

Article Figures & Data
Figures
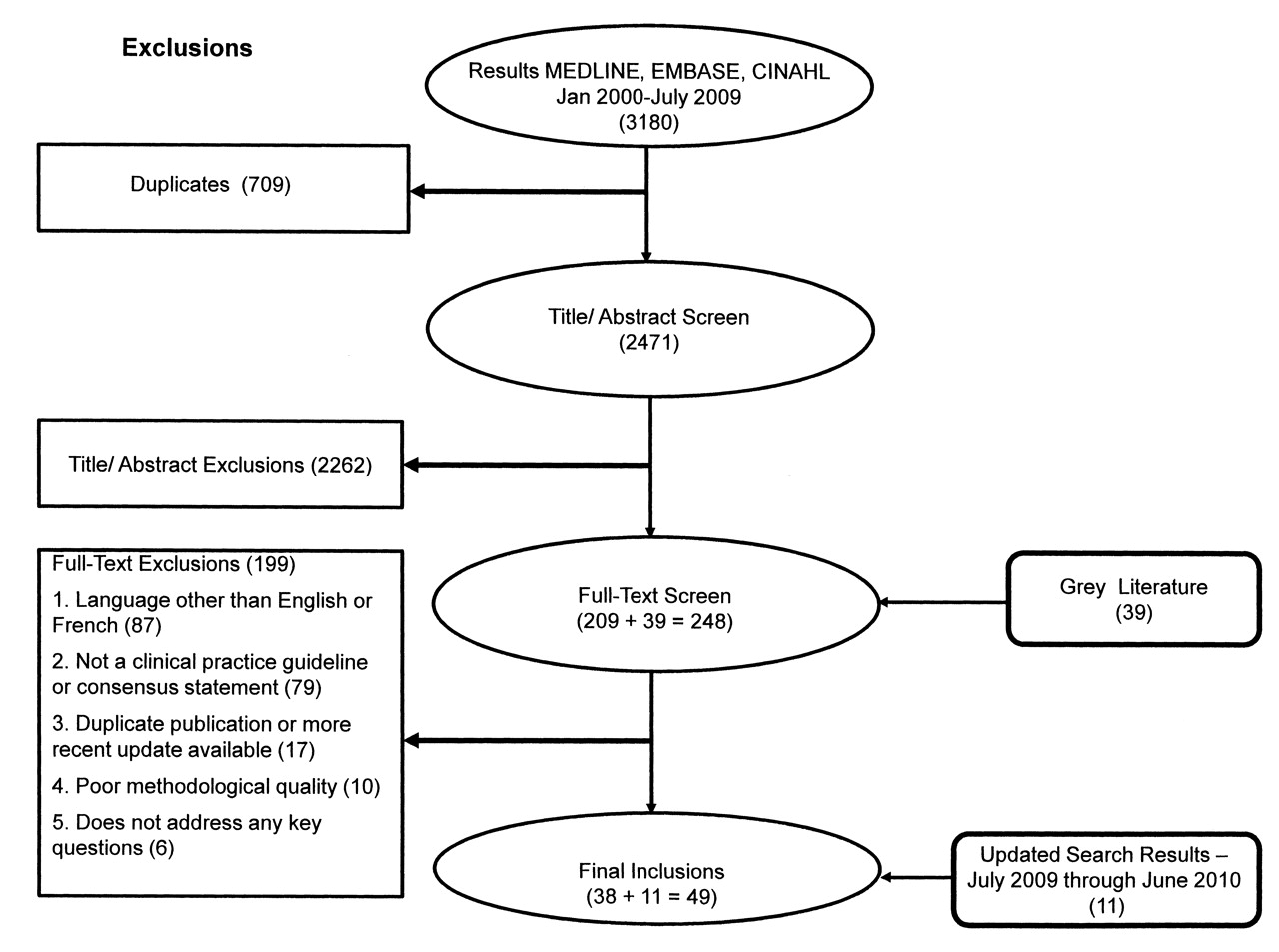
- Figure 1.
Steps in the systematic review of international guidelines on the pharmacological management of rheumatoid arthritis.
