

Abstract
Objective. To evaluate abatacept safety and efficacy over 5 years in patients with rheumatoid arthritis (RA) who had inadequate response to anti-tumor necrosis factor (TNF) therapy in the ATTAIN trial.
Methods. Patients completing the 6-month, double-blind (DB) placebo-controlled period were eligible to enter the longterm extension (LTE), where all patients received abatacept every 4 weeks (∼10 mg/kg, according to weight range). Safety, efficacy, physical function, and health-related quality of life were monitored throughout.
Results. In total, 317 patients (218 DB abatacept, 99 DB placebo) entered the LTE; 150 (47.3%) completed it. Overall incidences of serious adverse events, infections, serious infections, malignant neoplasms, and autoimmune events did not increase during the LTE versus the DB period. American College of Rheumatology responses with abatacept at Month 6 were maintained over 5 years. At Year 5, among patients who received abatacept for 5 years and had available data, 38/103 (36.9%) achieved low disease activity as defined by the 28-joint Disease Activity Score (DAS28)/C-reactive protein (CRP); 23/103 (22.3%) achieved DAS28/CRP-defined remission. Health Assessment Questionnaire response was achieved by 62.5% of patients remaining on treatment at Year 5; mean improvements from baseline in physical component summary and mental component summary scores were 7.34 and 6.42, respectively. High proportions of patients maintained efficacy and physical function benefits or improved their disease state at each timepoint throughout the LTE, if remaining on abatacept treatment.
Conclusion. Safety remained consistent, and abatacept efficacy was maintained from 6 months to 5 years, demonstrating the benefits of switching to abatacept in this difficult-to-treat population of patients with RA previously failing anti-TNF therapy.
Rheumatoid arthritis (RA) is a chronic, progressive disease that requires longterm therapy. It is important to examine the safety and clinical efficacy of RA therapy in the long term. Recent recommendations by the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) have specifically highlighted the need for clinical studies to evaluate the ability of a therapy to maintain responses over time1.
Anti-tumor necrosis factor (TNF) therapies have proven beneficial for many patients with RA. However, a considerable proportion of patients do not respond, lose their initial response over time, or are intolerant to anti-TNF agents2,3,4,5,6. Patients who discontinue one anti-TNF therapy either because of efficacy or safety/tolerability reasons often discontinue a second anti-TNF therapy for the same reason7,8,9. Patients for whom one or more anti-TNF therapies have failed represent a difficult-to-treat population that is refractory to multiple therapies. Switching such patients to a therapy with a different mechanism of action such as abatacept has proven effective10,11,12. It is of clinical importance to assess the efficacy and safety of the longterm administration of abatacept in this population.
Abatacept selectively modulates the CD80/CD86:CD28 costimulatory signal required for complete T cell activation13. Abatacept has been reported to provide benefits both in biologic-naive patients and in those with an inadequate response to anti-TNF treatment11,12,14. In the 6-month, double-blind (DB) period of the ATTAIN (Abatacept Trial in Treatment of Anti-TNF INadequate responders) trial, abatacept provided significant improvement versus placebo in the signs and symptoms of RA and in physical function in patients with active RA and inadequate response to anti-TNF therapy10. Significantly more abatacept-treated than placebo-treated patients achieved an ACR20 response [50.4% of abatacept group patients and 19.5% of placebo group patients (p < 0.001)] and clinically meaningful improvement in physical function [47.3% and 23.3% of abatacept and placebo group patients, respectively (p < 0.001)], the coprimary endpoints of the trial10. Efficacy results for abatacept were similar in patients for whom anti-TNF treatment had failed because of primary or secondary inefficacy. Over 6 months, abatacept treatment resulted in consistent decreases in mean 28-joint Disease Activity Score (DAS28) and Simplified Disease Activity Index (SDAI) scores, regardless of whether patients had experienced primary or secondary failure of their prior anti-TNF treatment (mean DAS28 and SDAI changes of −2.0 and −25.7 vs −2.0 and −24.3 for primary vs secondary anti-TNF failures treated with abatacept; −0.9 and −13.4 vs −0.9 and −13.1 for those treated with placebo)15. At Year 1, DAS28-defined low disease activity state (LDAS) was achieved by 24.4% and 23.7% of abatacept-treated patients, who had experienced primary and secondary treatment failure, respectively, and 25.5% and 21.6% of patients who had experienced the failure of 1 or 2 anti-TNF agents, respectively16.
