

Abstract
Objective. To investigate possible associations between occupation and hospitalization for systemic lupus erythematosus (SLE) in a nationwide study.
Methods. A nationwide database was constructed in Sweden by linking the Swedish Census to the Hospital Discharge Register to obtain data on all first hospitalizations with a primary or secondary diagnosis of SLE in adults during the study period (1970 to 2008). Standardized incidence ratios (SIR) and 95% CI were calculated for different occupations. Two cohorts were defined based on occupational titles recorded in Swedish census data in 1970 and 1980.
Results. A total of 8921 male and 42290 female hospitalizations for SLE were retrieved in individuals aged over 15 years. High education (> 12 yrs) was associated with a lower risk of hospitalization for SLE among both women (SIR = 0.73) and men (SIR = 0.72). Among men with the same occupation in 2 consecutive censuses, increased risks (SIR) > 2.0 were present among artistic workers (2.52); shop managers and assistants (3.63); miners and quarry workers (6.04); shoe and leather workers (6.93); plumbers (2.21); other construction workers (2.08); glass, ceramic and tile workers (4.43); chimney sweeps (4.54); and military personnel (3.01). Among women with the same occupation in 2 consecutive censuses, no occupation was associated with SIR > 2.0.
Conclusion. Occupation may carry significantly increased risk of hospital admission for SLE. Especially among men, several occupations were associated with increased risks for SLE.
The causes of systemic lupus erythematosus (SLE) are incompletely understood. A multifactorial etiology involving genetic susceptibility, age, hormonal factors, and environmental triggers has been suggested. Case reports have suggested possible roles for various infectious triggers of SLE, and the strongest evidence for a relationship between infection and SLE is the case of Epstein-Barr virus. Cigarette smoking and a number of occupational and environmental exposures, e.g., silica, solvents and chemicals, have also been associated with SLE1.
There is a growing body of evidence implicating socioeconomic status (SES) as a risk factor for SLE2,3,4. Socioeconomic factors may influence the risk of the disease in many ways. For example, exposure to harmful agents may be related to occupational, residential, and lifestyle factors, which may depend on SES. Some studies have found increased risks for incident SLE among some occupational categories2,4,5, and increased mortality in SLE among different occupations6; few studies have reported associations between specific occupations and the incidence of SLE5,7,8. Most studies to date have been case-control studies, and most of these have used prevalent cases and relied on self-reporting for exposure assessment, which may lead to survivorship and recall bias. Due to the lack of nationwide population-based data on the association between socioeconomic and occupational factors and SLE, we conducted a followup study of the entire Swedish population. Our aim was to investigate the association between education, occupation, and hospitalization for a primary or secondary diagnosis of SLE among men and women over 15 years of age.
MATERIALS AND METHODS
MigMed research database
Data used in our study were retrieved from the MigMed database, located at the Center for Primary Health Care Research at Lund University, Sweden. MigMed is a single, comprehensive database that contains individual-level information on all people in Sweden, including age, sex, SES (education), occupation, geographical region of residence, hospital diagnoses and dates of hospital admissions in Sweden (1964–2008), date of emigration, and date and cause of death. This unique database was constructed using several national Swedish data registers including, but not limited to, the total population register, the multigeneration register, and the Swedish hospital discharge register (1964–2008)9,10,11.
Information retrieved from the various registers in the MigMed database was linked at the individual level by the national 10-digit civic registration number assigned to each person in Sweden for his or her lifetime. Prior to inclusion in the MigMed database, civic registration numbers were replaced by serial numbers to ensure the anonymity of all individuals.
From this database, individuals were allocated to 1 of 2 census cohorts based on their occupational history. The 1970 census cohort consisted of individuals with a registered occupation in the 1970 census; the 1970/1980 census cohort consisted of individuals with the same registered occupation in the 1970 and 1980 censuses, i.e., in 2 consecutive censuses. Two cohorts were defined for both men and women: the first cohort included persons aged ≥ 15 years in 1970 and categorized according to their occupational status in 1970, and the second cohort included persons aged ≥ 15 years in 1970 who retained the same occupational title in 1970 and 1980. The starting point for the followup periods differed between the 2 cohorts (see Table 2 and 3). All followup periods proceeded until first hospitalization for SLE, death, emigration, or the end of the study on December 31, 2008.
