

Abstract
Objective. To assess agreement and application of Treat to Target (T2T) recommendations in Canadian practice.
Methods. A survey of Canadian rheumatologists was conducted on the recommendations of T2T, an international initiative toward reaching specific therapeutic goals in rheumatoid arthritis. Agreement with each recommendation was measured on a 10-point Likert scale (1 = fully disagree, 10 = fully agree). A 4-point Likert scale (never, not very often, very often, always) assessed application of each recommendation in current practice. Responders who answered “never” or “not very often” were asked whether they were willing to change their practice according to the particular recommendation.
Results. Seventy-eight rheumatologists responded (24% of the 330 who were contacted). The average agreement scores ranged from 6.92 for recommendation #5 (the frequency of measures of disease activity) to 9.10 for recommendation #10 (the patient needs to be involved in the decision-making process). A majority of participants indicated that they apply the T2T recommendations in their practice. Recommendations dealing with frequency of visits and the use of composite measures received the highest number of “never” or “not very often” responses. Busy practices and lack of confidence in composite outcome measures were the main reasons for objections to certain components of the recommendations.
Conclusion. Although a majority of Canadian rheumatologists agreed with and supported the T2T recommendations, there was resistance toward specific aspects of these recommendations. Efforts are needed to better understand the reasons behind identified disagreements. Action plans to encourage the application of T2T recommendations in Canada are in development.
Over the past 2 decades, there has been a significant shift in treatment models for rheumatoid arthritis (RA). In addition to the introduction of biologics, which has made longterm remission and prevention of irreversible joint damage highly achievable1,2,3,4, we have also witnessed significant advances in the availability of various tools and measures that can guide clinical practice and therapeutic approaches toward optimal outcomes5,6,7. Despite this, a wide heterogeneity of treatment strategies and outcome expectations still exists in daily practice, leaving a significant proportion of patients with suboptimal control of their disease8,9,10.
Treat to Target (T2T) is an international initiative aimed at providing rheumatologists with clear guidance as to how to reach specific therapeutic goals in RA, to ameliorate patient care11. To that end, a set of 10 recommendations based on both clinical evidence and expert opinion were developed and proposed as the international standard of RA care (Table 1).
Treat to Target in Rheumatoid Arthritis recommendations.
To ensure acceptance and implementation of these recommendations in daily rheumatology practice, a series of international and national surveys of rheumatologists has been proposed12. The objectives of these surveys are 3-fold. First, the surveys aim to evaluate the level of agreement with the T2T recommendations on global and national scales. The second objective is to determine physicians’ perceptions of the extent of their personal application of these recommendations in their practice. Finally, the surveys assess the willingness of clinicians to apply these recommendations in their practice.
Here we provide the results from the survey of Canadian rheumatologists. An attempt is also made to identify the main barriers to applying the T2T recommendations to Canadian practice.
MATERIALS AND METHODS
The Canadian rheumatologists were contacted by e-mail and/or fax and asked to complete a Web-based questionnaire. No incentives were offered. Nonresponders received several e-mail and/or fax reminders. The survey comprised a 6-page document. The first part of the questionnaire gathered demographic information and provided the overarching principles, and the second part requested responder feedback on each recommendation. Agreement with each recommendation was measured on a 10-point Likert scale (1 = fully disagree, 10 = fully agree). A 4-point Likert scale (never, not very often, very often, always) assessed application of each of the recommendations in current practice. Responders who answered “never” or “not very often” were asked whether they would be willing to change their practice according to the particular recommendation. Demographic data were used to evaluate any statistical differences between groups based on setting (academic vs nonacademic hospital), number of years in practice, number of patients seen per month, etc. Data are presented using standard summary statistics.
The survey allowed respondents to provide optional comments on the level of agreement, as well as application of a recommendation in practice. The feedback gathered from these comments served as an indication of the perceived obstacles and issues with each T2T recommendation.
RESULTS
Demographics
Seventy-eight physicians (13 French and 65 English speaking) responded. Taking into consideration that 330 Canadian rheumatologists were contacted, the response rate was 24%. The majority of the physicians who responded saw their patients in their private offices (50%) or in a university hospital (37%). Of the remainder, 8% indicated having a practice in general hospitals and 5% having a mixed practice (4% private clinic/general hospital and 1% private clinic/university hospital). The average number of years in practice of the responders was 18, ranging from 3 months to 40 years. The average number of patients with RA seen per month was 98, ranging from 10 to 400 patients per month.