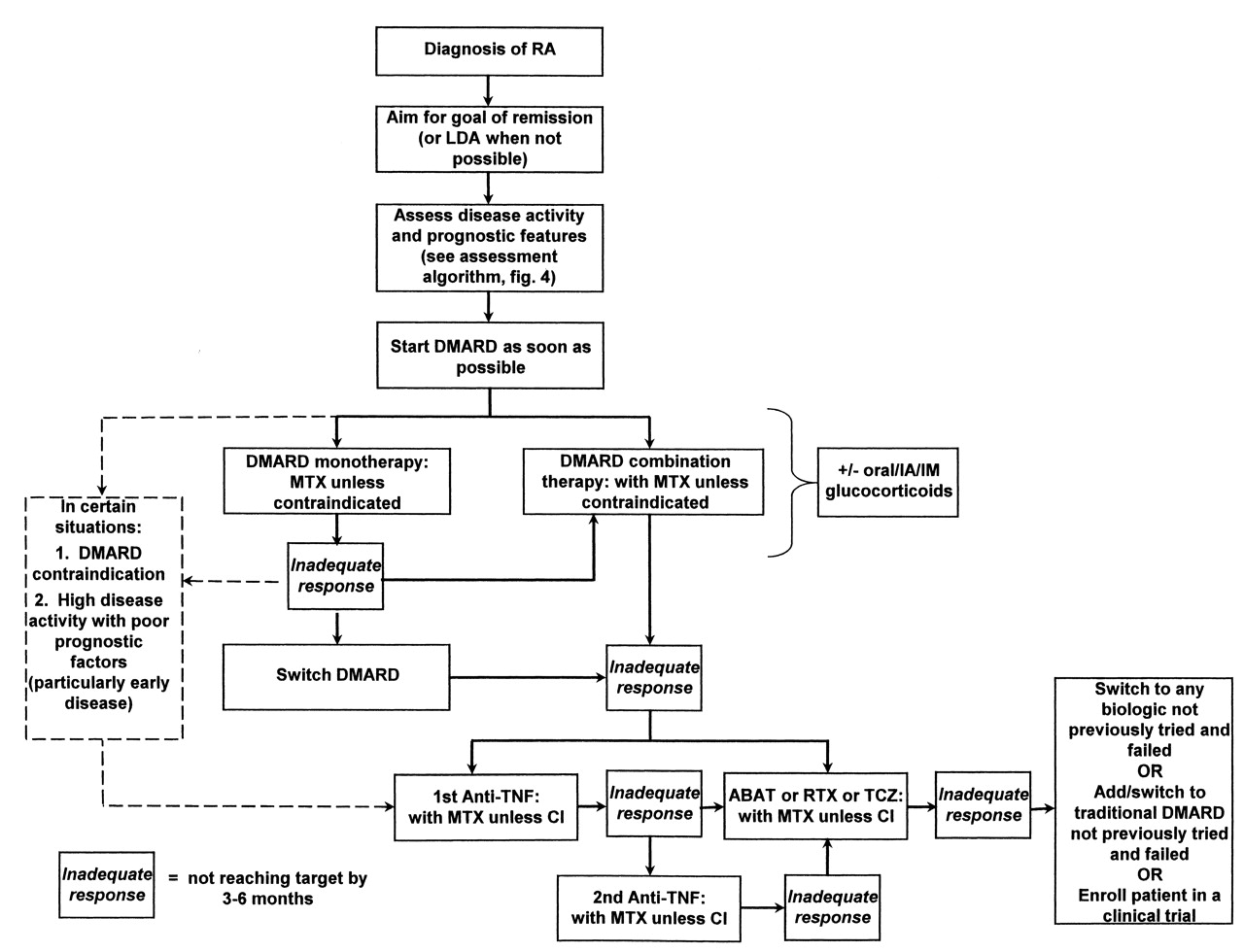
- Figure 2.
