

Abstract
Objective. A prospective observational study of mycophenolate mofetil (MMF) treatment in patients with diffuse progressive cutaneous systemic sclerosis (SSc) of recent onset.
Methods. Twenty-five previously untreated consecutive patients with recent-onset (< 24 mo) diffuse progressive cutaneous SSc received MMF as the only disease-modifying therapy. Modified Rodnan skin score (mRSS) and affected body surface area (BSA) were compared from initiation of MMF to study end. Pulmonary function tests performed at the same institution before therapy and at study end were available in 15 patients. Histopathology and real-time PCR assessment of fibrosis-related gene expression were performed before and after treatment in skin biopsies from 3 patients.
Results. At 18.2 ± 8.73 months of MMF therapy (median 2000 mg/day) the mRSS decreased from 24.56 ± 8.62 to 14.52 ± 10.9 (p = 0.0004) and the affected BSA from 36% ± 16% to 14% ± 13.3% (p = 0.00001). Pulmonary function tests remained stable from initiation of MMF to the end of the study. Skin histopathology showed a remarkable reduction in accumulation of fibrotic tissue. Real-time PCR of skin biopsies demonstrated a marked decrease in expression of fibrosis-related genes.
Conclusion. Patients with diffuse progressive cutaneous SSc of recent onset treated with MMF experienced marked improvement in skin involvement and stabilization of pulmonary function. Skin biopsies from 3 patients demonstrated histopathological improvement and decreased expression of fibrosis-related genes.
Systemic sclerosis (SSc) is a heterogeneous autoimmune disease characterized by increased collagen deposition in skin and multiple internal organs, prominent vascular and endothelial abnormalities, and humoral and cellular immune dysregulation1,2,3. The introduction of target organ-specific therapies has substantially decreased morbidity and mortality of SSc4. In contrast, most studies of potential disease-modifying agents have shown negative results and currently there is no generally accepted SSc disease-modifying therapy.
A major challenge for the evaluation of effectiveness of therapeutic interventions in SSc is the heterogeneity and variable course of the disease. To mitigate the effects of variability of the course of SSc and following the paradigm that early intervention is crucial for halting fibrosis, most recent studies selected patients with recent onset of disease5,6,7,8,9. Disease of recent onset has been defined in different ways in various studies, although a cutoff point of 18–24 months from the appearance of clinically detectable skin induration is generally accepted. Further, patients should have substantial skin involvement at initiation of treatment to allow detection of improvement employing the outcome measurement tools currently available.
Mycophenolate mofetil (MMF) is an immunosuppressant agent that inhibits proliferative responses of T and B lymphocytes as well as antibody production by B lymphocytes. It is indicated for prevention of organ rejection following allogeneic cardiac, hepatic, and renal transplants10. It is also used for induction and maintenance therapy of lupus nephritis11,12. Further, there is evidence that MMF can inhibit fibrosis by acting either directly on fibroblasts13 or by inhibiting fibroblast proliferation14, and by reducing tissue accumulation of activated myofibroblasts15.
Studies including a recent assessment of 98 patients have described encouraging results of MMF treatment for SSc16,17,18,19,20. In contrast, a recent observational trial failed to show significant differences between 4 different therapeutic approaches, 3 of which included MMF21.
We describe a prospective observational study of MMF for the treatment of SSc in patients with recent onset of progressive diffuse cutaneous involvement. In contrast with other studies16,17,18,19,20, patients included in our study had not received any previous immunosuppressive, immunomodulating, or antifibrotic therapy, and none had received any other disease-modifying therapy during the study.
MATERIALS AND METHODS
Patient cohort
From December 2006 to December 2009, every new patient with diffuse and rapidly progressive SSc of recent onset evaluated at our institution was offered treatment with MMF as disease-modifying monotherapy. Only patients with < 2 years of disease and modified Rodnan skin score (mRSS) > 12 points who had not received any previous immunosuppressive, immunomodulatory, or antifibrotic therapy were included. Despite the consecutive enrollment design, not all qualifying patients received MMF, for diverse reasons including most commonly the denial of insurance reimbursement.
