 1 may be overfitted because 14 independent variables were entered, and hence any real difference between the mean cIMT and plaque prevalence between black and white patients could be disguised. However, when we entered disease duration, prednisone use, hypertension, total and HDL cholesterol, pack-year smoking history, alcohol use, the presence of extraarticular manifestations, education level, BMI, and number of deformed joints as potential confounders, each separately and together with age, sex, and healthcare center in different models, the results remained consistently unaltered: the cIMT remained similar in blacks compared to whites (p = 0.6 to 1.0) and population or ethnic grouping (EG) remained unassociated with plaque (OR 0.79 to 0.96, 95% CI 0.32–0.96, 95% CI 1.96–2.62, p = 0.5 to 0.9) in each of the models.
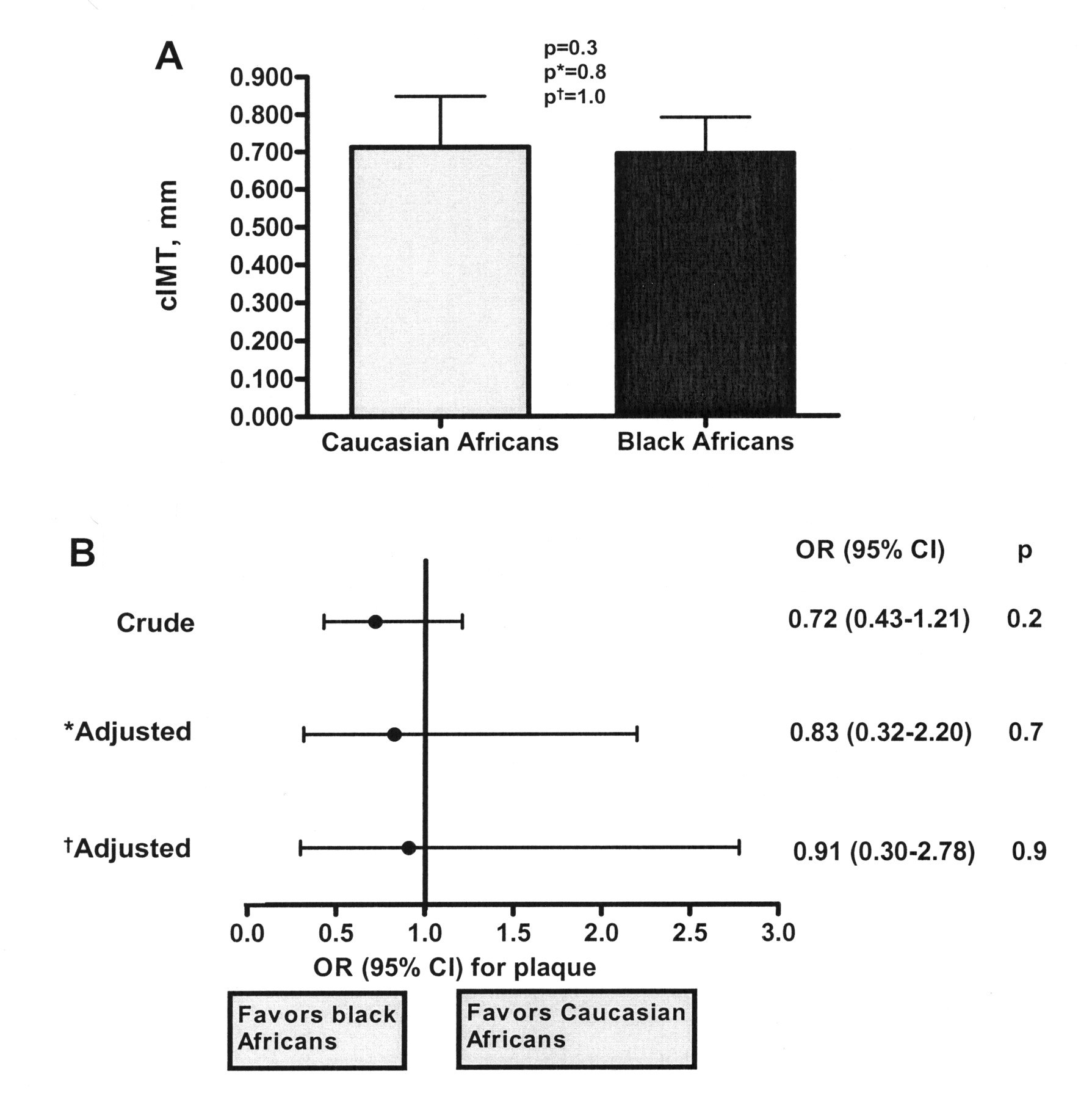
The carotid artery atherosclerosis burden in black and white Africans with rheumatoid arthritis (RA). A. Carotid intima-media thickness (cIMT) in black compared to white patients with RA. B. The association of population or ethnic grouping with carotid artery plaque. Results are expressed as mean (SD) and the corresponding p value in univariate analysis (Student t test) as well as p values in confounder-adjusted linear regression models in panel A, and as OR (95% CI) and the corresponding p values in univariate and confounder-adjusted logistic regression models in panel B. *Adjusted for age, sex, and healthcare center. †Further adjusted for disease duration and prednisone use as well as cardiovascular risk/predisposing factors that differed between black and white patients (Table 2) and included hypertension, total and HDL cholesterol, pack-year smoking history, alcohol use, presence of extraarticular manifestation, education, body mass index, and number of deformed joints.