Agreement with the recommendations
Agreement with T2T recommendations ranged from 6.9 to 9.1 (recommendations #5 and #10, respectively; Figure 1). There were no significant differences between rheumatologists practicing in academic (n = 30; 38%) and nonacademic (n = 48; 62%) institutions (Table 2). In addition, individual ANOVA for each of the 10 recommendations revealed no significant differences in scores regarding patient load (number of patients with RA seen per month) or years of practice.
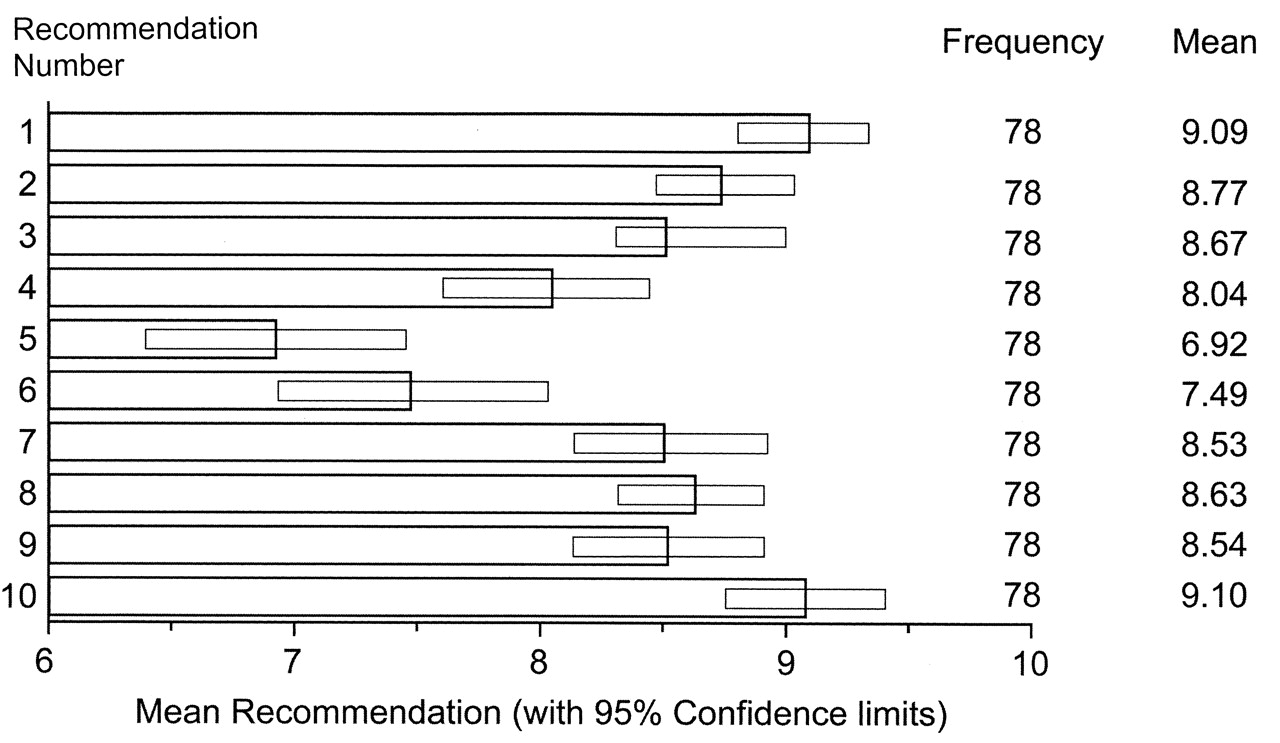
Average agreements scores for the 10 individual recommendations.
Agreement scores for the 10 recommendations: academic versus nonacademic.
Application of the recommendations in daily practice
Application of the T2T recommendations in daily practice was also relatively high (Figure 2). The majority of responses were “always” and “very often”; from 100% for recommendation #8 to 66.7% for recommendation #5. However, recommendations #5 and #6 received the highest number of “never” or “not very often” responses, 33.3% and 32.1%, respectively.

Frequency of application of each recommendation in daily practice.
Willingness to change practice according to recommendations
It is important to note that a substantial percentage of responders who are currently not applying the T2T recommendations in their practice were unwilling to change their practice according to the recommendations (Figure 3). This might not be a significant issue, because a majority of participants indicated that they are already applying these in their current practice. However, recommendations #4, #5, and #6 clearly require further attention: 92% out of 15.4%, 73% out of 33.3%, and 68% out of 32.1% of responders (who responded “never” or “not very often”) are not willing to change their practice according to recommendations #4, #5, and #6, respectively. There was no difference in willingness to change practice between clinicians practicing in nonacademic versus academic institutions. Further, willingness to change was not affected by patient load.