The results of the 18-month open-label, longterm extension (LTE) of the ATTAIN trial showed that these short-term efficacy benefits were maintained through 2 years of abatacept treatment11. Further, abatacept demonstrated a consistent safety profile between the DB period and the LTE11. We evaluate the safety, efficacy, and physical function benefits over 5 years of intravenous (IV) abatacept treatment in patients with RA and an inadequate response to anti-TNF therapy in the ATTAIN trial. These data represent the longest followup available for abatacept treatment after inadequate response to anti-TNF agents reported to date.
MATERIALS AND METHODS
Patients
Patients who completed the 6-month DB period of the ATTAIN trial11 were eligible to enter the LTE. Patients had active RA and an inadequate response to anti-TNF therapy because of lack of efficacy following ≥ 3 months of etanercept or infliximab treatment, or both administered sequentially10. This study was initiated before adalimumab was widely available. At randomization, patients had to have ≥ 10 swollen joints, ≥ 12 tender joints, and C-reactive protein (CRP) levels ≥ 1 mg/dl.
Study design
The design and conduct of the ATTAIN study (clinical trial registration number NCT00124982) have been reported in detail10,11. In brief, the longterm extension of the ATTAIN trial assessed the safety and tolerability of abatacept in combination with background disease-modifying antirheumatic drugs (DMARD); efficacy was also assessed during the LTE.
Patients who entered the open-label LTE received abatacept, regardless of their initial randomization group in the DB period (abatacept or placebo); abatacept was administered as a 30-minute IV infusion every 4 weeks at a fixed dose of about 10 mg/kg, according to weight range (reassessed yearly). All patients continued to receive 1 or more background DMARD throughout, and dose adjustments were permitted at the discretion of the investigator. Use of marketed biologics and anti-TNF therapies was not allowed. Patients completed the study when abatacept became commercially available in their country; if abatacept was not available commercially in their country at Year 5, patients could remain in the study until it was terminated by the sponsor.
Safety assessments
Safety assessments were performed monthly during the LTE, and included monitoring of adverse events (AE) and serious AE [SAE; as classified by the Medical Dictionary for Regulatory Activities (MedDRA), version 11.1], changes in vital signs, and physical examination. Reported infections were based on the system organ class of infections and infestations within MedDRA. Safety data are presented up to Year 5 (6-month DB + 4.5-year LTE) of the study.
Clinical assessments
Signs and symptoms of RA were assessed by ACR20, ACR50, and ACR70 response criteria17. Disease activity was assessed by DAS28 based on C-reactive protein (CRP), with LDAS defined as DAS28 ≤ 3.2 and DAS28-defined remission as DAS28 < 2.618. Assessments for ACR responses and DAS28 were taken quarterly up to Year 3 and at 6-month intervals thereafter; these are presented up to Year 5 (6-month DB + 4.5-year LTE). Physical function was evaluated by the Health Assessment Questionnaire Disability Index (HAQ-DI)19,20, with HAQ response defined as an improvement of 0.3 units in HAQ-DI from baseline; annual HAQ-DI assessments are presented up to Year 5 (6-month DB + 4.5-year LTE).
Health-related quality of life
Health-related quality of life (HRQOL) was assessed using Medical Outcomes Study Short-Form 36 questionnaire (SF-36) scores [Physical Component Summary (PCS) and Mental Component Summary (MCS)]. Changes in SF-36 scores from baseline were evaluated to Month 6 and then yearly up to Year 5 (6-month DB + 4.5-year LTE).
Shift analysis
In addition to the group-level analyses, posthoc shift analyses of disease states were performed for the subgroups of abatacept-treated patients who achieved moderate disease activity state (MDAS), LDAS, and remission at Month 6 and maintained or improved their disease state from Month 6 to Years 1, 2, 3, 4, and 5. Shift analysis was also performed for those patients treated with abatacept who were in high disease activity state (HDAS) at Month 6 and who improved their disease state from Month 6 to Years 1, 2, 3, 4, and 5. For these analyses, HDAS was defined as DAS28/CRP > 5.1, MDAS as DAS28/CRP > 3.2–5.1, LDAS as DAS28/CRP ≤ 3.2, and remission as DAS28/CRP < 2.6.
Statistical analysis
Baseline demographics and clinical characteristics were analyzed descriptively for all patients who received at least 1 abatacept dose during the LTE.
