

Abstract
Objective. For patients with rheumatoid arthritis (RA), recommendations are inconclusive about whether tumor necrosis factor-α (TNF-α)-blocker therapy should be evaluated at 3 or 6 months. Biomarkers are needed to predict at 3 months which patients would benefit from further treatment because of nonoptimal response. Our objective was to investigate whether serum etanercept (ETN) concentrations and anti-ETN antibodies at 3 months are predictors of clinical response to ETN at 6 months in patients with RA in terms of European League Against Rheumatism criteria and Disease Activity Score in 28 joints (DAS28).
Methods. Between 2009 and 2010, we included 19 women with active RA who were candidates for ETN therapy. Response criteria were evaluated at 3 and 6 months. Serum concentrations of ETN and anti-ETN antibodies were measured by ELISA at baseline and at 3 and 6 months.
Results. Eighteen patients completed followup. Three-month ETN concentrations were lower for 6-month nonresponders than responders (p = 0.03). Three-month ETN levels correlated significantly with change in DAS28 between baseline and 6 months (r = −0.62, p = 0.006). The best predictor of response at 6 months was observed with an ETN threshold of 3.1 μg/ml at 3 months. No anti-ETN antibodies were found.
Conclusion. ETN concentrations at 3 months predict response to ETN therapy at 6 months. Low ETN concentrations could explain the absence of response to ETN, suggesting that patients with low ETN levels could benefit from increased ETN dose or earlier interruption of treatment.
The European League Against Rheumatism (EULAR) and the American College of Rheumatology (ACR) recommend evaluating the efficacy of tumor necrosis factor-α (TNF-α) inhibitors at 3 months in patients with rheumatoid arthritis (RA), whereas the British Society for Rheumatology and the British National Institute for Health and Clinical Excellence recommend that treatment not persist beyond 6 months in case of uncontrolled disease activity1,2 (London: National Institute for Health and Clinical Excellence; Website: www.nice.org.uk/nicemedia/pdf/TA130guidance.pdf). Previously, a significant proportion of nonresponders at 3 months were found to respond at 6 months3. The question in daily practice is often whether to continue TNF inhibitors after 3 months in light of nonoptimal response. Biomarkers that predict the benefit of an additional 3 months of treatment are needed.
In this prospective pilot study, we assessed serum concentrations of etanercept (ETN) and anti-ETN antibodies at baseline and 3 and 6 months and the correlations with treatment response evaluated by EULAR criteria. We investigated whether ETN concentrations and anti-ETN antibodies at 3 months were predictors of clinical response to ETN at 6 months in patients with RA. Our secondary objective was to assess the optimal threshold of these markers for treatment decisions.
MATERIALS AND METHODS
Patients
We included 19 patients aged 18 years or older with RA satisfying the ACR criteria, revised in 1987. All patients were candidates for TNF inhibitors according to international guidelines. All were TNF inhibitor-naive. Clinical response was determined by the EULAR criteria and the Disease Activity Score in 28 joints (DAS28). Responders were defined as moderate and good EULAR responders. Low disease activity was defined as DAS28 2.6–3.2 and remission as DAS28 < 2.6. The study was approved by the local ethics committee (Montpellier, France), and informed consent was obtained from patients in accord with the Helsinki Declaration of 1975 (revised in 1983).
All patients received ETN 50 mg subcutaneously once a week. Combination with a synthetic disease-modifying antirheumatic drug (sDMARD) was permitted.
ETN concentrations and anti-ETN antibodies
Fasting blood was collected in dry tubes at baseline and after 3 and 6 months of ETN. All samples were collected prior to the next ETN injection. Tubes were centrifuged at 3600 RPM for 8 min at 4°C and frozen at −80°C. Simultaneous assays of ETN levels and neutralizing anti-ETN antibodies were carried out with LISA-Tracker Premium® ETN kits (LTE001; Biomedical Diagnostics®, Marne la Vallee, France). This test was developed according to the French Health Products Safety Agency and the European Union quality criteria.