All patients received MMF 500 mg twice a day for 3 to 4 weeks and then the dose was escalated to 1–1.5 g twice a day. Other concomitant medications included calcium channel blockers, angiotensin-converting enzyme inhibitors, proton pump inhibitors, statins, and low-dose aspirin. The effects of MMF on the extent and severity of skin involvement using the mRSS and an estimate of extent of affected body surface area (BSA) were assessed as described22. The effects of MMF on SSc severity using some of the categories of Medsger’s severity scale23 were also examined.
The inclusion criteria were (1) time from onset of clinically detectable skin induration to initiation of MMF < 24 months; (2) diffuse skin involvement at initiation of MMF affecting the trunk and/or arms and legs proximally to the elbows and/or knees with mRSS > 12; (3) no previous treatment with MMF, D-penicillamine, bovine collagen, cyclophosphamide, or any other putative SSc disease-modifying drug or intervention; and (4) presence of progressive skin involvement based on information provided by the referring rheumatologist or by sequential examination at our center.
The exclusion criteria were (1) skin involvement confined to face or acral regions of the body (limited cutaneous SSc); (2) eosinophilic fasciitis, nephrogenic systemic fibrosis, or other SSc-like diseases; (3) mixed connective tissue disease and overlap syndromes; (4) prior or current therapy with any other immunosuppressant or antifibrotic agent; and (5) poor compliance to medications or followup.
Study entry was the initiation of MMF treatment and end of study was the last recorded visit. For data analysis, only patients who were followed for at least 6 months were included.
Assessment of MMF effects on cutaneous and visceral involvement
The extent and severity of skin involvement was assessed by the mRSS, and the extent of affected BSA was assessed by the rule of nines employing a burns-victim diagram as described22. These variables were recorded every 3–6 months during treatment followup. Pulmonary function tests including total lung capacity (TLC) and DLCO were monitored every 6–12 months during the study. Although chest computerized tomography (CT) is part of the evaluation and management for all patients with SSc at our center, CT findings were not systematically followed up. Percentages and means ± SD were used to describe demographic data. A paired 2-tail Student t test was used to compare data during the study period. Because skin involvement continues to increase in extent and severity for a variable length of time following initiation of therapy in patients with diffuse SSc of recent onset, comparisons of skin involvement were performed between the initial versus final scores and between the maximal (peak) versus final scores.
Effects of MMF on skin histopathology and fibrosis-related gene expression
Pre- and post-treatment skin biopsies were performed in 3 patients with their informed consent. Punch biopsy samples were obtained from affected skin in the dorsum of the forearm. The post-treatment samples were from an area removed about 5 mm from the initial skin biopsy. Histopathology assessment was performed in H&E-stained skin biopsy samples. Total RNA was extracted from all the biopsies using the RNeasy Fibrous Tissue Kit (Qiagen, Valencia, CA, USA). Each sample was retro-transcribed using SuperScript II reverse transcriptase (Invitrogen, Carlsbad, CA, USA) and real-time quantitative polymerase chain reaction (rt-PCR) was performed for the expression of COL1A1, COL1A2, COL4A1, COL14A1, CTGF, FN1, ACTA2, and TGFB1. Sequence-specific primers (Table 1) were designed using PrimerQuest (Integrated DNA Technologies, Coralville, IA, USA). Rt-PCR was performed using SYBR-green with an ABI Prism 7900 system (Applied Biosystems, Carlsbad, CA, USA). The expression level of messenger RNA was normalized by 18s ribosomal RNA.
Sequence of primers used for real-time polymerase chain reaction.
Statistical analysis
Statistical analysis was performed using a paired Student t test. A p value < 0.05 was considered statistically significant. Statistical analyses were performed using Excel and GraphPad Prism programs.