Outcome variable
The eighth, ninth, and tenth revisions of the International Classification of Diseases (ICD-8, ICD-9, ICD-10) were used to identify all hospital admissions with a primary or secondary diagnosis of the outcome variable SLE during the study period (1970–2008; ICD-8, code 734.1; ICD-9, code 710.0; ICD-10, code M32).
Individual variables controlled for in the analysis
Gender: men and women.
Age at hospitalization was categorized in 5-year groups starting at 15 years. Occupation was coded according to national adaptations of the Nordic Occupational Classification (NYK). NYK is a common Nordic adaptation of the International Standard Classification of Occupation from 1958. Three-digit codes were combined into 53 NYK occupational groups and 1 economically inactive group12. Occupational groups were combined based on similarities in the included occupations.
Educational level was classified into 3 categories: completion of compulsory school or less (≤ 9 yrs), completion of high school or some high school (10–12 yrs), and more than high school (> 12 yrs). Educational level was chosen as a marker for SES, because education could be regarded as a stable measure of SES.
Geographical region was divided into (1) large cities (cities with a population > 200,000, i.e., Stockholm, Gothenburg, and Malmö); (2) Southern Sweden; and (3) Northern Sweden. Large cities were defined in a separate category because it is likely that individuals living in large cities have better access to healthcare. In addition, they are more exposed to air pollution. Sweden is divided into 25 counties. Geographical region was included as an individual variable to adjust for possible differences between geographical regions in Sweden regarding hospital admissions for SLE.
