

Abstract
Objective. To evaluate the effect of golimumab on physical function, general health, and fatigue in patients with active rheumatoid arthritis (RA) despite methotrexate (MTX) therapy.
Methods. In the multicenter, randomized, placebo-controlled GO-FORWARD study, 444 adults with active RA despite MTX received subcutaneous placebo + MTX (crossover to golimumab 50 mg at Week 24), golimumab 100 mg + placebo, golimumab 50 mg + MTX, or golimumab 100 mg + MTX every 4 weeks. Physical function and general health were assessed using the Health Assessment Questionnaire-Disability Index (HAQ-DI) and Physical and Mental Component Summary (PCS, MCS) scores of the Medical Outcomes Study Short Form-36 questionnaire (SF-36), respectively, through Week 52. Fatigue was measured through Week 24 using the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-Fatigue) questionnaire.
Results. Mean improvements from baseline in HAQ-DI, SF-36 PCS, and FACIT-Fatigue scores (Weeks 14 and 24) were significantly greater for golimumab 50 mg + MTX and 100 mg + MTX versus placebo + MTX. Significantly greater proportions of patients treated with golimumab + MTX achieved clinically meaningful improvements from baseline to Weeks 14 and 24 in HAQ-DI, PCS, and FACIT-Fatigue scores. Mean improvements in SF-36 PCS (Week 14), MCS (Week 24), and FACIT-Fatigue (Weeks 14 and 24) scores were significantly greater for golimumab 100 mg + placebo versus placebo + MTX. Mean improvements from baseline in HAQ-DI, SF-36 PCS, and MCS scores through Week 24 were sustained through Week 52.
Conclusion. Patients with active RA despite MTX had significant improvement in physical function, general health, and fatigue following golimumab + MTX therapy; improvements in physical function and general health were maintained through Week 52. (Clinical Trials Registration NCT00264550)
Rheumatoid arthritis (RA) is a systemic immune-mediated inflammatory disorder with an unknown etiology manifesting predominantly as inflammation of the joints. The main presenting symptoms of joint pain, stiffness, and swelling and quite often joint destruction result in impaired physical function and quality of life1,2,3. RA is a systemic disorder and can include fever, malaise, and pulmonary, ocular, kidney and cardiovascular disease4,5. In addition, severe fatigue can occur in a substantial number of patients with RA and can be predicted by general health and the degree of disability6.
Several clinical studies have demonstrated that treatment with the anti-tumor necrosis factor (TNF) agents adalimumab, certolizumab pegol, etanercept, and infliximab improves the manifestations of RA, supporting the concept that TNF plays a key role in the pathogenesis of RA7,8,9,10,11,12,13,14. These anti-TNF agents have also proven effective in improving physical function, general health, and fatigue in patients with RA3 and psoriatic arthritis15.
Golimumab is a human anti-TNF monoclonal antibody that binds with high affinity and specificity to soluble and transmembrane TNF-α. Golimumab is approved in several countries for the treatment of RA, although recommended doses vary. In the United States, golimumab 50 mg administered subcutaneously with concomitant oral methotrexate (MTX) is approved for patients with RA16; however, the European Medicines Agency recommends a 50-mg dose for RA patients with an increase to 100 mg allowed in patients weighing more than 100 kg who have an inadequate response to treatment17.
We previously reported on efficacy and safety of golimumab through Weeks 24 and 52 of the GO-FORWARD trial, a phase III, multicenter, randomized, double-blind, placebo-controlled trial in 444 patients with active RA despite MTX therapy18,19. Patients treated with golimumab 50 mg or 100 mg plus MTX had significant improvements in the signs and symptoms of active RA at Week 2419, and these improvements were maintained through Week 5218. In addition, golimumab was generally well tolerated, and safety results at Week 52 were similar to those at Week 24. We now report 1-year findings from the GO-FORWARD trial related to patient physical function, general health, and fatigue.