RESULTS
Demographics
There were 35 patients with progressive SSc who fulfilled the classification criteria for SSc of the American College of Rheumatology24 and the criteria of LeRoy, et al25 for the clinical subset of diffuse cutaneous SSc. All patients had disease of recent onset and had not received any prior immunomodulatory or immunosuppressive therapy or any putative antifibrotic agent or intervention. Twenty-five patients met the inclusion and exclusion criteria and were followed at our institution for at least 6 months. The mean ± SD age at initiation of treatment was 48.6 ± 14.5 years. The majority of the patients were white (76%) with a smaller proportion of African Americans (12%). The autoantibody profile indicated that 100% had a positive antinuclear antibody (ANA) by immunofluorescence, and 36% (9 patients) harbored anti-Scl-70 antibodies. The remaining patients were ANA-positive but Scl-70 and anticentromere antibody-negative. Analyses for RNA polymerase I/III or other SSc-specific antibodies were not performed in all patients. The average duration of therapy was 18.2 ± 8.73 months, and 18 out of 25 (72%) were treated for longer than 1 year. The average dose of MMF was 2.02 g/day. Only 3 patients had received < 2 g/day because of gastrointestinal (GI) side effects.
Clinical assessment of skin involvement and pulmonary function
Clinically detectable skin induration was first noted at a mean 14.1 ± 7.3 months before study entry. At the initiation of therapy the mRSS was 24.56 ± 8.62 units and the affected BSA was 36% ± 16%. In the majority of patients a worsening of mRSS and extent of affected BSA was noted following entry into the study, reaching a peak 3–6 months after initiation of MMF therapy. The average time from the first detectable skin involvement to the maximal involvement (considered as the maximal mRSS) was 20.1 months and the interval between initiation of treatment to peak mRSS was 6.4 months. Maximal mean mRSS was 27.36 ± 9.71 points and BSA 38% ± 15.4%. The increase in mRSS from