Immigrant status was classified into 2 categories: individuals born in Sweden and individuals born outside Sweden.
Comorbidity was defined as hospitalization for a primary or secondary diagnosis of the following: (1) chronic obstructive pulmonary disease (COPD) 490–493 (ICD-8), 490–496 (ICD-9), and J40–J49 (ICD-10); (2) alcoholism and alcohol-related disease, 291, 303, and 571 (ICD-8), 291 and 303 (ICD-9), and F10 and K70 (ICD-10). These comorbidities were included to adjust for possible increased risks for SLE associated with smoking and alcohol.
Statistical analysis
Person-years were calculated from the start of followup until first hospitalization for SLE, death, emigration, or closing date (December 31, 2008). Age-specific incidence rates (defined as first hospitalization during the study period) were calculated for the whole followup period, divided into five 5-year periods. Standardized incidence ratios (SIR) were calculated for different educational and occupational groups as the ratio of observed to expected number of cases13, using the entire cohort as reference with the assumption that various SES and occupational groups should experience the same incidence as all workers in the entire cohort. The expected number of cases was calculated for age (5-year groups), sex, period (5-year groups), region, SES (education), immigrant status, and comorbidity-specific SIR. Ninety-five percent CI were calculated assuming a Poisson distribution13.
Ethical considerations
The Ethics Committee at Lund University, Sweden, approved our study.
RESULTS
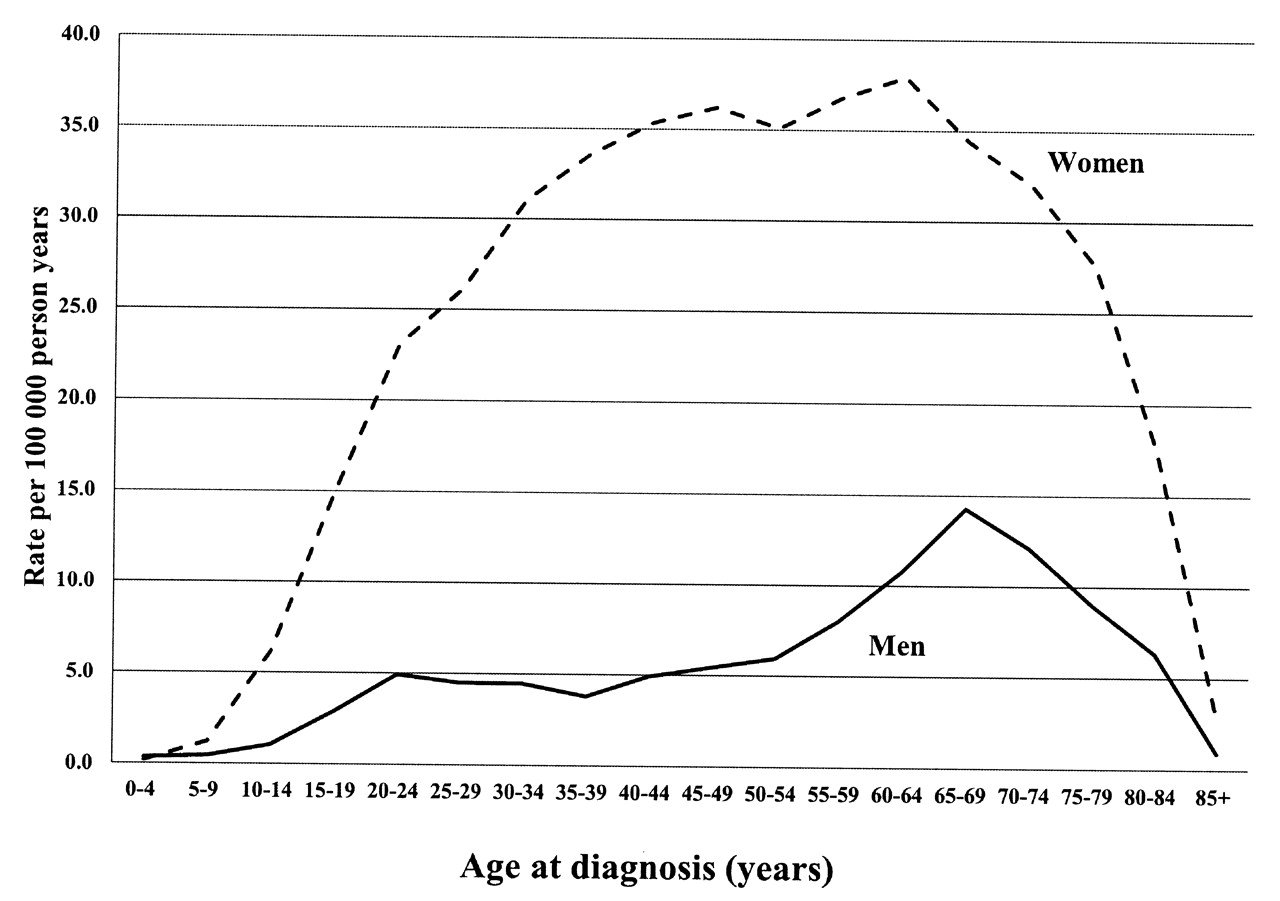
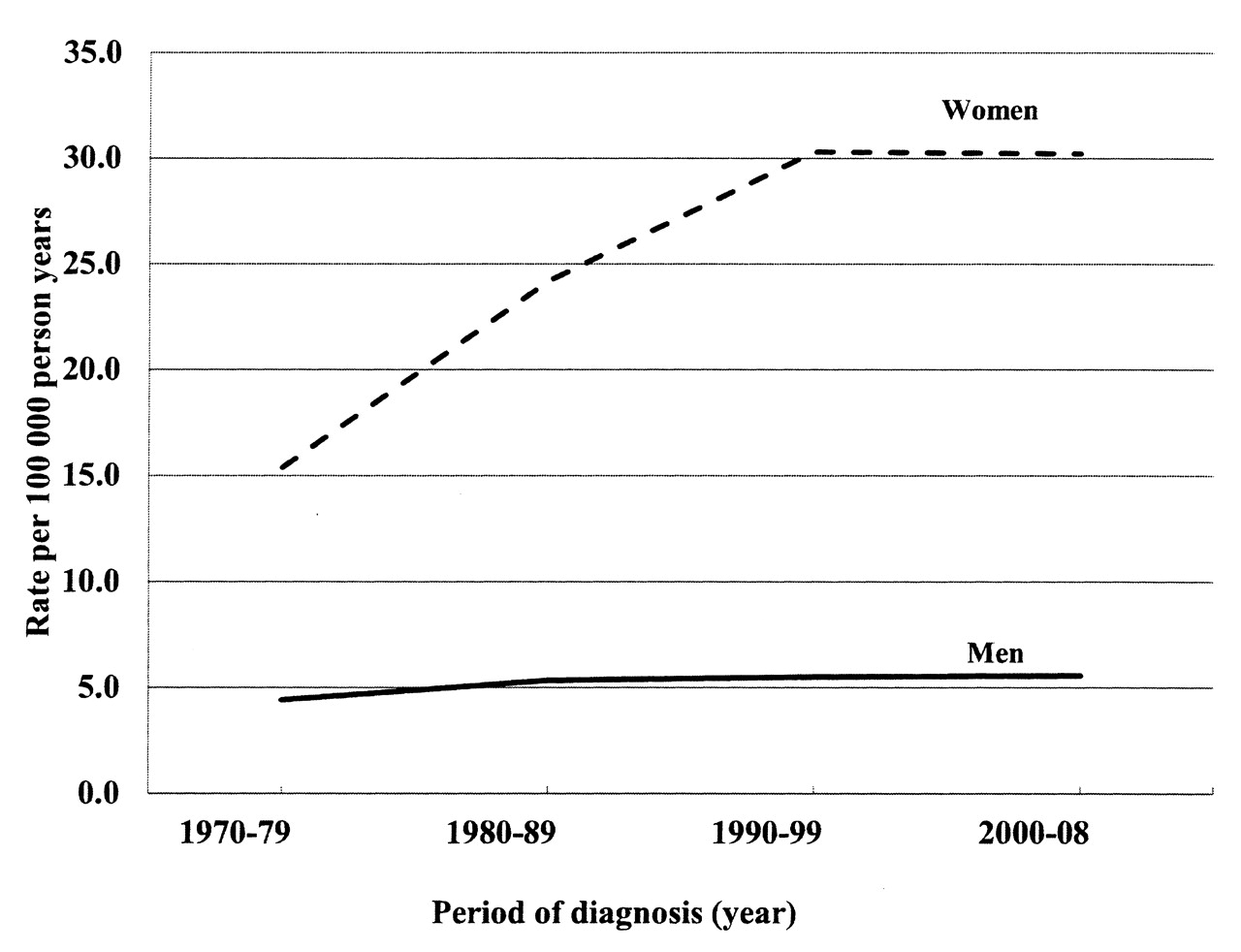