Dosage of etanercept
Serum ETN levels were measured using ELISA. The assay is based on the ability of ETN to bind its ligand. TNF-α is coated onto a polystyrene microtiter plate. The diluted sample is added to the antibody-coated well to allow binding. After incubation, unbound proteins are removed by washing. Anti-human IgG biotinylated antibody is added. Again, unbound antibodies are removed by washing. Horseradish peroxidase (HRP)-labeled streptavidin is added. The streptavidin binds to the complex formed with biotinylated anti-IgG antibodies. After incubation, the wells are washed again to eliminate any excess of conjugate. The bound enzyme is revealed by addition of substrate TMB (3,3′,5,5′ tetramethylbenzidine). The color intensity is proportional to the amount of ETN. H2SO4 (0.25 M) is added to stop the enzymatic reaction. The optical density is read by a spectrophotometer at 450 nm. The detection limit is 0.2 μg/ml (95th percentile). Intra-run coefficient of variation (CV) ranged from 1.1% to 2.4% and inter-run CV from 4.9% to 13.9% depending on ETN concentrations.
Dosage of anti-ETN antibodies
ETN is coated onto a polystyrene microtiter plate. First, the diluted sample is added to the antibody-coated well to allow binding. After incubation, unbound proteins are removed by washing. Biotinylated ETN is added. After incubation, unbound antibodies are removed by washing. HRP-labeled streptavidin is added. The last steps are similar to those for ETN detection. Limit of detection is 5 ng/ml (95th percentile). As a positive control for anti-ETN antibody detection, monoclonal human anti-IgG antibodies recognizing the Fc portion of ETN (thus bridging ETN and biotinylated ETN) were used. Intra-run CV ranged from 3.0% to 8.1% and inter-run CV from 10.8% to 13.0% depending on anti-ETN antibody concentrations. The assay measures only free ETN and free anti-drug antibodies. Anti-ETN antibodies and ETN complexes are not detected. Thus, only active ETN and anti-ETN antibodies that have linked all ETN are measured. All measures were performed twice. In case of discrepancies in the first 2 results, a third measure was performed.
Interfering substance study
The LISA-Tracker Premium result for ETN was evaluated by Biomedical Diagnostics to assess potential crossreactivity to other antibodies and interference from serum components (complement: n = 4; IgG or IgM monoclonal immunoglobulins: n = 3; cryoglobulinemia: n = 1; triglycerides: n = 2; hemolyzed sera: n = 2; rheumatoid factors: n = 5; heterophilic antibodies: n = 5; warmed sera: n = 5; autoimmune antibodies: n = 7). None of the samples were positive for ETN or anti-ETN antibodies.
Statistical analysis
Data are expressed as mean ± SD, mean (range), and number (%). We compared ETN concentrations between responders and nonresponders by nonparametric Mann-Whitney test and the correlations between biomarker concentrations and changes in DAS28 by Spearman correlation coefficient. Sensitivity and specificity were calculated for each threshold of TNF-α and ETN concentration using logistic regression. As the cutpoint varies, the locus of “1 – specificity” (on the X-axis) and sensitivity (on the Y-axis) yields a bow-shaped receiver operating characteristic (ROC) curve. Then an optimal threshold was selected, taking into account the optimal threshold cutpoint from the ROC curve and the relative consequences of correct diagnosis and misdiagnosis4.
RESULTS
Baseline characteristics and response to therapy
At baseline, the median age of the women was 56 years (range 27–77) and median RA duration was 5 years (range 1–38). Rheumatoid factor (RF) and anticitrullinated protein antibodies were positive in 72% and 67% of patients, respectively. Eleven patients had RF > 100 IU/ml and 4 had RF > 300 IU/ml. Radiographic erosions were found in 78%. Median DAS28 score was 4.85 (range 3.14–7.62). In total, 12 patients received concomitant treatment with methotrexate (MTX) and 5 with leflunomide; 2 had no combination of sDMARD. One patient dropped out because of a disease flare requiring an early change of therapy (baseline DAS28 was 5.1; 3-month DAS28 was 6.5). At 3 months, she had an ETN concentration of 1.2 μg/ml.