the initiation of therapy to maximal involvement was statistically significant (p = 0.0065). Although the increase in BSA value displayed a similar trend it did not reach statistical significance (p = 0.069). A significant reduction of the mRSS and affected BSA was noted from the beginning of therapy to the end of the study. The mRSS decreased from 24.56 ± 8.62 at entry to 14.52 ± 10.9 (p = 0.004) and affected BSA decreased from 36% ± 16% at entry to 14% ± 13.3% (p = 0.00001). A more dramatic change was observed when the peak involvement was compared with involvement at the end of the study. The values observed were 27.36 ± 9.7 vs 14.52 ± 10.9 (p = 2.5 × 10−6) for mRSS and 38% ± 15.4% vs 14% ± 13.3% (p = 9.2 × 10−7) for BSA.
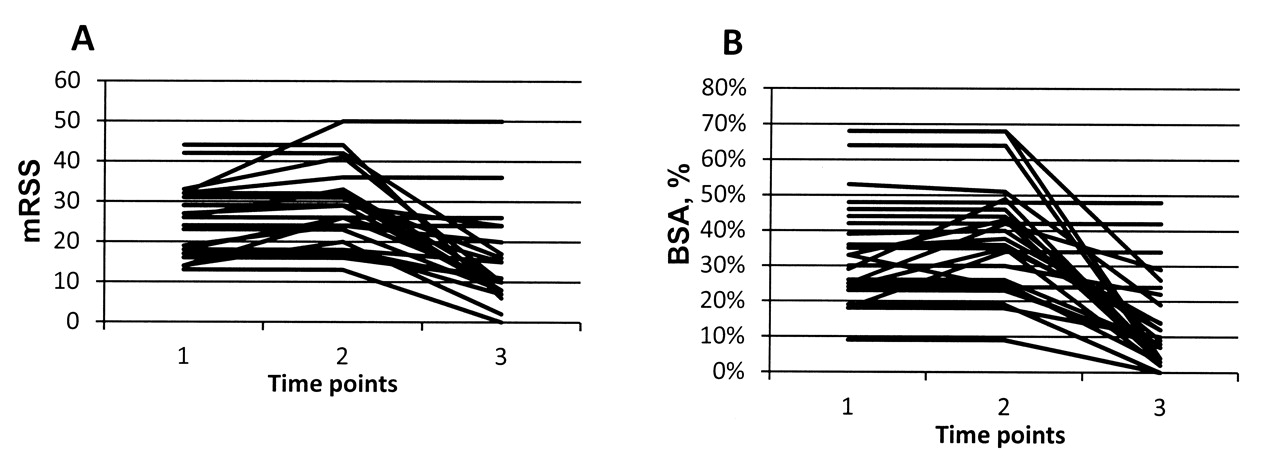
Figure 1 shows mRSS values and extent of affected BSA at initiation of treatment (point 1), at peak involvement (point 2), and at last followup (point 3). The changes in affected BSA in 3 patients from whom skin biopsies were obtained before initiation of MMF therapy and at the end of the study are pictured in Figure 2. The modified Medsger Severity Score was assessed in all patients; however, the values represent an underestimate of the severity of the disease since not all patients with GI symptoms were examined by endoscopy or barium-swallow, and muscle involvement was not routinely evaluated. Scores for organ involvement measured by the Medsger Severity Score at initiation of treatment compared with scores at the study end did not reach statistical significance, with the exception of the skin index, which showed a significant reduction, 2.2 ± 0.71 versus 1.52 ± 0.77 (p = 0.0003).

A. Assessment of modified Rodnan skin score (mRSS) was performed at initiation of treatment (point 1), at peak of skin involvement (point 2), and at last followup (point 3). B. Extent of affected body surface area (BSA) at initiation of treatment (point 1), at peak involvement (point 2), and at last followup (point 3).
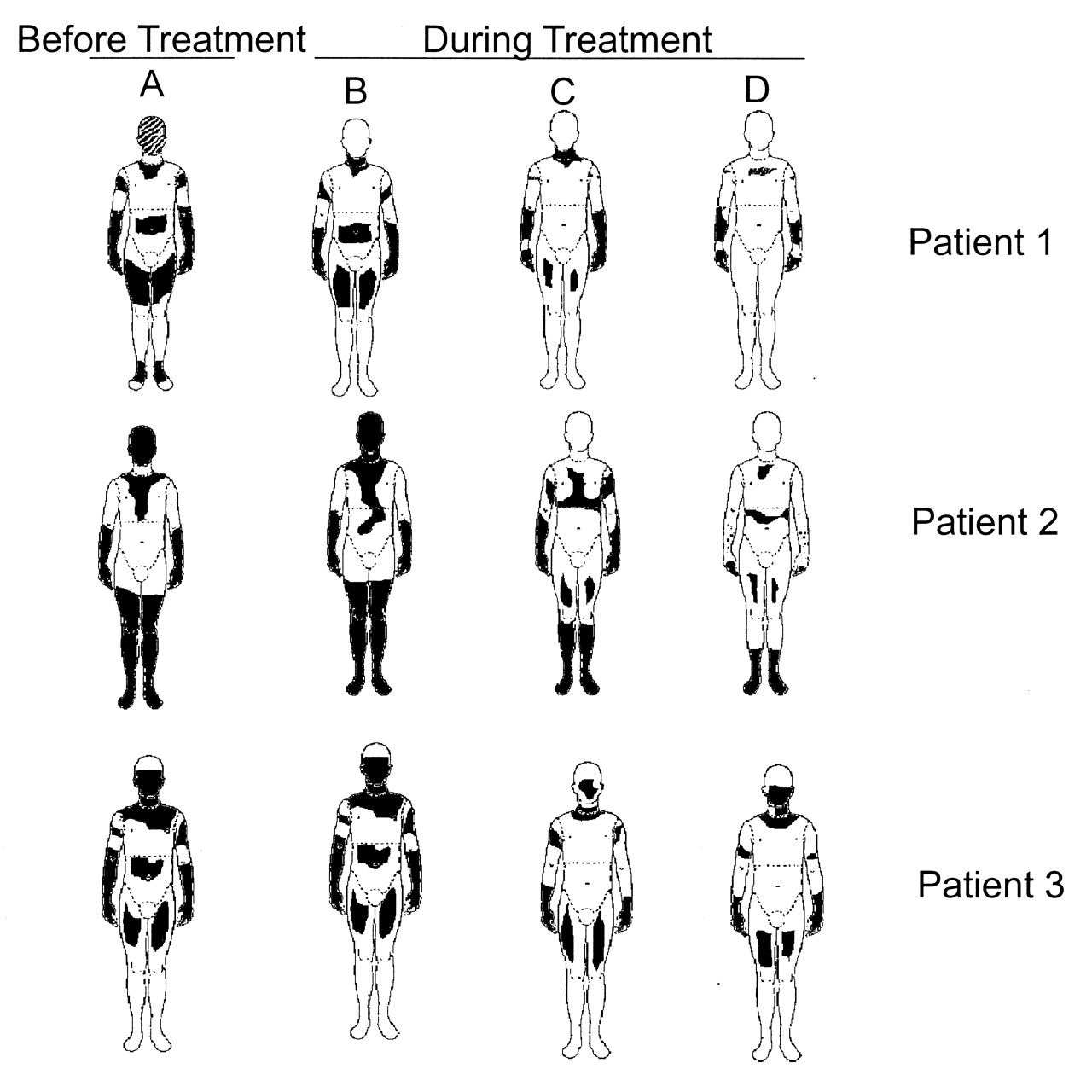