MATERIALS AND METHODS
Patients
Patient inclusion and exclusion criteria have been described19. Briefly, patients were at least 18 years of age and had a diagnosis of RA according to the revised 1987 criteria of the American College of Rheumatology20 for at least 3 months before screening. In addition, patients had active RA, despite previous MTX therapy, which was defined as 4 or more swollen joints (out of 66 total) and 4 or more tender joints (out of 68 total) and at least 2 of the following: screening C-reactive protein level of at least 1.5 mg/dl or screening/baseline erythrocyte sedimentation rate by Westergren method of at least 28 mm in the first hour, morning stiffness of at least 30 min at screening and baseline, bone erosion as observed by radiograph and/or magnetic resonance imaging prior to the first administration of study agent, or positive for anticyclic citrullinated peptide antibodies or rheumatoid factor at screening. Patients must have received a stable dose of MTX (≥ 15 mg/wk but not > 25 mg/wk) during the 4-week period immediately preceding screening and to have tolerated a dose ≥ 15 mg/week for at least 3 months. Institutional review board or ethics committee approval and patient’s written informed consent were obtained prior to study procedures (Clinical Trials Registration NCT00264550).
Study design
In this multicenter, double-blind, placebo-controlled trial, 444 patients were randomly assigned (3:3:2:2) to receive placebo injections plus MTX with crossover to golimumab 50 mg plus MTX at Week 24, golimumab 100 mg injections plus placebo capsules, golimumab 50 mg injections plus MTX, or golimumab 100 mg injections plus MTX. Injections were administered subcutaneously every 4 weeks through Week 48. At Week 16, patients who had < 20% improvement from baseline in both total tender and total swollen joint counts entered early escape in a double-blind fashion. Patients who originally received placebo plus MTX switched to golimumab 50 mg plus MTX, those who originally received golimumab 100 mg plus placebo switched to golimumab 100 mg plus MTX, and those who originally received golimumab 50 mg plus MTX switched to golimumab 100 mg plus MTX. Patients who were originally assigned to receive golimumab 100 mg plus MTX did not have any adjustment in treatment.
Evaluations
Patient functional status was assessed using the Health Assessment Questionnaire-Disability Index (HAQ-DI)21. This 20-question instrument assesses the degree of difficulty a person has in accomplishing tasks in 8 functional areas (dressing, arising, eating, walking, hygiene, reaching, gripping, and activities of daily living). Responses in each functional area are scored from 0, indicating no difficulty, to 3, indicating inability to perform a task in that area. A HAQ-DI score ≤ 0.5 indicates normal physical function. An improvement in HAQ-DI score ≥ 0.22 is considered to be clinically meaningful22; however, because the HAQ-DI score can only increase or decrease in 0.125 increments, the cutoff of a change ≥ 0.25 was used in this analysis.
The health status of patients was assessed using the Medical Outcomes Study Short Form-36 questionnaire (SF-36), an instrument comprising 8 multiitem scales: limitations in physical functioning because of health problems, limitations in usual role activities because of physical health problems, bodily pain, general mental health (psychological distress and well-being), limitations in usual role activities because of personal or emotional problems, limitations in social functioning because of physical or mental health problems, vitality (energy and fatigue), and general health perception. In addition, physical and mental component summary (PCS, MCS) scores of the SF-36 are reported. The concepts measured by the SF-36 are not specific to any age, disease, or treatment group, allowing comparison of the relative burden of different diseases and the relative benefit of different treatments23. An improvement ≥ 5 points in PCS or MCS score was considered clinically meaningful.
Fatigue was assessed with the Functional Assessment of Chronic Illness Therapy-Fatigue (FACIT-Fatigue) questionnaire, which assesses self-reported tiredness, weakness, and difficulty conducting usual activities because of fatigue24. The total FACIT-Fatigue score ranges from 0 to 52, a higher score indicating less fatigue. The FACIT-Fatigue questionnaire has been used in clinical trials of patients with RA and has demonstrated sensitivity to change in these patients25. A clinically meaningful improvement in FACIT-Fatigue score for patients with RA has been determined to be a 3- to 4-point change26.