Safety data presented for the cumulative (6-month DB period + 4.5-yr LTE = 5 yrs total duration) study period are based on all patients who received at least 1 abatacept dose in the LTE; events that occurred up to 56 days after the last dose of abatacept are included. Incidence rates were calculated for SAE, infections, serious infections, malignancies, and autoimmune events as the number of patients with the event of interest divided by exposure to the study drug in patient-years and multiplied by 100, to express events/100 patient-years of exposure. A patient’s contribution to the incidence rate of an individual AE ended at the time of the event’s first occurrence.
Efficacy and HRQOL data are presented for patients originally randomized to abatacept during the DB period who received at least 1 abatacept dose during the LTE, and have data available at the visit of interest (as-observed analysis). The post-hoc shift analyses were based on as-observed data for patients originally randomized to abatacept during the DB period who received at least 1 abatacept dose during the LTE with data available at Month 6 and the visit of interest (Years 1, 2, 3, 4, or 5).
RESULTS
Patient disposition
A total of 317 patients (218 patients from the original abatacept group and 99 patients from the original placebo group) entered the LTE (Figure 1)11,10; 47.3% (150/317) completed the LTE. The most common reasons for discontinuation during the LTE were lack of efficacy (69/317 patients; 21.8%) and AE (37/317 patients; 11.7%). Of the 69 patients discontinuing for lack of efficacy, 24 (35%) were originally treated with placebo in the DB period. The number of patients discontinuing treatment declined progressively throughout each year of the study (Figure 1).

Patient disposition. *An additional 2 patients discontinued (1 poor/noncompliance and 1 for other reason) more than 56 days after the last dose of the study treatment and are not included here. †Patients remained on abatacept treatment, either on commercially available drug or, for 29 patients from countries where abatacept was not commercially available, by continuing in the trial beyond Year 5. ‡In addition to the deaths described, a further patient discontinued because of an adverse event and subsequently died. DB: double blind; LTE: longterm extension.
Baseline demographics and baseline characteristics
These data for patients participating in the LTE were similar across original DB treatment groups (Table 1). Patients had a high degree of baseline disease activity, based on the mean number of tender and swollen joints (Table 1). Baseline mean HAQ-DI scores were 1.8 (SD 0.6) and DAS28/CRP 6.5 (SD 0.8) for both original treatment groups.
Demographics and clinical characteristics at baseline of double-blind study for patients who later entered the longterm extension. Values are mean ± SD unless otherwise stated.
Concomitant medications
Methotrexate (MTX), cortico-steroids, and nonsteroidal antiinflammatory drugs (NSAID) were the medications most frequently taken concomitantly with abatacept during the LTE (82.0%, 83.9%, and 83.0%, respectively); use of these remained stable over time.
Safety summary
During the cumulative study period, the mean exposure to abatacept was 43.4 months (range 3.7–75.2) for patients who entered the LTE. Upper respiratory tract infection (URTI), bronchitis, nasopharyngitis, sinusitis, and back pain were the most frequently reported AE during the LTE. The overall incidence rates for SAE, infections, serious infections, malignant neoplasms, and autoimmune events did not increase during the LTE relative to the DB period (Table 2).
Summary of safety during the ATTAIN trial.
Serious AE were reported in 136 patients during the LTE, at an incidence rate of 19.18 events/100 patient-years. The most frequently reported SAE by class were musculoskeletal and connective tissue disorders (n = 67), with RA accounting for the majority of events.
Six deaths were reported during the LTE. Causes were respiratory distress, asphyxia, arterial embolism of mesenteric artery, metastatic neoplasm, natural causes, and staphylococcal wound infection. One death (the staphylococcal wound infection) was considered possibly related to the study drug.
Infections
Infections and serious infections were reported in 254 and 34 patients during the LTE, respectively, with an incidence rate of 107.75 and 3.50 events/100 patient-years, respectively (Table 2). The most frequently reported infections (in ≥ 10% of patients) were URTI (n = 105), bronchitis (n = 66), nasopharyngitis (n = 61), sinusitis (n = 59), urinary tract infection (n = 57), and influenza (n = 32). The most frequently reported serious infections were pneumonia (n = 15), cellulitis (n = 2), and sepsis (n = 2); all other serious infections were reported in only 1 patient each.
Of the reported serious infection SAE, 1 event each of enterobacter pneumonia and sepsis (in 1 patient), and acute pyelonephritis and bacteremia (in 1 patient) were classified as very severe in intensity by the investigator. No cases of opportunistic infections, including tuberculosis, were reported during the DB or LTE periods.