Assessment of total body surface area (BSA) involvement in 3 patients who had skin biopsies before and after mycophenolate mofetil (MMF) treatment. A. BSA at the initiation of MMF therapy. B–D. BSA at serial followup evaluations (roughly every 3 months).
The results of pulmonary function tests were analyzed in 15/25 patients who had pre- and post-treatment tests performed at the same institution and were, therefore, consistent in methodology and equipment used. The results in these patients showed that TLC was 89.47% ± 16.61% of the level predicted at study entry compared with 85.33% ± 17.34% at study end (p = 0.13). In this subgroup of 15/25 patients only 3 patients showed a decrease in their TLC values > 10%. The results for DLCO were 69.0% ± 17.51% of the level predicted at study entry compared to 70.47% ± 18.84% at study end (p = 0.45).
Tolerability and adverse events
All patients tolerated MMF treatment well and in no case was MMF discontinued owing to intolerance or side effects, although in 3 of the 25 patients the dose was reduced to 1–1.5 g/day because of GI side effects. Ten patients developed at least 1 adverse event during MMF treatment. A total of 13 events were recorded. The most common events were diarrhea (n = 3) and upper respiratory infections (3), followed by lymphopenia (2) and urinary tract infection (2). One of these 10 patients required a dose adjustment because of leukopenia. One study patient died at 18 months after entry; the cause of death was a severe and rapidly progressive dilated cardiomyopathy of unknown etiology. Although it is very unlikely that this event was related to MMF treatment, the possibility that it represented an abrupt deterioration of SSc cardiac involvement or a viral infection possibly related to immunosuppression cannot be conclusively established. However, at her last evaluation following 9 months of MMF therapy and about 10 months before death there was a clear reduction in both mRSS and total affected BSA, making it less likely that death was related to SSc.