Algorithm based on the Canadian Rheumatology Association (CRA) recommendations for the pharmacological treatment of rheumatoid arthritis (RA) with traditional and biologic disease-modifying antirheumatic drugs (DMARD). LDA: low disease activity; DMARD: disease-modifying antirheumatic drug; CI: contraindicated; IA: intraarticular; IM: intramuscular; MTX: methotrexate; anti-TNF: tumor necrosis factor inhibitor; ABAT: abatacept; RTX: rituximab; TCZ: tocilizumab.
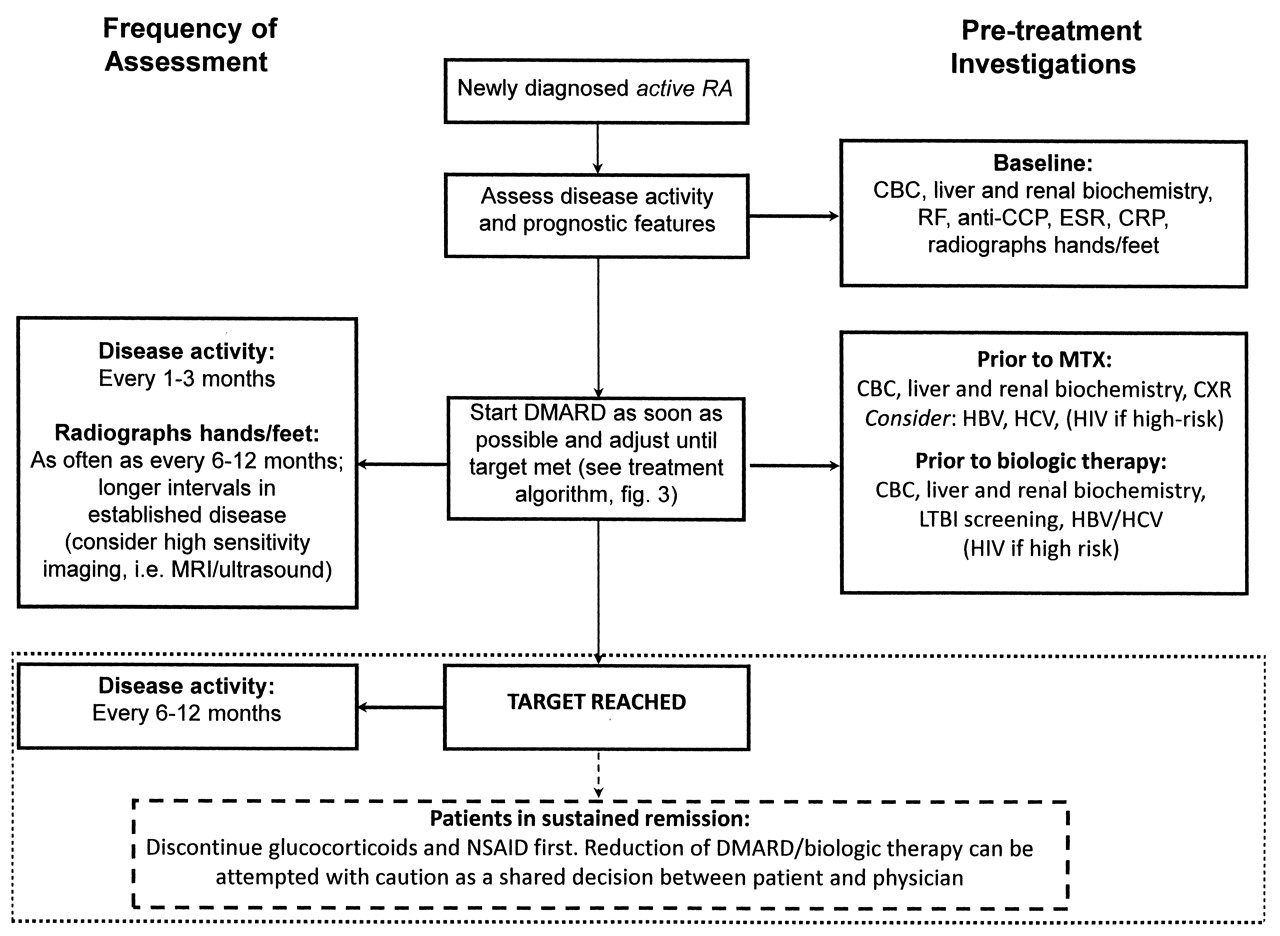
- Figure 3.