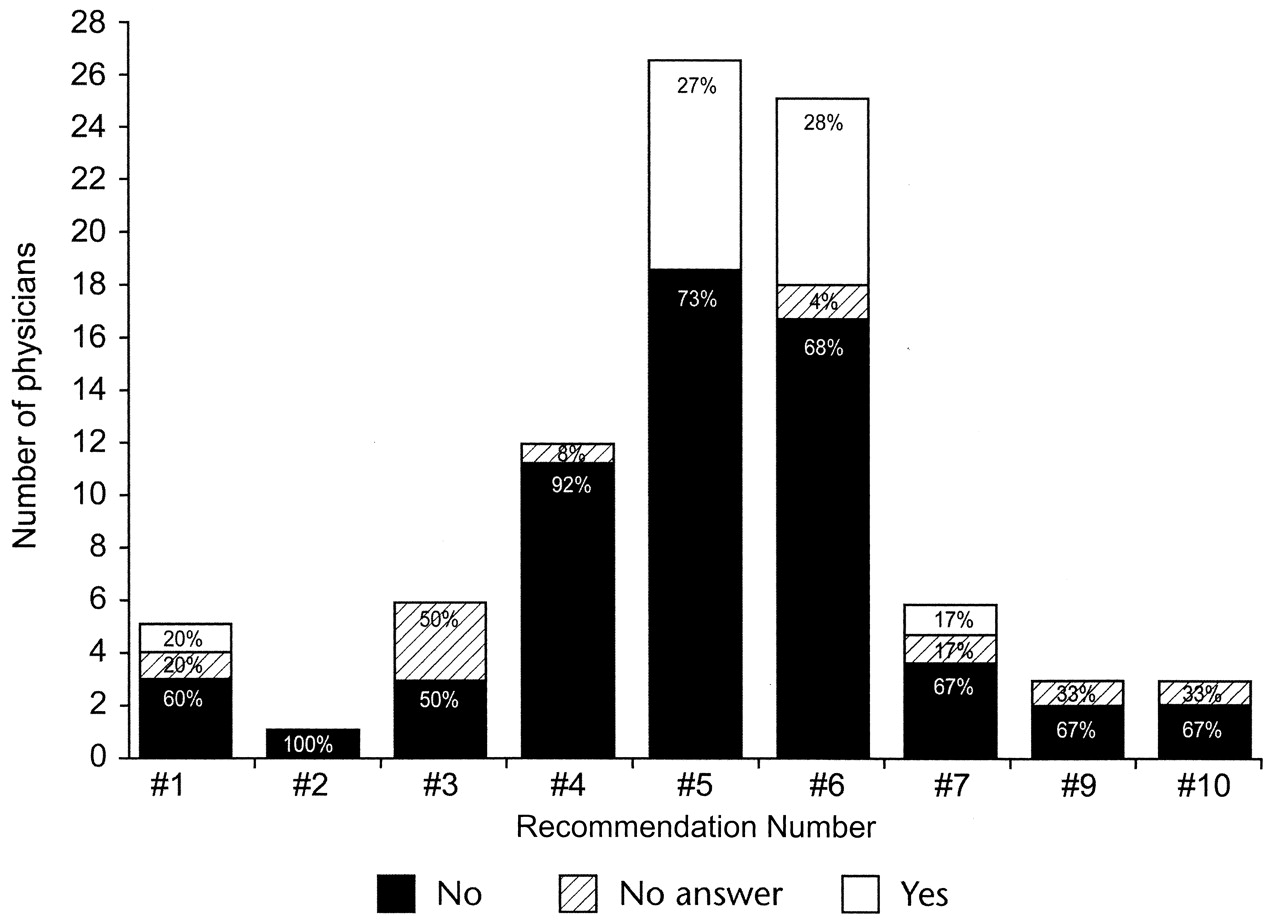
Physician willingness to change clinical practice according to individual recommendation.
A busy clinical practice, accompanied by a shortage of supporting staff, was identified as the main barrier to full compliance with the T2T recommendations from the physician standpoint. Further, geographic location, traveling arrangements, and reimbursement issues, as indicated by the optional comments made by the responders, prevent many patients with RA from keeping up with the tight followup schedules of the T2T recommendations.
DISCUSSION
This nationwide survey provides an overview of perceptions, attitudes, and approaches to RA treatment in Canada. The results clearly indicate that a majority of Canadian rheumatologists are aware of the latest shifts in the management of RA, and are presumably applying them in their daily practice. The survey also revealed different levels of interest and agreement with various aspects of the T2T initiative, identifying the potential for future endeavors and activities. Finally, the results hinted at potential barriers to implementation and compliance with T2T recommendations in Canadian clinical practice. These should be further examined at both the national and provincial levels to identify the appropriate strategies and efforts needed to ensure optimal care to all Canadians living with RA.