Skin histopathological analysis and assessment of fibrosis-related gene expression
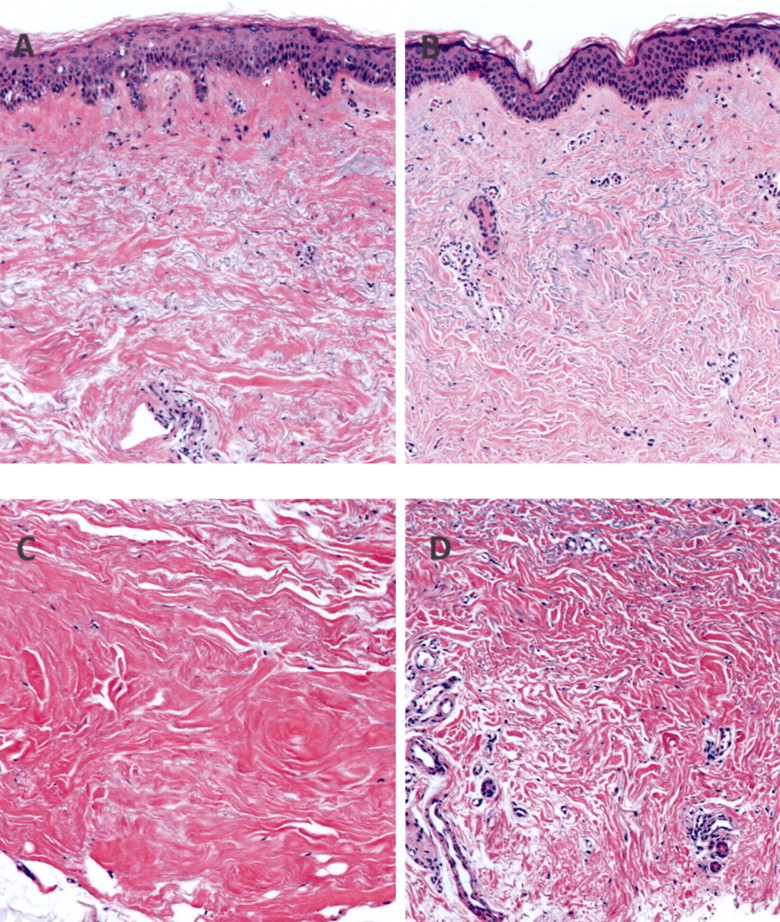
Histopathological examination and analysis of fibrosis-related gene expression were performed in pre- and post-treatment skin biopsies obtained from 3 patients. As illustrated in Figure 3, H&E staining showed a remarkable decrease in the abundance and thickness of collagen bundles and in their compact appearance in the dermis. Similar findings were observed in skin biopsies stained with Masson’s trichrome (not shown). There was also very noticeable reappearance of hair follicles and sweat and sebaceous glands in the post-treatment biopsies. Analysis of relative gene expression by rt-PCR demonstrated a marked decrease in the relative expression of numerous fibrosis-related genes including COL1A1, COL1A2, COL 4A1, COL 11A1 COL 14A1, CTGF, FN1, ACTA2, and TGFB1 (Figure 4).

Histopathology of pre-treatment (A and C) and post-treatment (B and D) H&E-stained skin biopsies (images are 100× original magnification). A and B show epidermis and upper dermis; C and D show lower dermis. Note remarkable decrease in the thickness and compact appearance of the collagen bundles, as well as the repopulation of dermal structures following MMF treatment.