At 3 months, the median change in DAS28 was −1.2 (range −4.4 to 1.8) and 72.2% of patients were responders according to the EULAR criteria. Half of the patients showed low disease activity and one-third had disease remission. From 3 to 6 months, the median decrease in DAS28 was 1.1 (range −4.8 to 1.0). At 6 months, 66.7% of patients were responders; 38.8% showed low disease activity and 27.8% had disease remission. From 3 to 6 months, 3 patients (16.7%) showed a changed EULAR response status: 1 nonresponder became a responder and 2 responders became nonresponders. After 1 year, 60% of the patients were still treated with ETN (9/15).
ETN concentrations and anti-ETN antibodies
Two patients had undetectable ETN concentrations at 3 months. Both had had to stop therapy in the previous 2 weeks, 1 with a urinary tract infection and the other because of ongoing dental care. ETN concentrations were stable between 3 and 6 months (median 3.6 μg/ml, IQR 2.0–4.6, and 3.4 μg/ml, IQR 2.12–4.25, respectively; p = 0.67). There was no correlation between ETN dosage at 3 months and RF titers (r2 = 0.004, p = 0.81); and ETN concentrations at 3 months were not different between patients with RF > 300 IU/ml and those with RF < 300 IU/ml (3.2 μg/ml, IQR 2.27–3.9, vs 3.3 μg/ml, IQR 1.0–6.7, respectively; p = 1.00).