The Canadian Rheumatology Association (CRA) has recently published recommendations for the pharmacological management of RA with traditional and biologic disease-modifying antirheumatic drugs13. These recommendations are in agreement with the T2T initiative and were guided by aspects of the Canadian healthcare system. Thus, these survey results might provide an early indication as to how the CRA recommendations will be perceived and accepted within the Canadian rheumatology community. On the other hand, the CRA guidelines might also help in overcoming some of the reluctance toward specific aspects of the T2T recommendations (i.e., frequency of assessment and the use of composite measures).
There are several limitations to consider when interpreting these results. First, although the 24% response rate was considered acceptable, the yielded sample size might be too small to show statistically significant differences among the various demographic groups. Second, there might be a selection bias, because responders may have been more willing to consider the T2T recommendations. Because of this, some responses may not be completely representative of the Canadian rheumatology community. Finally, the applied methodology might not accurately assess to what extent these recommendations are implemented in clinical practice because chart audits were not performed.
It is reassuring that Canadian rheumatologists accept remission as the ultimate therapeutic goal in RA (the agreement score for recommendation #1 was 9.1), as this was one of the T2T Expert Committee’s major and almost unanimous conclusions11. The CRA recommendations also state that remission is the ultimate goal of RA treatment13.
The responding rheumatologists also recognized that the patient should be an integral part of the decision-making process, whether the process is therapy-related or treatment target-related (the agreement score for recommendation #10 was 9.1). This is of particular importance in an era when patient-reported outcomes are becoming increasingly applied as endpoints in clinical trials and are often requested by governing agencies and insurance providers for decision-making purposes. Further, active patient participation in a therapeutic decision process enhances compliance and facilitates the achievement of treatment goals.
Although these results appear in line with results obtained from the international T2T survey12, some differences are worth noting. First, recommendations related to the frequency of visits and the regular use of composite measures to assess response received significantly lower agreement scores of 6.9 and 7.5, respectively, from Canadian rheumatologists, compared to scores of 8.5 and 8.7 at the international level. Second, while a majority of international responders who indicated that they are not currently using a specific T2T recommendation in their clinical practice are willing to change their practice, this was less evident with Canadian physicians. Although individual mind-set and personal experience might be contributing factors, other aspects such as patient volume, payment schemes, and lack of support are also likely to affect overall attitudes.
Indeed, several responders indicated that their busy practice and lack of supporting staff prevent them from evaluating patients as frequently as recommended in T2T. Others felt that such a tight monitoring schedule was unnecessary. Canadian rheumatologists also perceived validated composite measures of disease activity to be too complicated for daily practice. This is in accord with the findings from a recent practice audit that suggested that the determination of disease activity in Canadian rheumatology practice is often based on clinical judgment and that rheumatologists often chose not to rely on standard disease activity measures9. In-depth analysis of composite measures and their usefulness in daily clinical practice is beyond the scope of this report. Our goal is simply to report the results of a survey that was somewhat limited in its scope and based on a published set of recommendations. Further, the approval process for biological agents varies between provinces. Different provincial requirements may have influenced this survey but this could not be determined in the analysis because of the small number of physicians after stratification by province. It remains to be determined to what extent the provincial requirements affect the willingness of clinicians to adjust therapy to as frequently as every 3 months (T2T recommendation #4).
In Canada, geographic location may also present a significant barrier to healthcare services14. Residents of rural communities usually have access to a limited range of services and often have to travel long distances to reach urban clinics for specialized care15. This might have a significant effect on Canadian rheumatologists in regard to appointment scheduling.
Although the results of this survey demonstrated relatively strong agreement and support of the T2T recommendations among the Canadian rheumatology community, they also revealed resistance toward certain recommendations. Additional efforts are needed to better understand the reasons behind the identified disagreements. These reasons could be used to develop action plans to encourage the adoption and application of the T2T recommendations, as also conveyed by the recently published CRA recommendations for the management of RA13.
Acknowledgment
The authors gratefully acknowledge Radmila Day for assistance with the drafting of this manuscript and Lorenz Luthe for providing statistical analysis.
Footnotes
-
Full Release Article. For details see Reprints/Permissions at jrheum.org
- Accepted for publication January 13, 2012.
Free online via JRheum Full Release option








{kind=link}
{kind=link}
{kind=link}