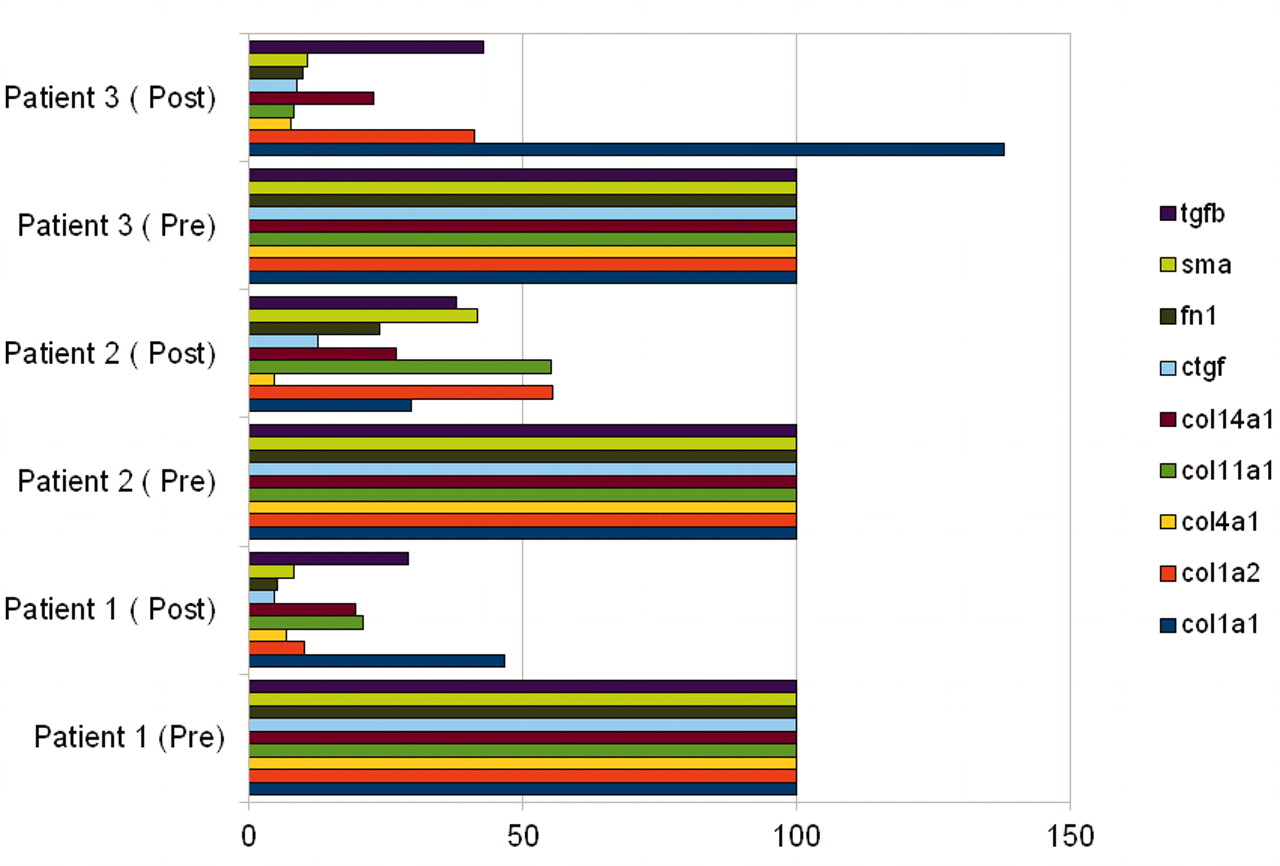
Relative change in real-time quantitative polymerase chain reaction fibrosis-related gene expression from beginning to end of treatment in skin biopsy samples from 3 patients. Shown are measurement of various collagen genes (COL1A1, COL1A2, COL4A1, COL11A1, COL14A1), connective tissue growth factor (CTGF), fibronectin 1 (FN-1), α-smooth muscle actin (SMA), and transforming growth factor-ß (TGFB). Horizontal scale shows expression levels as percentage; pre-treatment levels were normalized to 100%.
DISCUSSION
Mycophenolate mofetil, through its biologically active molecule mycophenolic acid, exerts potent antiproliferative properties resulting from the reversible inhibition of inosine monophosphate dehydrogenase (IMPDH). Given the higher sensitivity of the lymphocyte IMPDH isoform, MMF exerts its effects by causing preferential lymphocyte suppression. On the other hand, recent studies have shown that MMF is also able to decrease fibroblast proliferation, an effect that appears to be mediated mainly by IMPDH-dependent pathways, although IMPDH-independent pathways can also play a role14,15. It also has been shown that MMF is capable of direct inhibition of collagen production13.