Malignancies
A total of 21 malignant neoplasms were reported during the LTE (incidence rate: 2.11 events/100 patient-yrs; Table 2). The most frequently reported malignant events were basal cell carcinoma (n = 6) and squamous cell carcinoma (n = 6). The remaining events were reported in 1 patient each. The metastatic neoplasm (Grade III) that led to death was diagnosed at Day 1155 in a patient originally randomized to placebo, with a history of cancer. On Day 1255, the patient died as a result of metastatic adenocarcinoma, primary site unknown.
Two lymphomas were reported in the LTE: 1 was a non-Hodgkin T cell lymphoma and 1 was non-Hodgkin B cell lymphoma. The latter occurred in a patient with a history (> 5 yrs prior to study initiation) of diffuse large B cell lymphoma who was randomized to abatacept during the DB period. This lymphoma had not resolved at the last available report and abatacept was discontinued as a result of this event.
Autoimmune events
Autoimmune events were reported in 17 patients during the LTE, resulting in an incidence rate of 1.70 events/100 patient-years (Table 2). Most of these events were considered unrelated to the study drug. Psoriasis was the most frequently occurring autoimmune event (n = 4), and events were mild or moderate in intensity.
Two cases of autoimmune hepatitis were reported. One patient originally randomized to placebo, with a history of Raynaud phenomenon, was diagnosed with type I autoimmune hepatitis and treated with methylprednisolone. Abatacept was discontinued because of this event, which was continuing at the last available report. One patient originally randomized to abatacept in the DB period, with a history of elevated liver function tests, fatty liver, and