No anti-ETN antibodies were found at baseline or at 3 or 6 months.
ETN concentrations and response to therapy
At 3 and 6 months, median ETN concentrations were higher, but not significantly, for responders than for nonresponders (3 months: 3.6 μg/ml, IQR 2.2–4.4, vs 2.1 μg/ml, IQR 0.1–3.7, respectively; p = 0.10; 6 months: 3.6 μg/ml, IQR 2.5–4.4, vs 2.4 μg/ml, IQR 0.4–5.8; p = 0.40). Serum ETN concentration at 3 months was inversely correlated with the change in DAS28 at 3 months (r = −0.50, p = 0.03, respectively). Six-month ETN concentration was inversely correlated, although not significantly, with change in DAS28 at 6 months (r = −0.48, p = 0.06).
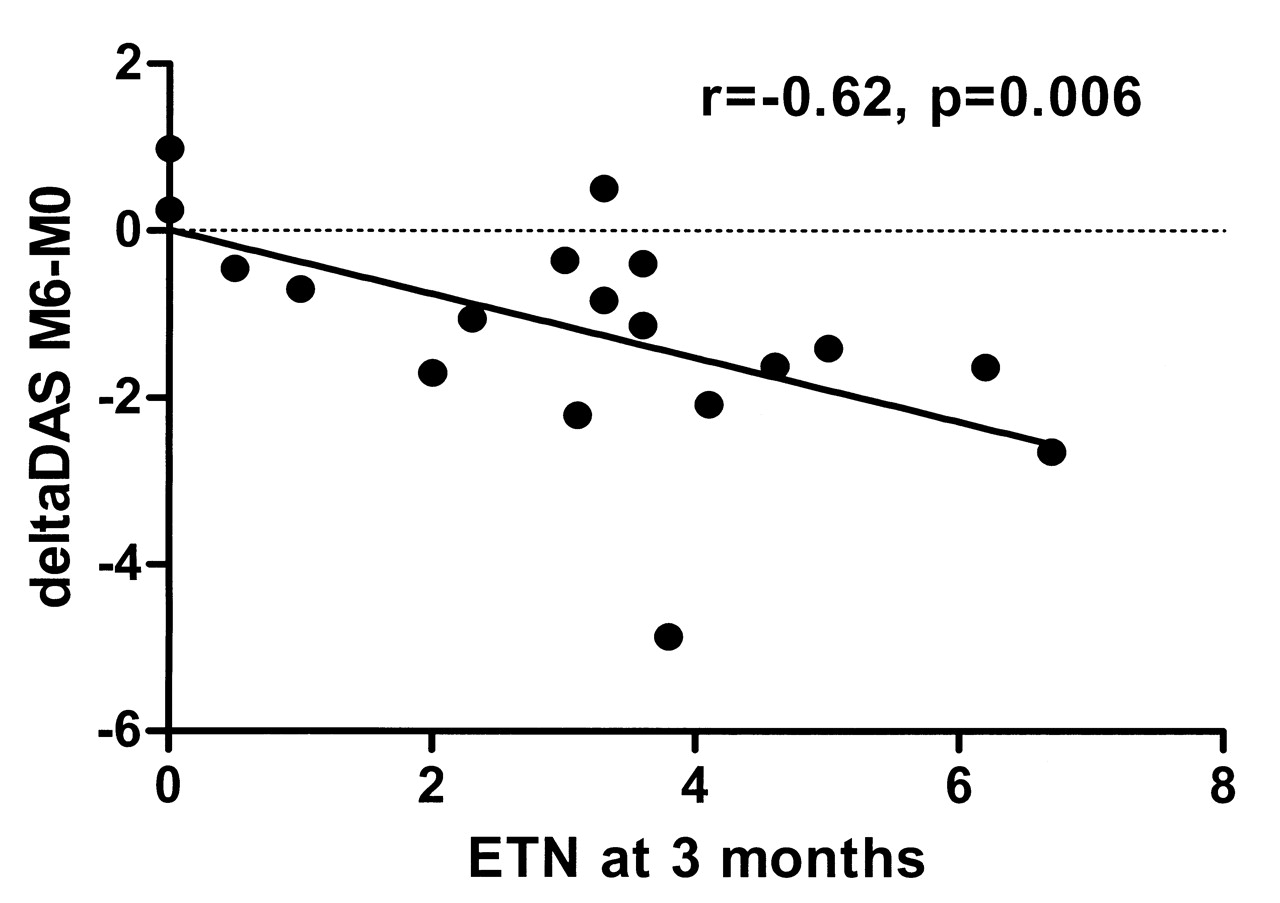
At 3 months the median ETN concentration was significantly lower for 6-month nonresponders than for responders (1.75 μg/ml, IQR 0–3.6, vs 3.70 μg/ml, IQR 1.0–6.7, respectively; p = 0.03; Figure 1). The 3-month ETN concentration was significantly correlated with change in DAS28 between baseline and 6 months (r = −0.62, p = 0.006; Figure 2). When data from patients with undetectable ETN levels were excluded, the 3-month ETN concentrations were still inversely correlated with change in DAS28 between baseline and 6 months (r = −0.49, p = 0.05).