Algorithm based on the Canadian Rheumatology Association recommendations for the assessment of patients with rheumatoid arthritis (RA). DMARD: disease-modifying antirheumatic drug; NSAID: nonsteroidal antiinflammatory drugs; MRI: magnetic resonance imaging; CBC: complete blood cell count; RF: rheumatoid factor; anti-CCP: anticyclic citrullinated peptide antibodies; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; CXR: chest radiograph; LTBI: latent tuberculosis infection; HBV/HCV: hepatitis B/C.
Tables
- Table 1.
Key questions regarding the pharmacological treatment of patients with rheumatoid arthritis (RA).
General RA treatment strategies 1. What are the goals of treatment? 2. What are poor prognostic features that should be measured at baseline to inform treatment decisions? 3. How often should disease activity be monitored? 4. How often should the treatment strategy be adjusted in patients with RA? 5. How often should radiographs be ordered? 6. Should therapy be changed in RA patients with adequate clinical response but with unequivocal x-ray progression? Treatment with glucocorticoids 7. What is the role of glucocorticoids in the management of RA? Treatment with traditional DMARD (disease-modifying antirheumatic drugs) 8. When should DMARD be started? 9. Which DMARD should be used first? 10. Which investigations should be ordered prior to starting treatment with MTX? 11. What is the optimal dosing strategy for MTX? 12. When should combination therapy with traditional DMARD be used? 13. Which traditional DMARD combinations are preferred? 14. Should leflunomide be used in combination with MTX? Treatment with biologic DMARD 15. In patients being considered for treatment with biologic DMARD, how should an inadequate response to traditional DMARD be defined? 16. Which investigations should be ordered prior to starting treatment with biologic DMARD? 17. Should MTX be coprescribed with biologic DMARD? 18. When should anti-TNF therapy be used in the treatment of patients with RA? 19. When should abatacept be used in the treatment of patients with RA? 20. When should rituximab be used in the treatment of patients with RA? 21. How should patients be retreated with rituximab? 22. When should tocilizumab be used in the treatment of patients with RA? 23. Which therapeutic strategy is recommended after failure of 1 anti-TNF? 24. Which therapeutic strategy is recommended after failure of 2 anti-TNF? 25. Which therapeutic strategy is recommended after failure of abatacept, rituximab, or tocilizumab? 26. Should therapy be tapered or withdrawn in RA patients who achieve sustained remission? -
MTX: methotrexate; anti-TNF: tumor necrosis factor inhibitor.
-
Levels of Evidence Strength of Recommendation I Metaanalyses, systematic reviews of RCT, or individual RCT A Strong recommendation: -
Direct level I evidence
II Metaanalysis, systematic reviews of observational studies (cohort/case control studies), or individual observational studies B Moderate recommendation: -
Direct level II evidence or extrapolated level I evidence
OR RCT subgroup/post-hoc analyses III Nonanalytic studies, e.g., case reports, case series C Weak recommendation -
Direct level III evidence or extrapolated level II evidence
IV Expert opinion D Consensus recommendation: -
Expert opinion based on very limited evidence
NR Recommendations are not linked to evidence -
RCT: randomized controlled trial; NR: not reported.
-
- Table 3.
Canadian Rheumatology Association (CRA) recommendation for the pharmacological management of RA with traditional and biologic DMARD.