Disparities in relationships of modifiable CV risk factors with carotid atherosclerosis in black compared to white patients with RA
In age, sex, and healthcare-adjusted analysis in all patients, these factors were associated with the cIMT: hypertension [partial correlation coefficient in multivariable linear regression model (pr) = 0.13, p = 0.04)], log HDL cholesterol concentrations (pr = −0.16, p = 0.01), LDL cholesterol concentrations (pr = 0.15, p = 0.02), non-HDL cholesterol concentrations (pr = 0.13, p = 0.04), BMI (pr = 0.13, p = 0.04), and DAS28 (pr = 0.13, p = 0.04). No CV risk factors were associated with plaque in all patients.
Interactions between EG and recorded individual CV risk factors (Table 2) that were associated with cIMT in all patients independent of confounders and individual terms are shown in Table 3; they comprised EG × systolic blood pressure, EG × total cholesterol/HDL cholesterol ratio, EG × CRP concentration, and EG × AIMS tension score. In stratified analysis, the systolic blood pressure, total cholesterol/HDL cholesterol, and CRP concentration were associated with the cIMT in white but not in black patients; conversely, the AIMS tension score was related to the cIMT in black but not in white patients. In an additional model, systolic blood pressure (pr = 0.21, p = 0.03), total cholesterol/HDL cholesterol (pr = 0.21, p = 0.03), and CRP concentration (pr = 0.21, p = 0.03) were associated with cIMT in whites, independent of one another and of confounders; further, the association of the AIMS tension score with cIMT among black patients with RA was materially unaltered (pr = 0.18, p = 0.07) after adjustment for socioeconomic factors as potential confounders and comprising marital status, education, alcohol use, and pack-year smoking history.
Associations of modifiable CV risk factors with common carotid intima-media thickness (cIMT) in black and white patients with RA separately. Significant associations are shown in bold type.
Interactions between EG and CV risk factors that were independently associated with carotid artery plaque are shown in Table 4; they comprised EG × systolic blood pressure, EG × extraarticular manifestations, EG × AIMS tension score, and EG × NSAID use. In stratified analysis, systolic blood pressure and presence of extraarticular manifestations were associated with plaque in white but not black patients; conversely, the AIMS tension score and NSAID use were related to plaque in black but not white patients. In additional models, systolic blood pressure (OR per 10-mm Hg increase = 1.37, 95% CI 1.03–1.82, p = 0.03) and the presence of extraarticular manifestations (OR 5.83, 95% CI 1.34–25.39, p = 0.02) in white patients and the AIMS tension score (0 to 10 scale; OR 1.42, 95% CI 1.05–1.92, p = 0.02) and NSAID use (OR 6.75, 95% CI 1.57–39.33, p = 0.03) in black patients were associated with plaque, independent of one another and confounders. Further, among black patients, the association of the AIMS tension score with plaque with RA was materially unaltered (OR 1.31, 95% CI 1.00–1.74, p = 0.05) after adjustment for socioeconomic factors as potential confounders and comprising marital status, education, alcohol use, and pack-year smoking history, and the association of NSAID use with plaque was independent of prednisone and DMARD use.
Associations of modifiable CV risk factors with carotid artery plaque in black and white patients separately. Significant associations are shown in bold type.
The analysis revealed that major conventional CV risk factors were related to the cIMT in white but not in black patients. This was confirmed upon assessment of whether the association of overall major conventional CV risk as estimated by the Framingham score with cIMT differed by ethnic group. Thus, the interaction term EG × Framingham score was associated with the cIMT independent of healthcare center and individual terms (p = 0.002; age and sex were not adjusted for in the respective model since these characteristics are used in calculating the Framingham score). In stratified analysis, the Framingham score was significantly associated with cIMT in white (pr = 0.47, p < 0.0001) but not in black (pr = 0.18, p = 0.06) patients.
DISCUSSION
We found the carotid artery atherosclerosis burden sustained by black Africans with established RA was similar to that in whites. An increased cIMT in the presence of hypertension may reflect arterial medial-layer hypertrophy rather than atheroma37. The cIMT was, however, similar in African black and white patients independent of a diagnosis of hypertension. Additionally, we found a marked variation in the independent associations between modifiable CV risk factors and atherosclerosis among black and white patients with RA. Our main findings each originated in several multivariable regression models adjusted for confounders. To our knowledge, this is the first study that simultaneously assessed and directly compared the atherosclerosis burden and its relationships with CV risk factors between patients with RA that belong to a developing and a developed population.