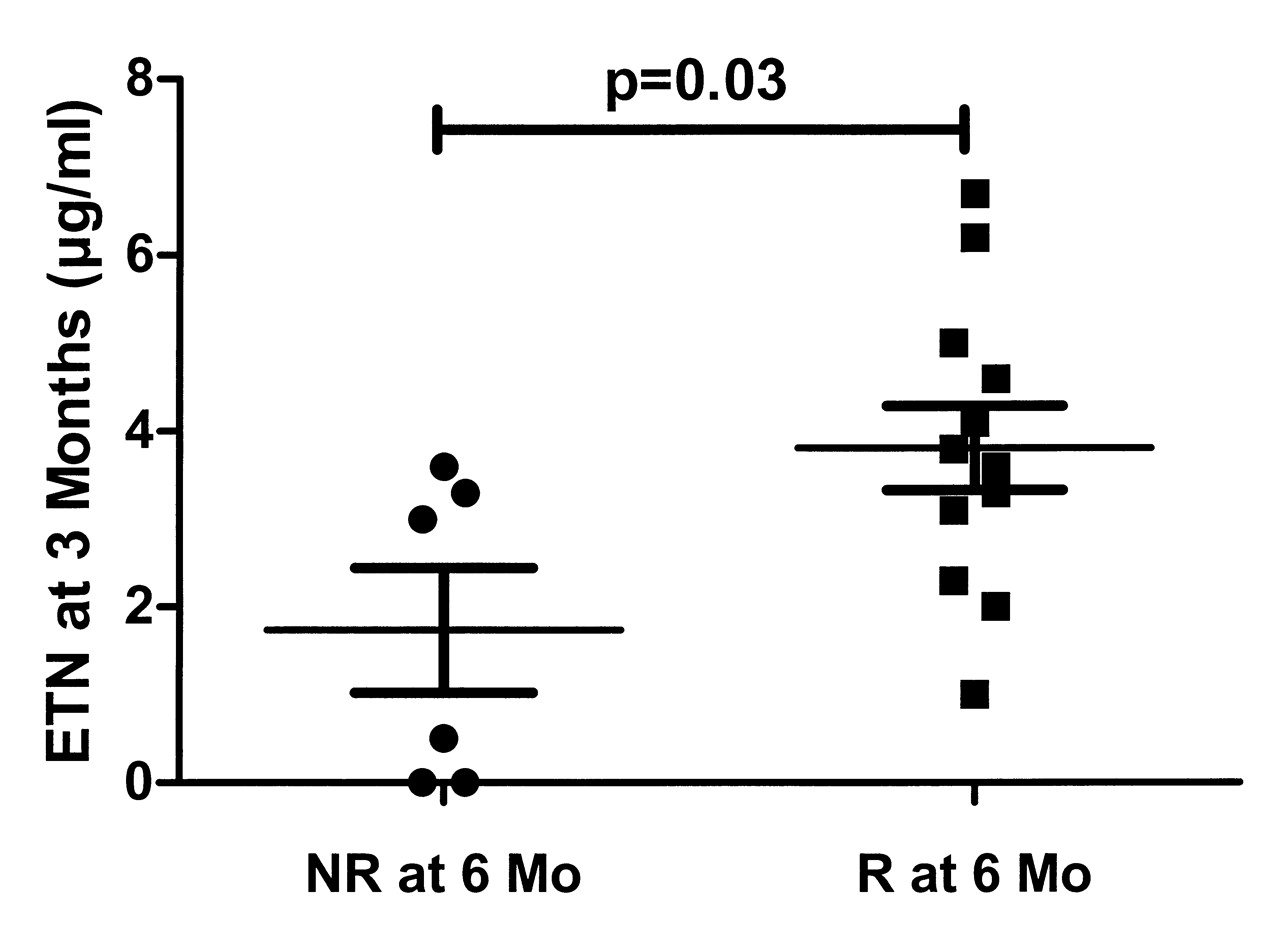
Comparison of 3-month etanercept (ETN) concentrations in nonresponders (NR) and responders (good and moderate responders; R) according to European League Against Rheumatism criteria at 6 months.

Correlations between 3-month serum concentrations of etanercept (ETN) and change in Disease Activity Score in 28 joints (DAS28) between baseline and 6 months.
C-reactive protein (CRP) changes between baseline and 3 months tended to correlate negatively with ETN concentrations at 3 months (r = −0.46, p = 0.08). ETN concentrations at 3 months correlated significantly with CRP changes in the first 6 months (r = −0.73, p = 0.004).