a family history of systemic lupus erythematosus, presented with elevated liver chemistry while not taking MTX. The patient was diagnosed with severe/grade III autoimmune hepatitis and treated with prednisone. The study drug was discontinued because of this event.
Clinical efficacy
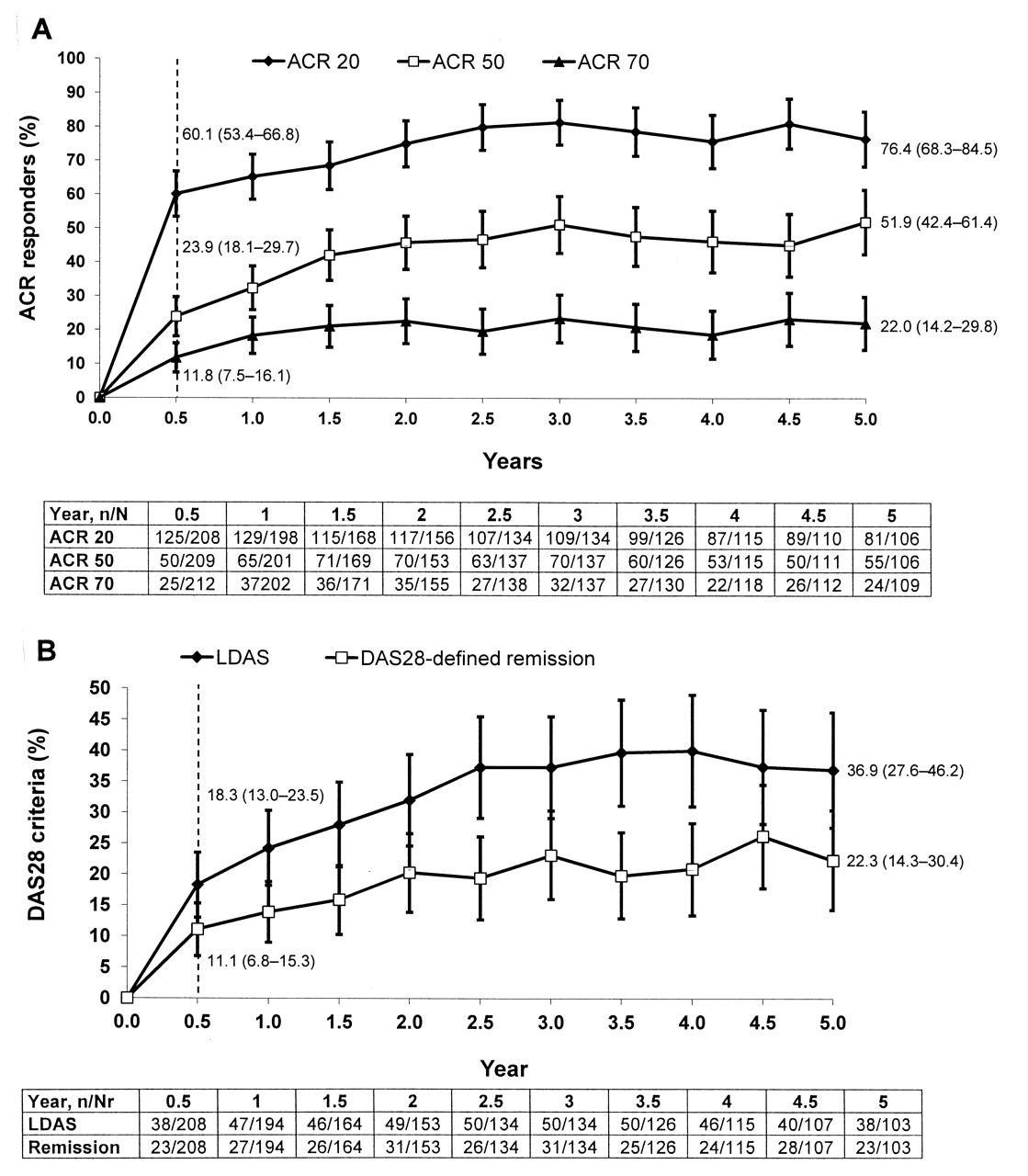
Mean improvements in ACR20, ACR50, and ACR70 responses observed at Month 6 were maintained over 5 years in patients who remained on abatacept therapy (Figure 2A). Similarly, the proportions of patients with low levels of disease activity (LDAS or remission) observed at Month 6 were maintained throughout the LTE for patients who remained on abatacept therapy. At Year 5, 38/103 patients (originally randomized to abatacept) achieved LDAS and 23/103 patients achieved DAS28 (CRP)-defined remission (Figure 2B). Mean change from baseline in DAS28 (CRP) was −2.00 (95% CI −2.19, −1.80) at Month 6 (n = 205) and −2.89 (95% CI −3.16, −2.82) at Year 5 (n = 101).
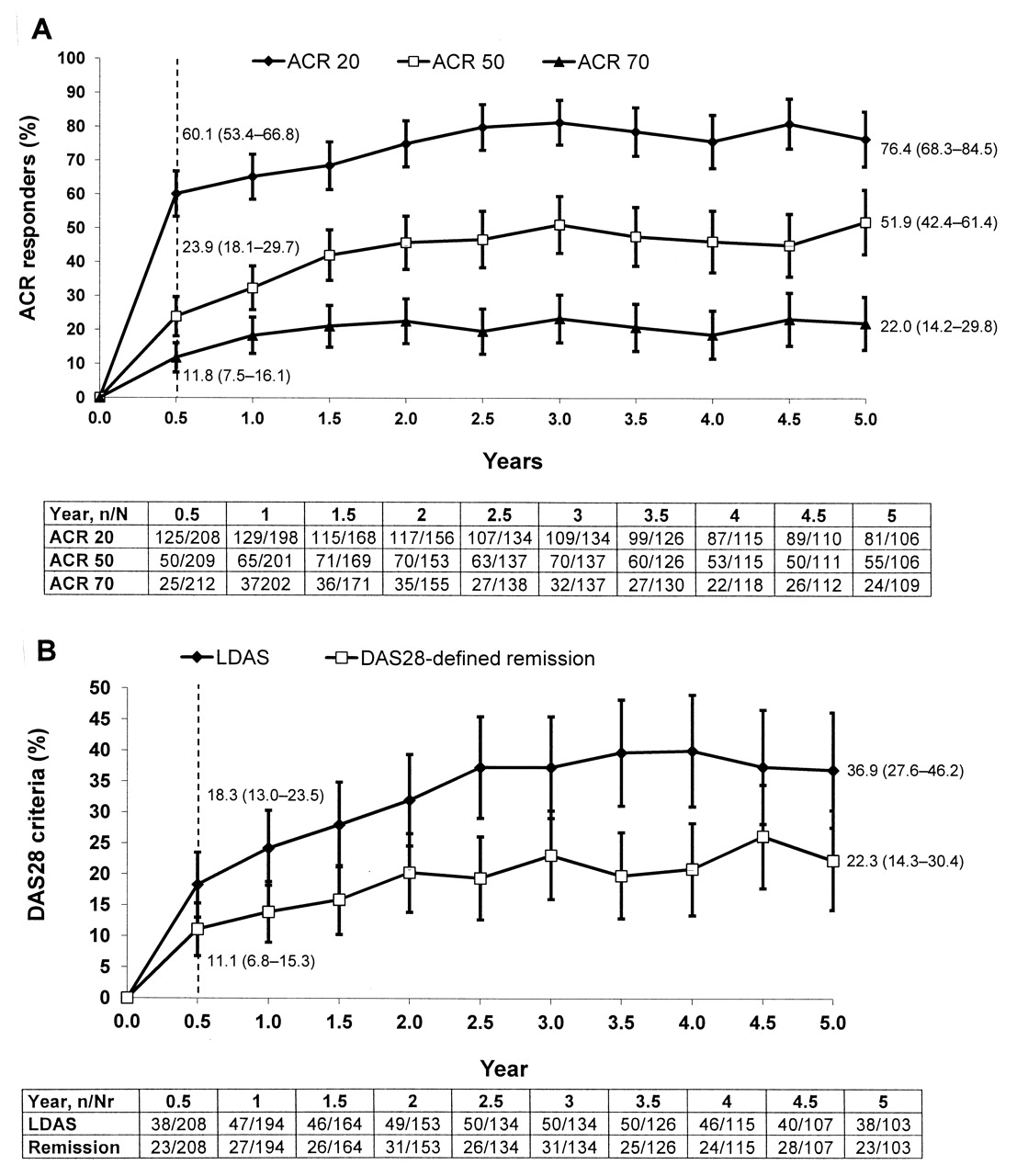
Clinical efficacy. A. Proportion of patients achieving American College of Rheumatology (ACR) 20, 50, and 70 response rates over 5 years. B. Proportion of patients achieving low disease activity state (LDAS), defined as 28-joint Disease Activity Score (DAS28) C-reactive protein (CRP) ≤ 3.2 and DAS28/CRP-defined remission (DAS28/CRP < 2.6) over 5 years. All data are based on posthoc as-observed analyses of patients originally randomized to abatacept, and are presented with 95% CI; both double-blind (Day 1 to Month 6) and longterm extension (Month 6 to Year 5) data are presented.