Recommendations Level Strength General RA management strategies 1. The goal of treatment is remission and, when not possible, minimal disease activity (I) while controlling symptoms, halting damage, preventing disability, and improving quality of life (IV) I, IV A 2. The presence of the following poor prognostic features should be assessed at baseline and considered when making treatment decisions: RF positivity, anti-CCP positivity, functional limitation, high number of swollen and tender joints, early erosions, extraarticular features, high ESR or CRP II B 3. RA care providers should monitor disease activity as frequently as every 1 to 3 months in patients with active RA (I). Patients with well controlled disease and patients in remission can be monitored at longer intervals (IV) I, IV A 4. Traditional and biologic DMARD therapy should be adjusted every 3–6 months, as long as the goal has not been achieved I, IV B 5. Radiographs of the hands and feet are recommended as frequently as every 6–12 months in patients with recent-onset disease (II). Radiographs can be performed at longer intervals in patients with established disease (IV) II, IV B 6. A change in therapy should be considered in patients with radiographic progression despite adequate clinical response IV D Treatment with glucocorticoids 7. Glucocorticoids (oral, intramuscular, or intraarticular) can be added to DMARD therapy as part of the initial treatment strategy of patients with RA (I), and may be an option for managing flares, as bridge therapy while waiting for DMARD to take effect, or for symptom control if no other options exist (IV). Glucocorticoids should be used in the lowest possible dose and tapered as rapidly as clinically feasible (IV) I, IV A/D Treatment with MTX/DMARD 8. In patients with persistent synovitis, DMARD should be introduced as soon as possible I A 9. MTX is the preferred DMARD with respect to efficacy and safety and should be the first DMARD used in patients with RA unless contraindicated I A 10. A complete blood count (II), liver (I) and renal biochemistry (II), and a chest radiograph (II) should be ordered prior to initiating MTX therapy. Screening for hepatitis B and C should be considered (III), and HIV testing is recommended in high-risk patients (IV) I–IV B/D 11. Dosing of MTX should be individualized to the patient (IV). MTX should be started oral or parenteral and titrated to a usual maximum dose of 25 mg/week by rapid dose escalation. In patients with an inadequate response or intolerance to oral MTX, parenteral administration should be considered (I) I, IV A 12. Initial combination therapy with traditional DMARD should be considered, particularly in patients with poor prognostic features, moderate-high disease activity, and in patients with recent-onset disease. Combination therapy should also be considered in patients who have an inadequate response to monotherapy I B 13. When treating with combination therapy, MTX should be used as the anchor drug unless contraindicated. Combinations not including MTX can be considered on a case-by-case basis I A 14. Combination therapy with leflunomide and MTX should be used with caution as it is associated with higher toxicity (gastrointestinal and liver) (I) and has no added benefit relative to other DMARD combinations (IV) I, IV A Treatment with biologics 15. In patients being considered for biologic therapy, an inadequate response to DMARD is defined as moderate to high disease activity despite treatment with at least 2 DMARD (including MTX unless contraindicated) in mono or combination therapy after 3 months at target dose IV D 16. Routine laboratory tests (complete blood count, liver and renal biochemistry) and screening for hepatitis B and C (and HIV in high-risk patients) are recommended prior to initiating all biologic therapy. Screening for latent tuberculosis is recommended prior to anti-TNF, abatacept, and tocilizumab. Baseline antinuclear antibody testing could be considered prior to starting anti-TNF IV D 17. MTX coprescription with biologics is recommended for improved efficacy I A 18. Anti-TNF therapy is recommended for treatment of patients with RA after an inadequate response to DMARD (I). In exceptional circumstances involving patients with DMARD contraindications or high disease activity and poor prognostic factors (particularly early disease), anti-TNF therapy may be an option after failure of DMARD monotherapy or in DMARD naive patients I A 19. Abatacept is recommended for the treatment of patients with RA after inadequate response to DMARD or anti-TNF therapy I A 20. Rituximab is recommended for the treatment of patients with RF-positive RA after an inadequate response to DMARD or anti-TNF therapy I A 21. Patients should not be expected to flare before they are retreated with rituximab (IV). Retreatment can occur as early as 6 months if the patient has had an initial response but has persistent synovitis (II) II, IV C 22. Tocilizumab is recommended for the treatment of patients with RA after inadequate response to DMARD or anti-TNF therapy I A 23. In patients who have failed treatment with 1 anti-TNF due to lack of efficacy or toxicity the following options are recommended: switch to another anti-TNF (I, II), switch to another biologic with a different mechanism of action (abatacept, rituximab, tocilizumab) (I), or add MTX (or other DMARD) if anti-TNF was used in monotherapy (II) I, II B 24. In patients who have failed treatment with 2 anti-TNF a switch to another biologic with a different mechanism of action (abatacept, rituximab, tocilizumab)) is recommended II/IV C 25. In the absence of data on therapeutic strategies after failure of abatacept, rituximab, or tocilizumab the following options can be considered: switch to any biologic not previously tried and failed, add or switch to a traditional DMARD not previously tried and failed, or enroll the patient in a clinical trial with a new agent IV D 26. If a patient achieves sustained remission after discontinuation of NSAID and glucocorticoids, a reduction in traditional and biologic DMARD can be attempted with caution as a shared decision between the patient and physician IV D -
RA: rheumatoid arthritis; DMARD: disease-modifying antirheumatic drug; anti-CCP: anti-cyclic citrullinated peptide antibody; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; HIV: human immunodeficiency virus; MTX: methotrexate; NSAID: nonsteroidal antiinflammatory drug; RF: rheumatoid factor.