ETN concentration thresholds
The threshold for response to treatment was assessed by 3-month ETN concentrations for 6-month nonresponders and responders. In prediction analyses, sensitivity and specificity were the probability that the predictor would identify a true responder and a true non-responder, respectively. Optimal thresholds to predict treatment response were assessed by the relative consequences of correct prediction and misprediction at 6 months. We used a high sensitivity threshold because the risk of supplementary 3-month treatment would be acceptable for a potential nonresponder. For ETN, a concentration of 3.1 μg/ml was associated with a sensitivity of 87% and a specificity of 67% (Table 1). With this threshold, the DAS28 at 6 months was significantly higher in patients with low than in those with high median 3-month ETN concentrations (4.43, IQR 2.50–5.23, vs 2.94, IQR 1.82–4.57; p = 0.02; Figure 3). Similar results were found after excluding the 2 patients with undetectable ETN levels at 3 months (2.94, IQR 1.82–4.57, vs 4.43, IQR 2.50–5.23; p = 0.05). The therapeutic maintenance at 1 year was 33.3% (2/6) and 77.8% (7/9) for patients with 3-month ETN level < 3.1 and ≥ 3.1 μg/ml, respectively (p = 0.11).

Disease Activity Score in 28 joints (DAS28) at 6 months in patients with serum etanercept (ETN) concentrations above or below 3.1 μg/ml at 3 months. Patients represented as white symbols have undetectable ETN at 3 months.
Sensitivity and specificity of thresholds of serum etanercept (ETN) concentration in predicting Disease Activity Score in 28 joints at 6 months for patients with rheumatoid arthritis.
DISCUSSION
In this study, ETN concentration was closely associated with response to treatment, and ETN concentrations at 3 months predicted response to ETN therapy at 6 months. Low ETN concentrations could explain the absence of response to ETN, suggesting that patients with low ETN levels could benefit from increased doses or earlier interruption of treatment and rotation to another biologic treatment.
Results we obtained with this new commercial LISA-Tracker kit were consistent with those reported by Jamnitski, et al5. ETN concentrations were very close in the 2 studies: 3.30 μg/ml, IQR 1.2–4.1, at 3 months in our study compared to 3.25 μg/ml, IQR 2.08–4.71, at 4 months for Jamnitski; and 3.40 μg/ml, IQR 2.0–4.4, vs 3.44 μg/ml, IQR 2.34–4.78, respectively, at 6 months. No anti-ETN antibody was found in either study. Further, we did not observe any RF interference in our study.
Anti-drug antibodies (ADAb) against ETN are very rare (0%–5%) and do not seem to influence response to therapy, because all are non-neutralizing5,6,7. ADAb are usually directed against the Fab fraction, which is missing in ETN, as compared with monoclonal antibodies. However, small quantities of anti-ETN antibodies cannot be excluded because the assay does not detect the ETN/anti-ETN complexes. Conversely, ADAb are more frequent with monoclonal anti-TNF antibodies, and those are closely related to drug concentration8,9,10,11. For ETN, the concentrations may be explained by many patient variables, such as weight, liver enzymes, or genetics, that result in variable drug metabolisms. Concomitant treatments such as sDMARD can also influence the pharmacokinetics of biologics, but in RA, an association of MTX therapy does not influence serum ETN concentrations, unlike adalimumab concentrations12.
We found that ETN concentrations influenced response to treatment, with a correlation between 3-month serum ETN concentrations and decreased DAS28 scores at 3 months. Similar results were previously found with monoclonal antibodies (infliximab and adalimumab)8,9,10,11. Jamnitski, et al5 also showed a relation between drug concentrations and response to ETN, with higher drug levels in EULAR good responders at 6 months compared to EULAR nonresponders [(n = 103) median 3.78 μg/ml, IQR 2.53–5.17, vs (n = 74) median 2.80 μg/ml, IQR 1.27–3.93, respectively; p < 0.05].