Mean improvements in physical function, as assessed by mean change from baseline in HAQ-DI score, were maintained between Month 6 [–0.51 (95% CI −0.59, −0.43), n = 207] and Year 5 [–0.57 (95% CI −0.69, −0.45), n = 104] for patients originally randomized to abatacept (Figure 3). At Month 6, 115/207 (55.6%) patients achieved a HAQ response (improvement of at least 0.3 units from baseline in HAQ-DI), and 65/104 patients (62.5%) who remained on treatment achieved this response at Year 5.
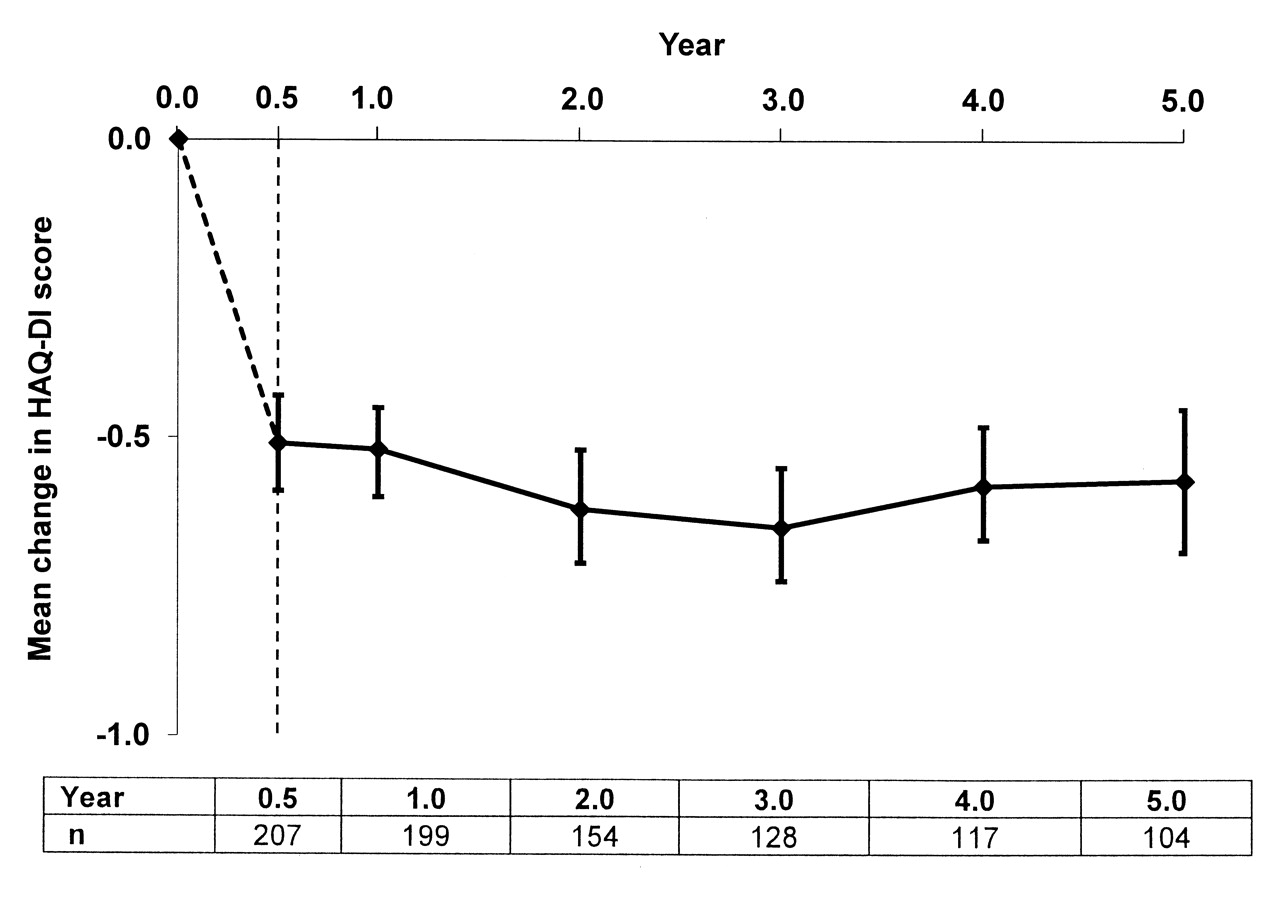
Physical function. Mean change from baseline in Health Assessment Questionnaire-Disability Index (HAQ-DI) score. Mean (± SD) baseline HAQ-DI score was 1.8 ± 0.6. All data are based on posthoc as-observed analyses of patients originally randomized to abatacept. Both double-blind (Day 1 to Month 6) and longterm extension (Month 6 to Year 5) data are presented.
HRQOL
Mean improvements from baseline to Month 6 in PCS and MCS (n = 204 for both) were 7.46 (95% CI 6.11–8.81) and 5.83 (95% CI 4.18–7.47), respectively. These improvements were maintained throughout the LTE, and at Year 5 mean changes from baseline in PCS and MCS (n = 103 for MCS, n = 104 for PCS) were 7.34 (95% CI 4.94–9.74) and 6.42 (95% CI 3.97–8.87), respectively.
Shift analyses
Shifts in disease state from Month 6 to each subsequent year are presented in Table 3. Of those patients who were in HDAS at Month 6, 56.7% had improved their disease state by Year 1 and 78.1% of these patients had improved their disease state at Year 5 with continued abatacept treatment. Of those patients who were in MDAS at Month 6, 82.9% had improved or maintained their disease state by Year 1. At each subsequent year, 85.7%–88.6% of these patients maintained or improved their disease state with continued abatacept treatment, and at Year 5, 95.9% of these patients had maintained