The degree of improvement of mRSS we observed correlates well with results from Derk, et al19 and Le, et al20, who found reduction of 14.1 and 7.6 points, respectively, in the mRSS of patients treated with MMF. Given the heterogeneous SSc course, the > 10-point mRSS improvement and the 23% reduction in affected BSA we observed are likely clinically significant for this population of previously untreated patients with SSc of recent onset with diffuse cutaneous involvement and usually progressive clinical course. Further, these results are also superior to our previously published data on D-penicillamine in a similar population22. These results are also superior to the spontaneous reduction in mRSS observed in the placebo control group (−4.6) and in the relaxin-treated group (−4.4) in a study describing the results of a 24-week randomized controlled trial of human recombinant relaxin in a population of patients with SSc similar to the one we studied here26. It is also superior to the −3-point reduction at 15 months in either placebo or treatment group in patients with early-phase SSc who entered the bovine type I collagen randomized controlled trial27.
The clinical improvement we observed correlated well with a remarkable decrease in histopathological fibrosis and reappearance of dermal hair follicles and sebaceous and sweat glands, as well as with a marked reduction in the expression of numerous fibrosis-related genes in samples from 3 patients in whom skin biopsies were obtained before and after therapy. Of importance was the observation that MMF treatment prevented deterioration of pulmonary function in this population with diffuse SSc of recent onset, in whom substantial and significant deterioration of lung function is highly likely. However, it should be emphasized that the cohort we studied had only a mild baseline decrease in TLC at study entry, a variable that may have contributed to slow progression of deterioration of pulmonary function, as described by Plastiras, et al28. The stabilization of lung involvement as assessed by comparison of pulmonary function tests from initiation of MMF treatment to the end of the study is similar to results recently described by Simeón-Aznar, et al in 14 consecutive patients with SSc who were treated with MMF 1.5 g for 12 months29.
Although the number of patients we studied is not large, there are several strengths to our study, including the prospective observational design and the strict criteria for defining the study population requiring that only patients with very early (< 2 years) and progressive skin disease be included. This is in contrast with populations with much longer duration of skin disease in the majority of other studies of SSc disease-modifying interventions. Another strength of our study is that all patients were naive to any immunosuppressants or antifibrotic treatment and received MMF as the only disease-modifying therapy for the duration of the study.
The selection of patients with early disease was required in order to mitigate the effects of the variable course of SSc and to address the paradigm that early intervention is crucial for effective treatment in SSc and other fibrotic diseases. On the other hand, given the relatively low sensitivity of the current tools for disease assessment, the inclusion of patients with moderate to severe disease was important to demonstrate differences induced by the therapeutic intervention.
From the safety perspective, MMF-related adverse events were mild and well tolerated and only 3 patients required a dose adjustment. Discontinuation of MMF was not necessary in any patient. In contrast to the benign pattern of MMF side effects, other options for SSc disease modification, including cyclophosphamide and bone marrow transplant, carry substantial and even fatal potential side effects30,31. Further, the frequency and severity of adverse events we observed are not greater than those found in patients with other autoimmune diseases or in renal transplant patients treated with MMF.
We are aware that owing to the non-placebo-controlled design of the study it is not possible to draw definitive conclusions regarding the efficacy of MMF in modifying disease course in SSc. However, the remarkable degree of clinical improvement observed in this cohort with progressive SSc of recent onset, which was strongly corroborated by histopathological and gene expression studies, is unlikely to be explained only by the natural evolution of the disease, particularly in this group of patients with very early and progressive disease. Given the benign safety profile, our findings suggest that therapy with MMF is safe and effective for SSc patients with progressive diffuse cutaneous disease of recent onset.
Given the major limitations and substantial challenges in the study of potential disease-modifying treatment for SSc, prospectively designed double-blind studies will be needed to identify effective therapeutic interventions for this often devastating disease.
Acknowledgment
We gratefully acknowledge the technical assistance of Megan Musick in the gene expression studies. The excellent assistance of Melissa Bateman in the preparation of the manuscript is also gratefully acknowledged.
Footnotes
-
Supported in part by NIH Grant AM19616 to Sergio A. Jimenez.
- Accepted for publication January 20, 2012.








{kind=link}
{kind=link}
{kind=link}
{kind=link}