Pocock, et al3 showed that 57% of patients with non-response to TNF inhibitor at 3 months (n = 21) could respond at 6 months. For half of the patients, continuing ETN therapy after 3 months would be beneficial, but the authors did not know which ones. We found a significant correlation between serum ETN and TNF-α concentrations at 3 months and response to treatment at 6 months. ETN concentrations at 3 months also correlated significantly with CRP changes between baseline and 6 months (r = −0.73, p = 0.004). One-year therapeutic maintenance in patients with low ETN concentrations was less than half that of patients with high ETN concentrations. We determined that for patients with partial response at 3 months and a high ETN concentration (≥ 3.1 μg/ml), therapy could be continued for at least 3 more months (Figure 4). For patients with a low ETN concentration (< 3.1 μg/ml), an increased ETN dose or an early switch to another biologic could be proposed. It would be interesting to investigate whether an earlier ETN measurement (e.g., at 1 month) could also predict this response.
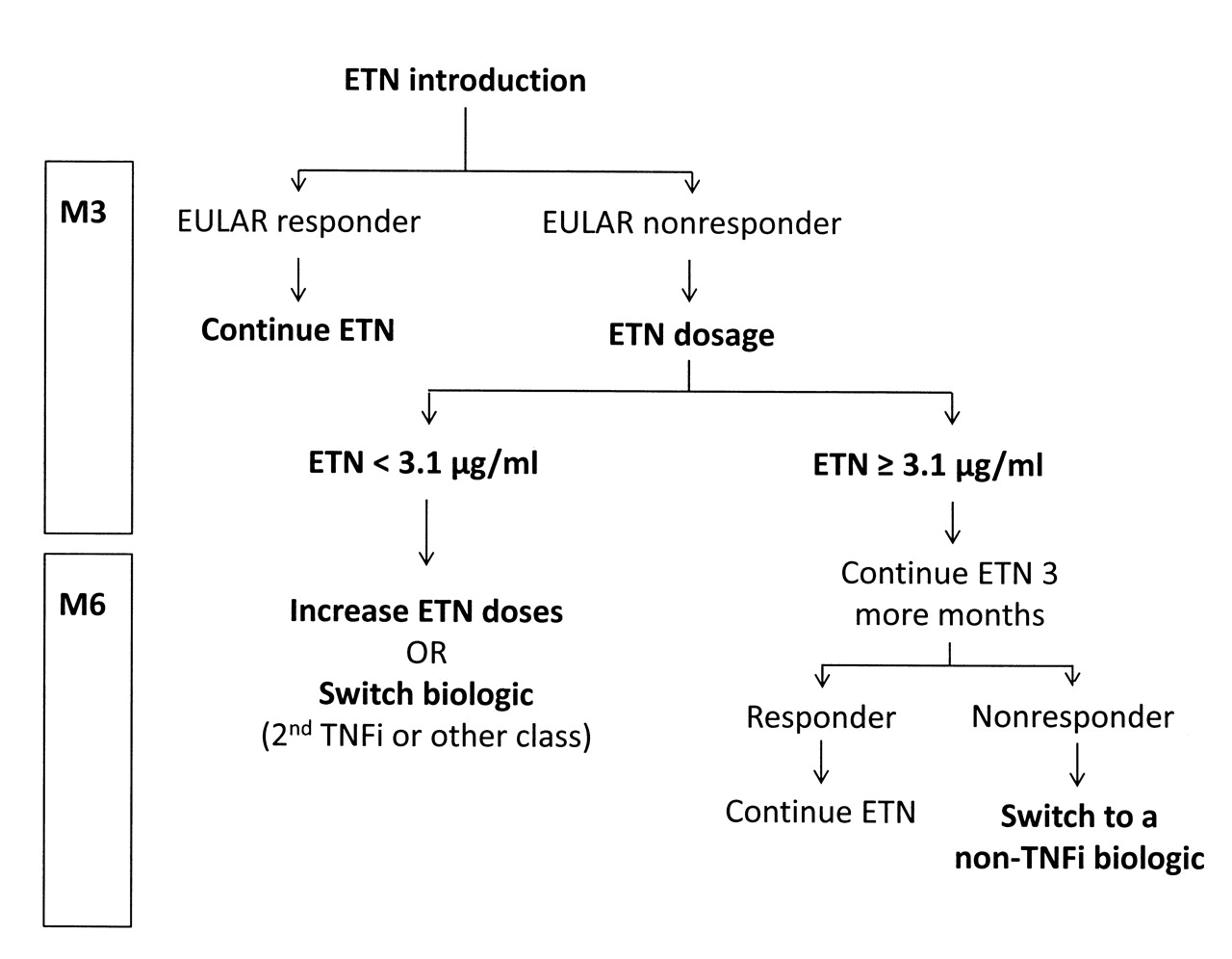
Proposed decision algorithm for the management of RA with etanercept (ETN). TNFi: TNF inhibitor; EULAR: European League Against Rheumatism.