Statistical analyses
Descriptive statistics including means, counts, and percentages are reported. Treatment group comparisons were made at Weeks 14 and 24 using ANOVA on the van der Waerden normal scores. Clinically meaningful improvements in HAQ-DI, PCS, MCS, and FACIT-Fatigue scores were compared between the placebo plus MTX group and the golimumab groups using a chi-square test. In the Week 52 analyses, the golimumab plus MTX groups were combined for comparison with the placebo (golimumab crossover) plus MTX group, and patients were categorized according to their originally assigned treatment group. In addition, patients in the placebo plus MTX group who discontinued the study before receiving any golimumab doses were not included in the Week 52 analysis.
Spearman’s correlation was used to evaluate the relationship between fatigue and physical function. All analyses were based on an intent-to-treat principle, and all statistical testing was performed 2-sided at a significance level of 0.05. A last-observation-carried-forward procedure was used for imputation of missing data and for patients who entered the early escape procedure.
RESULTS
Patient disposition and baseline characteristics
Patient baseline characteristics as described19 were well balanced across the treatment groups. Mean baseline HAQ-DI scores, which ranged from 1.3 to 1.4 across the treatment groups, indicated moderate functional impairment (Table 1). The mean baseline PCS and MCS scores of the SF-36 ranged from 29.9 to 31.6 and 43.2 to 44.1, respectively, across the treatment groups. Mean baseline FACIT-Fatigue scores ranged from 26.6 to 28.7 (out of 52) across the treatment groups and indicated a substantial amount of patient fatigue. Patient disposition up to Week 52 has been described18.
Baseline patient characteristics.
Physical function
Treatment with golimumab 50 mg or 100 mg plus MTX resulted in statistically significant and clinically meaningful improvements in HAQ-DI scores. The mean (± SD) improvement in HAQ-DI score at Week 14 was significantly greater in the golimumab 50 mg plus MTX group (0.42 ± 0.50) and the golimumab 100 mg plus MTX group (0.41 ± 0.46) than in the placebo plus MTX group (0.16 ± 0.49; p < 0.001 for both comparisons; Table 2). Similar results were observed at Week 24, with patients in the golimumab 50 mg plus MTX (0.47 ± 0.55) and golimumab 100 mg plus MTX (0.45 ± 0.52) groups having significantly greater mean improvement in HAQ-DI score compared with those who received placebo plus MTX (0.13 ± 0.58; p < 0.001 for both comparisons). Mean improvements from baseline in HAQ-DI scores through Week 24 were sustained or enhanced through Week 52 (Table 3).
Improvements in HAQ-DI, SF-36, and FACIT-Fatigue scores at Weeks 14 and 24.
Week 52 results for HAQ-DI and SF-36 scores.
The proportion of patients achieving at least a 0.25-unit improvement from baseline to Week 14 in HAQ-DI score was significantly greater in the golimumab plus MTX groups [50 mg: 67.8% (59/87); 100 mg: 71.4% (60/84)] than in the placebo plus MTX group [42.6% (55/129); p < 0.001 for both; Figure 1]. Similarly, at Week 24 significantly greater proportions of patients receiving golimumab 50 mg plus MTX [68.2% (60/88)] or golimumab 100 mg plus MTX [72.1% (62/86)] had a clinically meaningful improvement in HAQ-DI score compared with those receiving placebo plus MTX [38.6% (49/127); p < 0.001 for both; Figure 2).