Table 1 shows the number of cases and SIR for hospitalization for SLE by educational level, region, age at diagnosis, immigrant status, and comorbidities among men and women followed 1970–2008. All SIR are also adjusted for time period. A total of 8921 men and 42,290 women over 15 years of age were hospitalized for SLE during the followup periods. Among those patients, 21% male and 15% female patients were diagnosed between 1970 and 1979, and 25% male and 28% female patients were diagnosed between 2000 to 2008 (data not shown). Age-adjusted hospitalization rates were 5.0 per 100,000 person-years for men and 26.6 per 100,000 person-years for women. The overall female-to-male ratio was 5.3:1. However, the female-to-male ratio varied by age interval (Figure 1). At ages 35 to 39 years, the rates were 4.0 per 100,000 person-years for men and 35.8 per 100,000 person-years for women (Figure 1), with a corresponding female-to-male ratio of 8.95. During the followup period, hospitalization rates increased from 15.4 per 100,000 person-years in the 1970s to 30.3 per 100,000 person-years in the 1990s in women. In men, however, hospitalization rates were 4.4 per 100,000 person-years in the 1970s and 5.5 per 100,000 person-years in the 1990s (Figure 2). Thus, the female-to-male ratio increased from 3.5:1 in the 1970s to 5.5:1 in the 1990s.

Age-specific incidence rate of systemic lupus erythematosus in men and women in followup 1970 to 2008.
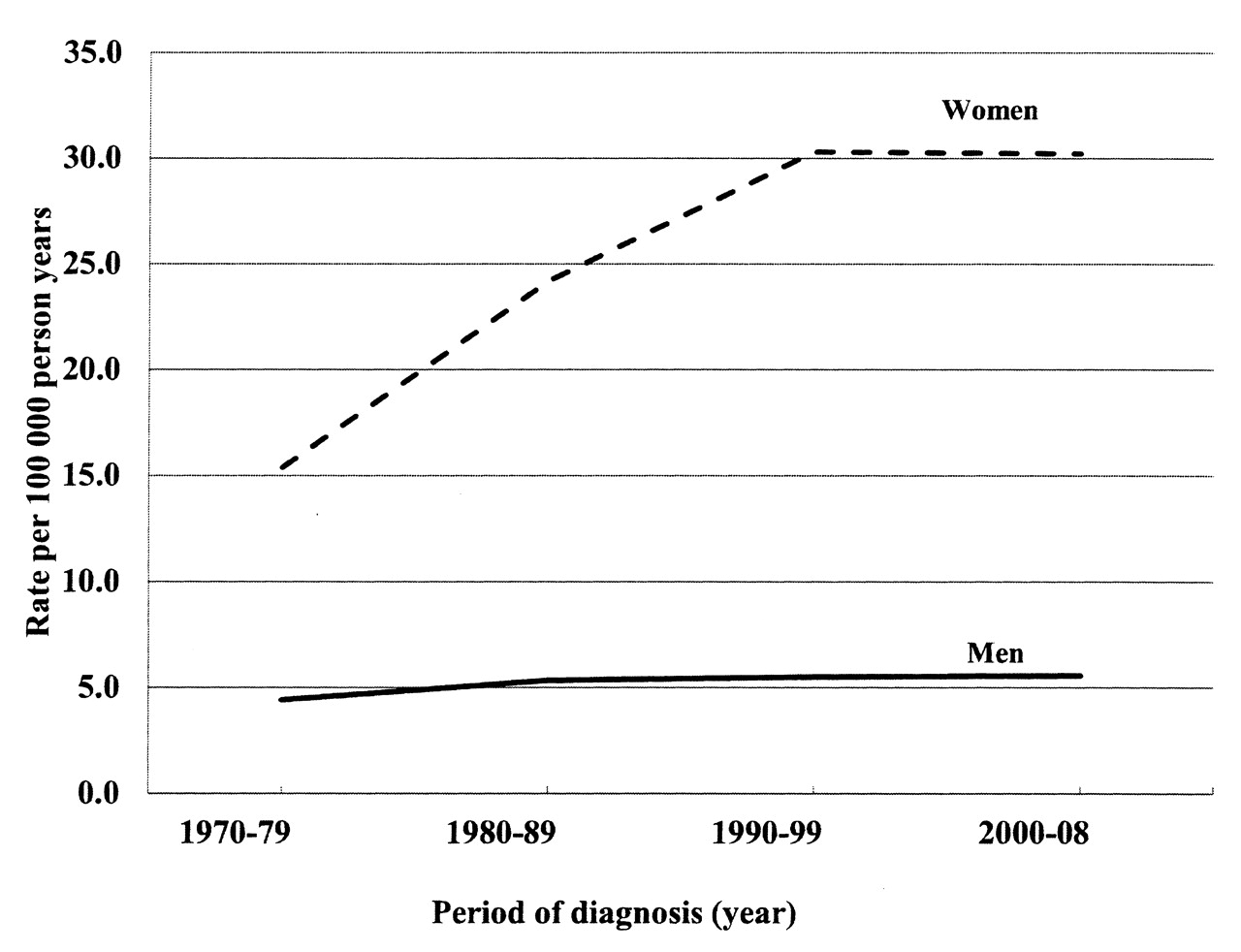
Age-adjusted incidence rate of systemic lupus erythematosus in men and women in followup 1970 to 2008.
Standardized incidence ratios (SIR) for hospitalization of systemic lupus erythematosus by different educational levels, region, age, immigrant status, and comorbidities in men and women.
Socioeconomic factors and hospitalized SLE