or improved their level of disease activity. Of those abatacept-treated patients who had achieved LDAS at Month 6, 55.6%–65.4% maintained LDAS or achieved remission to Year 5 with continued abatacept treatment. Of those abatacept-treated patients who achieved remission at Month 6, 61.9% of these patients maintained remission at Year 1 and over half maintained remission at each subsequent year to Year 4 with continued abatacept treatment. At Year 5, 40.0% of these patients had maintained remission.
Summary of shift in rheumatoid arthritis disease states during the ATTAIN trial. Numbers in parentheses are definitions of disease states, by 28-joint Disease Activity Score/C-reactive protein levels. Data represent as-observed analysis in patients who had data available at Month 6 and at the timepoint considered.
DISCUSSION
During the ATTAIN trial, the safety and efficacy of abatacept treatment in patients with active RA and an inadequate response to anti-TNF therapy were evaluated over 5 years. The data reported here represent one of the longest randomized clinical trial analyses of a biologic in anti-TNF-refractory patients with RA. At Year 5, roughly half the patients who entered the LTE remained on abatacept treatment. The yearly discontinuation rate during the LTE decreased over time, with few dropouts due to AE. Of the discontinuations due to lack of efficacy, 35% occurred in patients originally treated with placebo, meaning that their first exposure to abatacept was during the LTE; this suggests that they discontinued because of a lack, rather than a loss, of efficacy. Of patients who discontinued because of loss of efficacy, 71% discontinued within the first 2 years of treatment (up to 1.5 years of the LTE).