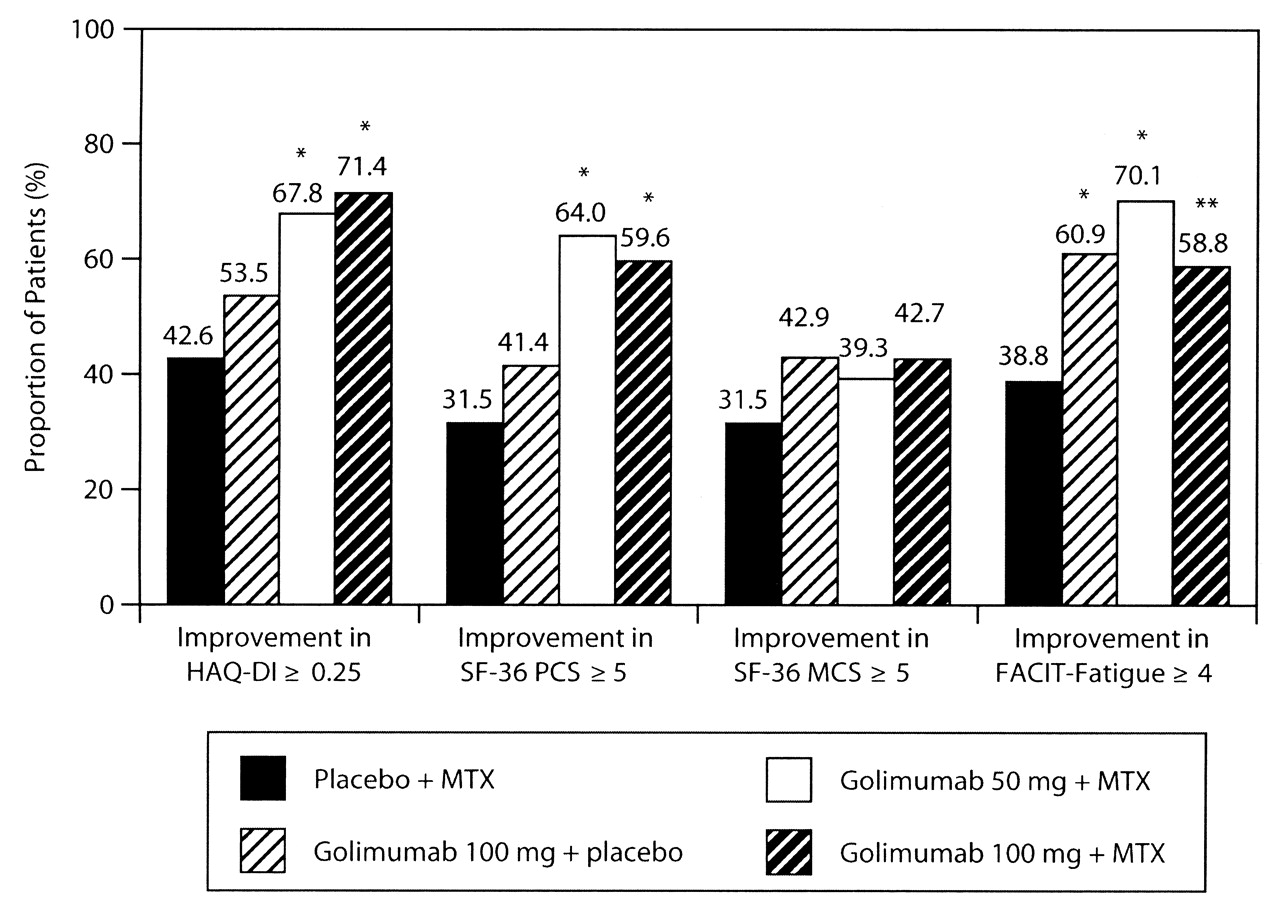
Proportion of patients achieving a clinically meaningful improvement from baseline to Week 14 in HAQ-DI, SF-36 PCS, SF-36 MCS, or FACIT-Fatigue scores. *p < 0.001; **p < 0.01. HAQ-DI: Disability Index of the Health Assessment Questionnaire; MCS: mental component summary; MTX: methotrexate; PCS: physical component summary; SF-36: Medical Outcomes Study Short Form-36.

Proportion of patients achieving a clinically meaningful improvement from baseline to Week 24 in HAQ-DI, SF-36 PCS, SF-36 MCS, or FACIT-Fatigue scores. *p < 0.001; **p < 0.01; ***p < 0.05. HAQ-DI: Disability Index of the Health Assessment Questionnaire; MCS: mental component summary; MTX: methotrexate; PCS: physical component summary; SF-36: Medical Outcomes Study Short Form-36.