Lower risks for SLE were observed for both men and women who had attended college, i.e., > 12 years education (Table 1). Women living in big cities had a significantly increased risk of SLE. Significantly increased SIR of hospitalization for SLE were observed for men aged 60 to 79 years and women aged 30 to 79 years. Significantly increased SIR for hospitalization of SLE were also observed for both men and women hospitalized for COPD and alcoholism. Decreased SIR were observed for men > 50 years of age, men born outside Sweden, and women > 80 years of age.
Occupation and hospitalized SLE among men
SIR for hospitalization for SLE for men by occupation in the 2 cohorts (census 1970 and census 1970/1980, i.e., men who retained the same occupational title in 2 consecutive censuses) is shown in Table 2. Only occupations with > 10 cases for either cohort were included. All SIR were adjusted for age, period, region, educational level, immigrant status, and comorbidities. Among men, significantly increased SIR that were present in both cohorts were observed in shop managers and assistants; miners and quarry workers; shoe and leather workers; plumbers; electrical workers; wood workers; other construction workers; glass, ceramic and tile workers; chimney sweeps; and military personnel. Especially high SIR were observed for certain workers who kept the same job title in 2 consecutive censuses, i.e., shop managers and assistants (3.63), miners and quarry workers (6.04), shoe and leather workers (6.93), glass, ceramic, and tile workers (4.43), chimney sweeps (4.54), and military personnel (3.01).
Standardized incidence ratios (SIR) for hospitalization for systemic lupus erythematosus in men by occupation from census 1970 and in men who kept the same job title in 2 consecutive censuses (followup).