The acquisition of western lifestyles resulting in emerging CVD risk factors and events was recently documented in non-RA black Africans18,22. Nevertheless, CVD is still confirmed in only 6% of black South Africans that present to hospital with heart disease38. Our finding of a similar atherosclerosis burden in black and white patients with RA confirms that in the presence of RA, protection against CVD, mediated by the earlier epidemiological transition stage, may be absent in black Africans18.
Because hypertension was more frequent and the mean atherogenic index and CRP concentrations were similar in black compared to white patients in our study, it is particularly striking that the respective risk factors as well as the Framingham score were associated with atherosclerosis in whites only. This finding has 2 potential implications. First, major conventional CV risk factors and systemic inflammation may not be reliable in estimating CVD risk in black Africans that have developed established RA. This is in sharp contrast with reported findings in studies that were performed in developed populations and are congruous with our current results obtained in whites3,4,5,6,7,8,9,10. Because ultrasonographically identified atherosclerosis including both carotid cIMT and plaque was shown to predict CVD events not only in non-RA subjects but also in patients with RA and independent of population origin25,26,39, our results suggest that the use of direct vascular imaging may be more frequently indicated in optimal CV risk assessment in patients with RA from developing populations. Second, atherogenesis in black Africans with RA needs further investigation. The absence of associations of hypertension and dyslipidemia with atherosclerosis among black Africans with RA in our analysis does not exclude a role of major conventional risk factors in atherogenesis. Rather, because black Africans are currently undergoing a rapid socioeconomic transition18,20,22, upon reaching a mean age of 56 years as applied to those enrolled in our study, they are likely to sustain a shorter lifetime exposure to unhealthy lifestyles that could have contributed to our findings. Equally relevant, we recently reported that, compared to British white subjects, non-RA black Africans experience much greater aortic reflective waves and hence possibly greater aortic blood pressure values for a given brachial blood pressure40, and black Africans have reduced nocturnal blood pressure dipping that may produce target organ effects independent of conventional blood pressure41. Finally, we found that CRP concentrations were associated with atherosclerosis only in white Africans with RA. Interestingly, we recently documented prevalent high CRP concentrations in non-RA black Africans that were also not independently related to CVD risk as assessed by increases in aortic pulse pressure, the component waves, or the determinants of central pulse pressure42. Taken together, the potential contributions of major conventional risk factors and systemic inflammation to atherogenesis in black Africans with RA require assessment in future longitudinal studies and possibly central rather than brachial blood pressure evaluation40, the use of ambulatory 24-hour day and night blood pressure recording41, and direct measurement of inflamed joint-derived circulating cytokine concentrations43,44,45.
We found that the presence of extraarticular manifestations that reflect RA severity46 was independently associated with atherosclerosis in whites only. This disease characteristic was previously shown to be associated with atherosclerosis47 and to predict CV mortality in RA46. However, in keeping with an earlier report48, extraarticular disease was distinctly uncommon in black Africans with RA (2.5% vs 12.3% in whites; adjusted OR 0.19), and therefore a larger study may be required to adequately assess its potential influence on atherogenesis in patients with RA from this population.
Vascular reactivity to psychological stress is enhanced in black compared to white subjects and is associated with an increased susceptibility to atherosclerosis and incident CV events49,50,51. Stress reduction was shown to reduce carotid atherosclerosis and CV mortality in black Americans52. In our investigation, the AIMS tension score was independently associated with both the cIMT and plaque in black Africans with RA and not in whites; and in multivariable analysis, marital status, low education level, and smoking and alcohol use did not materially alter this relationship. Our results support the presence of an enhanced interconnectedness between mental and physical health23 that should be considered in optimal CVD prevention in black Africans with RA.
Selective COX-2 inhibition can enhance thrombosis risk and the development of hypertension53. However, the use of both traditional NSAID and selective COX-2 inhibitors increases CV event rates54. Variable effects of these agents in terms of atheroma development were reported in animal studies53. In our cohort, traditional NSAID use independently increased the OR for plaque 6-fold in black Africans with RA.
In addition to an earlier epidemiological health transition stage in black compared to white Africans, genetic differences between patients with RA from the 2 ethnic groups may alternatively or additionally support our findings. Indeed, in studies that included black and white populations, a different ethnic distribution of genetic polymorphisms that are associated with CVD, hypertension, and circulating lipid and CRP concentrations was found55,56,57,58,59,60. Further, specific patterns of associations between genetic variations in beta-adrenoreceptors and not only cold and but also psychological stress have been reported in young black individuals61. Finally, the potential importance of documented variations in CVD-related COX polymorphisms among white and black Americans62 deserves further study.
Compared to their white counterparts, black Africans with RA experience a similar burden of carotid atherosclerosis. These findings call for intensive CV risk management irrespective of epidemiological transition stage or population origin in patients with RA. However, relationships between cross-sectionally recorded modifiable risk factors and atherosclerosis vary considerably among Africans with RA. Longitudinal studies and possibly other than conventional CV risk factor evaluations are needed to further elucidate atherogenesis and optimal CV risk assessment in black Africans with RA.
Footnotes
-
Supported by a Medical Research Council Grant.
- Accepted for publication May 18, 2012.








{kind=link}