Health status
Patients treated with golimumab 50 mg or 100 mg plus MTX had significantly greater improvement from baseline in mean (± SD) SF-36 PCS scores compared with the placebo plus MTX group at both Week 14 (8.02 ± 7.17 and 7.41 ± 8.04, respectively, vs 2.39 ± 7.80; p < 0.001 for both comparisons) and Week 24 (8.28 ± 8.33 and 7.01 ± 7.80, respectively, vs 2.54 ± 8.06; p < 0.001 for both comparisons; Table 2). Patients receiving golimumab 100 mg plus placebo also demonstrated significant improvement in mean SF-36 PCS score (4.72 ± 8.78; p = 0.033) at Week 14 compared with the placebo plus MTX group.
The proportions of patients achieving a clinically meaningful improvement (≥ 5 points) from baseline to Week 14 or Week 24 in PCS score were significantly greater in the golimumab 50 mg plus MTX group [64.0% (57/89) for both time-points] and the golimumab 100 mg plus MTX group [59.6% (53/89) and 57.3% (51/89), respectively] than in the placebo plus MTX group [31.5% (39/124) and 30.6% (38/124), respectively; p < 0.001 for all; Figures 1 and 2).
At Week 14, the mean (± SD) improvement in SF-36 MCS score for the golimumab 100 mg plus MTX group was significantly greater than that in the placebo plus MTX group (4.62 ± 10.17 vs 1.63 ± 9.81; p = 0.039; Table 2). At Week 24, both the golimumab 100 mg plus MTX group (4.33 ± 10.66; p = 0.014) and the golimumab 100 mg plus placebo group (3.37 ± 10.18; p = 0.033) had significantly greater mean improvement in MCS score compared with the placebo plus MTX group (0.75 ± 9.7; Table 2). There were no significant differences in mean improvement in MCS score between the golimumab 50 mg plus MTX group and the placebo plus MTX group at Weeks 14 and 24.
There were no significant differences between the golimumab groups and the placebo group in the proportion of patients achieving a clinically meaningful improvement (≥ 5 points) in MCS score at Week 14 (Figure 1). At Week 24, 44.9% (40/89) of patients in the golimumab 100 mg plus MTX group had a clinically meaningful improvement in MCS score compared with 29.0% (36/124) in the placebo plus MTX group (p < 0.05; Figure 2); no other statistically significant differences were observed between the golimumab groups and the placebo group.
Fatigue
At Week 14, significantly greater mean (± SD) improvements from baseline in FACIT-Fatigue scores were observed in the golimumab 100 mg plus placebo group (6.08 ± 10.81; p = 0.002), the golimumab 50 mg plus MTX group (7.58 ± 8.93; p < 0.001), and the golimumab 100 mg plus MTX group (6.40 ± 9.62; p = 0.002) compared with the placebo plus MTX group (2.28 ± 9.23; Table 2). Similar findings were observed at Week 24.
At both Weeks 14 and 24, the proportion of patients achieving a clinically meaningful improvement in the FACIT-Fatigue score was significantly higher in the golimumab 100 mg plus placebo group [60.9% (78/128), p < 0.001, and 60.0% (75/125), p < 0.05, respectively], the golimumab 50 mg plus MTX group [70.1% (61/87), p < 0.001, and 62.5% (55/88),p < 0.01, respectively], and the golimumab 100 mg plus MTX group [58.8% (50/85) and 63.2% (55/87), respectively; p < 0.01 for both] compared with the placebo plus MTX group [38.8% (50/129) and 44.1% (56/127), respectively; Figures 1 and 2].
Additionally, FACIT-Fatigue scores correlated with HAQ-DI scores at baseline (r = −0.550, p < 0.0001), and improvement in FACIT-Fatigue scores correlated with improvements in HAQ-DI scores at both Week 14 (r = 0.536, p < 0.0001) and Week 24 (r = 0.545, p < 0.0001; data not shown).