Occupation and hospitalized SLE among women
Table 3 shows SIR for hospitalization for SLE among women by occupation in the 2 cohorts (census 1970 and census 1970/1980, i.e., women who retained the same occupational title in 2 consecutive censuses). Only occupations with more than 10 cases for either cohort were included. Among women, public safety and protection workers had a particularly increased SIR (2.59) that was present in the 1970 census (followed 1970 to 2008).
Standardized incidence ratios (SIR) for hospitalization of systemic lupus erythematosus in women by occupation from census 1970 and in women who kept the same job title in 2 consecutive censuses (followup).
We performed an additional analysis with separate followup analyses for cohort 1 (1970 census): followup 1970–1979, 1980–1999, and 2000–2008. Results are shown in Tables 4 and 5. For certain occupations, the risks increased when the followup period increased. Among men, particularly high SIR that were present in later followup periods were observed in artistic workers (3.32), miners and quarry workers (10.22), postal and communication workers (2.17), plumbers (3.99), painters and wallpaper hangers (2.47), other construction workers (2.70), and chimney sweeps (9.84). Among women, particularly high SIR were observed for journalists (3.50) and public safety and protection workers (4.31) in later followup periods.
Standardized incidence ratios (SIR) for hospitalization of systemic lupus erythematosus in men by occupation from census 1970.
Standardized incidence ratios (SIR) for hospitalization of systemic lupus erythematosus in women by occupation from census 1970.
DISCUSSION
The main finding of our study is that education level and occupation sometimes carry a significantly increased risk of hospitalization for SLE. For example, decreased SIR for SLE were observed for both men and women who had an educational level > 12 years. Among men, significantly increased SIR were present in both cohorts among shop managers and assistants; miners and quarry workers; shoe and leather workers; plumbers; electrical workers; wood workers; other construction workers; glass, ceramic, and tile workers; chimney sweeps; and military personnel. Among women, only religious, juridical, and other social-science-related workers had an increased SIR in both cohorts. No increased risks were found for most occupational groups among women. Thus, more occupations among men than women were associated with increased risk for SLE. To the best of our knowledge, this is the first study to investigate the association between education and occupations and the risk of hospitalization for SLE in an entire population aged over 15 years.
The highest hospitalization rates of SLE occurred in the 50–60-year age category for women and in the 60–70-year age category for men and with an overall female-to-male ratio 5.3:1. Our results are consistent with a UK study with a similar age pattern and overall female-to-male ratio14. Two studies have previously estimated the incidence rate of SLE in Sweden15,16. Jonsson, et al determined the age-specific incidence of SLE in a defined population in southern Sweden in multiple sources of retrieval during 1981–198616. The female incidence rate was 5.4/100,000/year and the male incidence rate was 1/100,000/year. Thus, the female-to-male ratio was 5.4:1, which is similar to our present study. Ståhl-Hallengren, et al studied the incidence of SLE in the same area but for the years 1987–199115. The median annual incidence was 4.8/100,000/year. The age and sex-specific incidence rates between 1987–1991 were notably highest in ages 65–74 (14.1/100,000/year) in women and ages 65–74 (3.2/100,000/year) in men. The point prevalence on December 31, 1986, was 42/100,000 and on December 31, 1991, 68/100,000. In our present study the hospitalization rate was somewhat higher than the estimated incidence in the 2 previous Swedish studies. This may be because hospitalizations reflect not only incident cases of SLE but also prevalent cases with relapse that need hospital admission. In addition, our study involved a later time period and a larger population sample.
Education level was chosen as an individual variable in our study because education can be regarded as a stable measure of SES. Education level may influence the risk of disease in many ways and is an important attribute in the selection of an occupation. It is common for people with certain occupations, such as teacher, administrator, and manager, to have a higher level of education. This, in turn, is a predictive factor for disposable income and many socioeconomic aspects of life, including residential and lifestyle factors. In the present study, we found an increased risk of hospitalization for SLE in individuals with a lower level of education, which is consistent with findings from earlier studies17. Low SES may influence the risk of SLE through factors such as infections, psychosocial stressors, occupational exposures, and poor nutrition, which are also more common for other autoimmune diseases4,18,19,20.