The safety of IV abatacept over the 5-year cumulative study period was found to be consistent with that reported for the 6-month DB period10. The incidence rates of malignancies and infections in the cumulative study period were comparable to those reported in the DB period and did not increase over time (2.11 and 107.75 events per 100 patient-years of exposure for malignancies and infections in the cumulative period, respectively). No cases of opportunistic infections, including tuberculosis, were reported. Incidence rates of overall serious infections were toward the lower range of those previously reported in clinical trials of patients with RA treated with anti-TNF therapies21, and did not increase relative to the incidence of serious infections in patients switching anti-TNF therapy, as reported in a recent metaanalysis22. These findings are consistent with a recent Cochrane Review suggesting that abatacept is associated with a lower incidence of SAE and serious infections than some biologics (OR 0.65 and 0.57, compared with control)23. However, these data should be interpreted in the context of the patient population enrolled in the ATTAIN trial; these patients were highly selected and had failed their prior anti-TNF because of inefficacy only, and so were not representative of patients in clinical practice.
For those patients who received abatacept throughout the cumulative period, mean improvements in signs and symptoms of RA, disease activity, physical function, and HRQOL that were achieved during the DB period were maintained throughout the LTE. The level of improvement in clinical efficacy seen with abatacept treatment over the short term is similar to that seen with other biologics, as shown in both mixed patient populations, in a Cochrane Review metaanalysis (adjusted for placebo treatment), and in patients who had failed previous anti-TNF therapy, in a EULAR/ACR systematic review24. Meaningful proportions of patients from this refractory population achieved significant improvement in RA signs and symptoms, disease activity, and physical function (ACR50 response, LDAS, or normalized HAQ) and maintained these improvements during the LTE.
Patient-level analyses of shifts in disease state supported the findings from the group-level analyses, with high proportions of patients maintaining or improving the disease state achieved at Month 6 throughout each year of the LTE if they remained on abatacept treatment. Favorable shifts in disease state were observed in high proportions of patients in HDAS at Month 6, with continued abatacept treatment, despite patients in ATTAIN having highly active RA at enrollment and being refractory to prior treatments. For a molecule such as abatacept, which demonstrates sustained treatment responses at the group level, these data for individual patients are of particular clinical interest and relevance. Although these data should be interpreted within the context of the small patient numbers available for the shift analyses, these observations indicate that abatacept treatment induces a shift in disease activity across all disease states. As well as achieving and maintaining low disease activity or remission, continued abatacept treatment can elicit improvement, even in those patients with high levels of disease activity who were refractory to other treatment strategies.
These data should be interpreted within the context of the limitations of the study. The patients had high levels of disease activity at entry and their prior anti-TNF therapy had not been effective. Therefore they may not be representative of patients typically found in clinical practice. It should be noted that the data presented here are based on as-observed analyses, which are potentially vulnerable to the discontinuation of patients responding less well to treatment. However, applying imputation over the long term would not be meaningful, given that about 50% of patients remained in the trial25. Here, in agreement with a recent publication offering guidance on the reporting of longterm extension studies25, we present longterm data at the group level, in addition to the shift in disease state at the individual patient level.
Overall, these data from the ATTAIN trial and the LTE demonstrate the benefits of switching to abatacept from anti-TNF therapy, including consistent safety and longterm sustained clinical efficacy. These data also support the longterm use of abatacept as an effective and well-tolerated therapeutic option in this difficult-to-treat population of patients with RA whose previous anti-TNF therapy had failed.
Acknowledgment
The authors thank Tracy Li and Jean-Claude Becker, who were employees at Bristol-Myers Squibb at the time of the study, for their valuable contribution to the ATTAIN study; Coralie Poncet (Docs International, Sèvres, France) for statistical support, and Eve Guichard (Medicus International) for editorial assistance.
Footnotes
-
Supported by Bristol-Myers Squibb. Dr. Genovese and Dr. Schiff have received consulting fees from Bristol-Myers Squibb. Dr. Luggen has received research grants from Bristol-Myers Squibb. Dr. Le Bars and Dr. Elegbe are employees and shareholders of Bristol-Myers Squibb. Dr. Aranda was an employee and shareholder of Bristol-Myers Squibb at the time of the study. Dr. Dougados has received consulting fees, research grants, speakers’ bureau fees, and honoraria from Bristol-Myers Squibb.
- Accepted for publication May 11, 2012.








{kind=link}
{kind=link}
{kind=link}