Longterm outcomes at Week 52
Improvements in SF-36 PCS, SF-36 MCS, and HAQ-DI scores were maintained from Week 24 through Week 52 among patients treated with golimumab 50 or 100 mg plus MTX. Patients who were initially assigned to receive placebo plus MTX and later switched to golimumab 50 mg plus MTX at either Week 16 (early escape) or Week 24 (crossover) achieved mean improvements in SF-36 PCS and MCS scores that were comparable to those for patients originally randomized to receive golimumab plus MTX at baseline (Table 3). The combined golimumab plus MTX group had a significantly greater mean improvement in HAQ-DI score compared with the placebo (golimumab crossover) plus MTX group.
DISCUSSION
Patients with RA can experience marked limitation of their physical function, which in turn can negatively affect their work productivity26. Improvements in physical function and fatigue have been associated with improvement in productivity27. Patients treated with golimumab (50 or 100 mg) plus MTX had significantly improved HAQ-DI scores at both Week 14 and Week 24 in our study. Importantly, treatment with golimumab plus MTX through Week 24 resulted in nearly twice as many patients achieving at least a 0.25-unit improvement in the HAQ-DI score compared with patients who received placebo plus MTX through Week 24. Mean improvements from baseline in HAQ-DI scores through Week 24 were sustained or enhanced through Week 52 of golimumab plus MTX therapy. Differences in response among the golimumab treatment groups could not be determined from this analysis as the study was not designed to compare the golimumab treatment regimens.
Significant improvements in the functional status as reported by mean SF-36 PCS and MCS scores were also observed with golimumab treatment through Week 14 and/or Week 24. At Week 52, there was no statistically significant difference in the proportion of patients achieving clinically meaningful improvements in PCS or MCS scores among patients who were initially assigned to golimumab plus MTX and those who were initially assigned to placebo plus MTX and switched to golimumab 50 mg plus MTX at either Week 16 or Week 24.
The vast majority of patients with RA experience fatigue. In addition, more than half of patients with RA identify fatigue as the most bothersome aspect of their disease28. All 3 golimumab regimens we studied (i.e., 100 mg plus placebo, 50 mg plus MTX, and 100 mg plus MTX) resulted in significant improvement from baseline to Weeks 14 and 24 in FACIT-Fatigue scores. Among all patients, improvements in fatigue were significantly correlated with improvements in physical function. In addition, results of a posthoc analysis showed that significantly higher proportions of patients receiving golimumab achieved a clinically meaningful improvement (i.e., improvement of at least 4 points) at Weeks 14 and 24 when compared with patients receiving placebo plus MTX. Among changes from baseline observed in the golimumab 100 mg plus placebo group, improvements in mean FACIT-Fatigue scores were significant at Weeks 14 and 24. This may indicate that fatigue is an outcome that is sensitive to change for assessing treatment efficacy, and more studies are needed to explore the treatment effect of therapies on fatigue in patients with RA.
In previous studies of patients with RA, improvements in health-related quality of life outcomes were associated with improvements in measures of disease activity, such as the Disease Activity Score 2829,30. Thus, health-related quality of life is an important aspect of RA that should be considered when evaluating a patient’s overall response to therapy. In our analysis, patients with active RA who received golimumab plus MTX administered subcutaneously every 4 weeks had improved physical function, general health, and fatigue compared with those who received placebo plus MTX. These results are consistent with previous findings that golimumab plus MTX improves disease activity in patients with RA19.
Acknowledgment
The authors thank Rebecca E. Clemente, PhD, Michelle Perate, MS, and Mary Whitman, PhD, of Janssen Services, LLC for assistance with preparing the manuscript.
Footnotes
-
Supported by Janssen Research & Development, LLC, Malvern, PA, and Schering-Plough, Kenilworth, NJ, USA.
-
MCG and ECK received research support to conduct this trial and have served as consultants to Janssen Research & Development, LLC. ECK has been a member of advisory boards for Janssen Research & Development, LLC. CH, JB, TG, and SP are or were employees of Janssen Global Services, LLC, at the time this study was conducted and own/owned stock in Johnson & Johnson. ECH, ZW, MUR are or were employees of Janssen Research & Development, LLC, at the time this study was conducted and own/owned stock in Johnson & Johnson.
- Accepted for publication January 13, 2012.








{kind=link}
{kind=link}