Occupational factors have been indicated to be involved in the etiology of SLE. The association between occupation and proximity to specific agents was assessed according to occupational exposures4,5,7,21,22. The risk of hospitalization for SLE was consistent with these studies. For men, this applied to the following occupations: miners and quarry workers; construction workers; and glass, ceramic, and tile workers. Increased risks for these occupations are consistent in different cohorts, and the risks were even higher in the 1970/1980 cohort, i.e., those who kept the same job title in 2 consecutive censuses. The main exposures in these groups are assumed to be silica, vibrations, engine oils, metal, and exhaust fumes as well as asbestos exposure among the construction workers.
There is strong epidemiological evidence that supports an association between occupational crystalline silica exposure and several diseases such as lung cancer23,24, COPD24, renal disease25, rheumatoid arthritis (RA)22,24, SLE22,24, and other autoimmune disorders22. Silica dust exposure occurs in a wide variety of industries and occupations, including miners and quarry workers, glass manufacture, ceramics, and various occupations in construction and manufacturing22,24,26. In accordance with these studies, our study showed that the risk of SLE was increased among men with similar occupational exposures.
For women, fewer silica-related occupations were associated with increased risks of SLE, maybe because women may work in jobs with shorter or less intense silica exposure, and women are less likely than men to work in the dusty trades.
Chemical exposures occur frequently in these occupations, for example, solvents and chemical cleaning agents. Earlier epidemiological studies have reported that solvent exposure increased the risks for SLE4,5,7. In our population-based database, however, information on detailed job assignments and potential environmental exposures inside or outside the workplace was not available. We had no information about specific chemicals, so it is difficult to identify which kind of chemical agent had a causative association.
Our study has a number of strengths, for example, the study population included a well-defined open cohort of the entire population of Sweden. Thanks to the civic registration number assigned to each individual in Sweden (changed to a serial number to ensure anonymity), it was possible to track the records of every person for the whole followup period. Data about occupational status were almost 100% (99.2%) complete. Additionally, the data in the Swedish Hospital Discharge Register are also highly complete. In 2001, the main diagnosis was missing in 0.9% and the national registration number in 0.4% of hospitalizations9.
Our study also has some limitations. For example, we had no data on several individual risk factors for SLE. In a register that includes an entire population, it is not feasible to include individual data on, e.g., smoking. However, the possible confounding effect of smoking and alcohol drinking was partly taken into account by including the variables COPD (as a surrogate of smoking) and alcoholism/alcohol-related diseases. As we only analyzed hospitalizations, some SLE cases may have been diagnosed before the first hospitalization for SLE in, e.g., an outpatient setting, which is a potential weakness of the study. Further, there were broad changes in the Swedish labor market during the study period27,28. Lack of information on the duration of employment was partly remedied by the analysis of individuals who maintained the same occupation in 2 consecutive censuses. The quality of data on occupational titles in the Swedish censuses has been assessed by Warnryd and coworkers29. The results showed that the proportion of concordant occupational titles was 72%, suggesting a reasonable quality for the census data. The large number of comparisons is another limitation and is a technical point worthy of consideration. Some associations might undoubtedly have been due to chance, and consistency within this study and between studies, as well as biological plausibility, should be assessed for causal inference. However, according to Rothman, adjusting for multiple comparison is not advisable29: “A policy of not making adjustments for multiple comparisons is preferable because it will lead to fewer errors of interpretation when the data under evaluation are not random numbers but actual observations on nature. Further, scientists should not be so reluctant to explore leads that may turn out to be wrong that they penalize themselves by missing possibly important findings.” In addition, early symptoms of disease before actual onset may influence a person’s choice of profession, which may in turn influence the results.
Another limitation is that SLE was not validated specifically in the hospital discharge register. However, an external review and validation of the Swedish national inpatient register (IPR) has been published29. A total of 132 papers were reviewed. The positive predictive value (PPV) differed between diagnoses in the IPR, but was generally 85–95%. The PPV for RA varied between 87.9 and 95.9% and the PPV for granulomatosis with polyangiitis (Wegener’s) was 87%.
Our study suggests that education and occupation sometimes carry significantly increased risks of hospitalization for SLE. Occupational risk factors for SLE appear to be more common among men than women. Occupational groups with possible exposure to silica, vibrations, organic solvents, and other chemicals may entail a “true” risk for SLE.
Footnotes
-
Supported by grants from the Swedish Research Council (2008–3110 and 2008–2638), the Swedish Council for Working Life and Social Research (2006–0386, 2007–1754, and 2007–1962), and the Swedish Research Council Formas (2006-4255-6596-99 and 2007–1352).
- Accepted for publication December 20, 2011.








{kind=link}
{kind=link}