-
Disease Activity Measures Remission Low Moderate High Formula ACR/EULAR Boolean-based definition for remission TJC28 ≤ 1, SJC28 ≤ 1, CRP ≤ 1 mg/dl, PGA ≤ 1 — — — Each criterion must be satisfied ACR/EULAR index-based definition for remission: Simple Disease Activity Index (SDAI) ≤ 3.3 — — — See details for SDAI below Disease Activity Score (DAS, range 0–10) < 1.6 1.6 to 2.4 > 2.4 to 3.6 > 3.6 [0.54*√(RAI)] + [0.065*44SJC]+ [0.33*In(ESR)] + [0.0072* GH] Calculator: http://www.das-score.nl Disease Activity Score 28 (DAS28, range 0–9.4)†† < 2.6 2.6 to 3.2 > 3.2 to 5.1 > 5.1 0.56 ×√ (TJC28) + 0.28 ×√ (SJC28) + 0.36 × In(ESR) + 0.014 × PGH + 0.96† Simplified Disease Activity Index (SDAI, range 0.1–86) ≤ 3.3 > 3.3 to 11 > 11 to 26 > 26 TJC28 + SJC28 + PGA + PhGA + CRP Clinical Disease Activity Index (CDAI, range 0–76) ≤ 2.8 > 2.8 to 10 > 10 to 22 > 22 TJC28 + SJC28 + PGA + PhGA Patient-reported Rheumatoid Arthritis Disease Activity Index (RADAI, range 0–10); data are medians — < 2.2 2.2 to 4.9 > 4.9 (PGA + patient reported disease activity based on SJC and TJC + pain + morning stiffness + TJC48)/items answered Patient Activity Scale (PAS or PASII, range 0–10) — ≤ 1.9 > 1.9 to 5.3 > 5.3 [(HAQ/HAQ-II*3.3) + pain + PGA]/3 Routine Assessment Patient Index Data (RAPID3, range 0–30) ≤ 3 3 to 6 > 6 to 12 > 12 MDHAQ functional score + pain + PGA -
↵† Calculator: http://www.das-score.nl.
-
↵†† Alternative DAS/DAS28 formulas based on the use of CRP rather than ESR are available from http://www.das-score.nl. Other cut points for the DAS28 have also been proposed (remission ≤ 2.4, low activity ≤ 3.6, high activity > 5.5)5. DAS: Disease Activity Score based on 44 joint counts; RAI: Ritchie Articular Index; DAS28: Disease Activity Score based on 28-joint counts; TJC28: tender joint count based on 28-joint count; SJC28: swollen joint count based on 28-joint count; ESR: erythrocyte sedimentation rate; PGH: patient global assessment of health [visual analog scale (VAS) 0–100 mm]; PGA: patient global assessment of disease activity (VAS 0–10 cm); PhGA: physician global assessment of disease activity (VAS 0–10 cm); CRP: C-reactive protein, mg/l; TJC48: tender joint count based on 48-joint count; HAQDI: Health Assessment Questionnaire Disability Index (0–3); HAQ-II: modified HAQ (0–3); MDHAQ: Multidimensional Health Assessment Questionnaire (0–10).
-










{kind=link}
{kind=link}
{kind=link}