The merit of increased dosing of biologic therapeutics is questionable and requires more studies. Increased dosing efficacy has been discussed for infliximab, for example. Some investigators found a significant improvement in response for patients with increased infliximab dose13,14; but others did not (n = 115)15. For adalimumab, the PREMIER study found no advantage of increasing the dose16. Bartelds, et al recently found that with adalimumab, about 80% of patients who had not achieved minimal disease activity before increasing the dosage did not achieve minimal disease activity after an increase of the dosage11. The situation with ETN is slightly different because the low levels of circulating drug are probably not due to the presence of ADAb. Experiences with increased dosing with ETN have rarely been published15, but the efficacy seems to be small or absent. A significant improvement in disease activity after dosage increase was found at 3 months (p = 0.03) but not at 6 months15. Moreover, an important consequence of dosage increase is the higher cost of therapy. Because many biologics are now available for RA, cost-effectiveness probably does not favor dosage increase. The situation may be different for patients with spondylitis, for whom treatment options are more limited. For patients with high ETN concentrations, the potential of decreased ETN doses also deserves investigation. It would be especially relevant in clinical trials evaluating strategies of decreased anti-TNF drugs for patients in remission. It would be of particular interest to observe whether patients without relapse although they decreased their ETN dosage were those with high ETN levels at inclusion.
Our results could also affect the choice of the next biologic for therapy. The definition of a primary nonresponder is based on disease activity at 3 or 6 months. For patients receiving monoclonal antibodies, Bartelds, et al proposed adding patients with an optimal concentration of anti-TNF antibodies and no ADAb to the definition of primary nonresponders11. These patients may benefit more from switching to another biologic instead of a second TNF inhibitor. This recommendation could also apply to patients receiving ETN: in patients who do not respond to ETN despite optimal drug concentrations, RA is likely not sensitive to TNF-α inhibition, and another class of biologic would be more effective than another TNF inhibitor (Figure 4).
In our study, 2 patients had undetectable ETN concentrations because of temporary interruption of therapy. Although not the case here, monitoring drug concentrations can help to detect patients with poor compliance, and consequently to improve treatment outcomes by improving compliance.
The main limitation of this study is the small number of patients, which did not allow drawing firm conclusions.
ETN concentration at 3 months helps to predict response to treatment at 6 months in patients with RA. This is significant because early detection of inefficient therapy may allow an earlier change to more efficacious treatment, and as well may optimize drug expenses. Our results need to be confirmed with a larger cohort and the thresholds further studied. Validation studies are needed to confirm these findings for effective decision making in rheumatology.
Acknowledgment
We thank Guillaume Noguier, Biomedical Diagnostics, for technical assistance.
Footnotes
-
Supported by unrestricted education grants from Pfizer (France) and the French Society of Rheumatology. Dr. Combe and Dr. Morel received < €10,000 in honoraria from Pfizer Laboratory for consulting as investigators in clinical trials.
- Accepted for publication April 30, 2012.








{kind=link}
{kind=link}
{kind=link}
{kind=link}