

Abstract
Objective. To determine the timeliness of consultation and initiation of disease-modifying antirheumatic drugs (DMARD) in patients with rheumatoid arthritis (RA) referred to rheumatologists.
Methods. The first part of the study was a review of the charts of 151 patients with RA followed by 3 rheumatologists. The outcome measure was the interval between symptom onset and consultation with a rheumatologist. The second part of the study involved a chart review of 4 family physician practices in a small urban center in order to determine the accuracy of diagnostic coding (International Classification of Diseases; ICD-9) of RA, as well as the proportion of patients with RA seen by a rheumatologist. Finally, a survey was sent to primary care physicians at a group of walk-in clinics to determine what percentage of their patients with RA were referred to a rheumatologist and, concerning referral patterns, how likely it is they would refer a confirmed or suspected RA patient to a rheumatologist.
Results. Patients with RA referred to rheumatologists in this sample were seen by a rheumatologist at a mean of 9.8 months (median 5 mo, range 0–129 mo) after symptom onset, and mean 1.2 months (median 4.0 mo, range 0–8 mo) after being referred by their primary care physician. All referred patients with confirmed RA were started on DMARD within 1 week of initial consultation. Primary care physicians would refer suspected RA patients 99.5% of the time (median 100, range 90–100%), and 87.6% (median 90, range 50–100%) of patients with confirmed RA would have seen a rheumatologist at least once. A chart review showed that, in a select group of family physicians, 70.9% (22/31) of patients coded as RA per the ICD-9 did indeed have RA and all had seen a rheumatologist for their condition.
Conclusion. In Northern Alberta, patients with RA are seen and started on DMARD therapy in a timely fashion. Most of the delay is at the primary care level, suggesting a need for improved education of patients and primary care physicians rather than a formal triage system.
Rheumatoid arthritis (RA) can lead to substantial pain, disability, and deformity. Recent guidelines encourage early referral to a rheumatologist for patients suspected of having RA, as well as timely initiation of disease-modifying antirheumatic drug (DMARD) therapy. These goals are directed at decreasing inflammation and preventing significant damage to the joints, and thus the longterm sequelae outlined above1,2. It is clear that earlier intervention is more likely to prevent development of erosion1,2.
In countries such as Canada, where a specialist consult is normally preceded by a referral from a primary care practitioner, one can consider the timeline for rheumatology consultation as comprising 3 intervals. The first interval is the period from onset of symptoms to presentation to the family physician, the second is the period from initial presentation to referral to a rheumatologist, and the third is the waiting period for the specialist consultation and subsequent initiation of DMARD therapy.
Data from 2 recent Canadian studies suggest, however, that in addition, a sizable number of patients coded as for RA are not referred to a rheumatologist3,4. There is some evidence that patients with RA under the care of a rheumatologist receive increased quality of care and have better outcomes5,6,7. Prior to the consideration of a triage process, we carried out a partial audit of rheumatology services in Northern Alberta to answer 3 questions with this chart audit and survey: how long after symptom onset are patients with suspected RA referred to rheumatologists; when are DMARD started; and how likely is a patient with confirmed or suspected RA to be referred to a rheumatologist?
MATERIALS AND METHODS
Part 1 – Rheumatologist chart review
Study sample
In this part of our study we focused on the charts of 3 rheumatologists in Edmonton, Alberta (a convenience sample, who volunteered, 2 in an academic setting and 1 in private practice). Records were used to identify patients diagnosed by the consultant rheumatologist as having RA and who had presented for the first time in the decade from July 2000 to July 2010. Time data were obtained from referral letters from the primary care physicians to rheumatologists stating diagnosed/suspected RA, and consultation letters confirming the diagnosis and the institution of DMARD therapy. All the charts of patients with RA were reviewed. In addition, a similar chart review of the only rheumatologist in Calgary not participating in a referral triage process (which might otherwise affect referral times) was performed, and relevant results are discussed.
Data collection and measures
Charts were reviewed with the aim of identifying a number of key intervals and metrics based on information from referral and consultation letters between primary care practitioners and rheumatologists. Data were gathered concerning the date (to the closest month) of the onset of symptoms, the date of the first visit to a primary care physician (generally a family physician) for those symptoms — if available, date of referral to a rheumatologist, the date of the initial consultation with the rheumatologist, the date of receiving a diagnosis of RA by the rheumatologist, and the date of first receiving a prescription for a DMARD. (This did not include steroids, which are rarely used in this region.)
Analysis
To evaluate the timeliness of referrals for patients with RA, the intervals between the various stages in care were calculated as follows. First, the number of months between symptom onset and referral by a family physician was counted as interval 1. The number of months between the date of the referral letter from the family physician and the date of the consultation letter from the rheumatologist counted as interval 2 (and counted as 0 months for any number of days < 30, i.e., greater precision, such as 0.25 months, was not considered valuable). Finally, the sum of interval 1 and 2 (in months) was considered interval 3, the total time between symptom onset and visit to a rheumatologist. Data are reported as mean, median, and range, as they have a non-normal distribution.
Part 2 – Family physician chart review
Study sample and data collection
In this part of our study, charts were reviewed in 2 primary care clinics (total of 4 family physicians) in Grande Prairie, a small urban center in Alberta. The charts of all patients who had been coded in the electronic records as having ICD-9 codes 714 or 714.0 within the past 5 years (RA ± other inflammatory polyarthropathies) were assessed to obtain referral data and dates.
Part 3 – Primary care physician survey
Study sample and data collection
In this part, to assess whether primary care physicians are likely to in fact refer patients with suspected RA or RA to a rheumatologist for further evaluation, an anonymous survey was sent to 30 primary care physicians in Edmonton asking the following 2 questions:
-
In the last 3 years, as best you can recall, what percentage of the patients with RA that you have encountered have seen a rheumatologist at least once?
-
If you were to see a new patient with RA what percentage would you normally refer to a rheumatologist?
The 30 primary care physicians all worked within a walk-in and primary care organization comprising 15 clinics distributed throughout the catchment area. They were thus considered representative for the catchment area. Data are reported as mean, median, and range, as they have a non-normal distribution. Three survey response forms were excluded from the analysis due to incomplete or erroneous data. Sample sizes were not calculated as the surveys were completed on sample populations readily available for study.
RESULTS
Timeliness of referrals to a rheumatologist
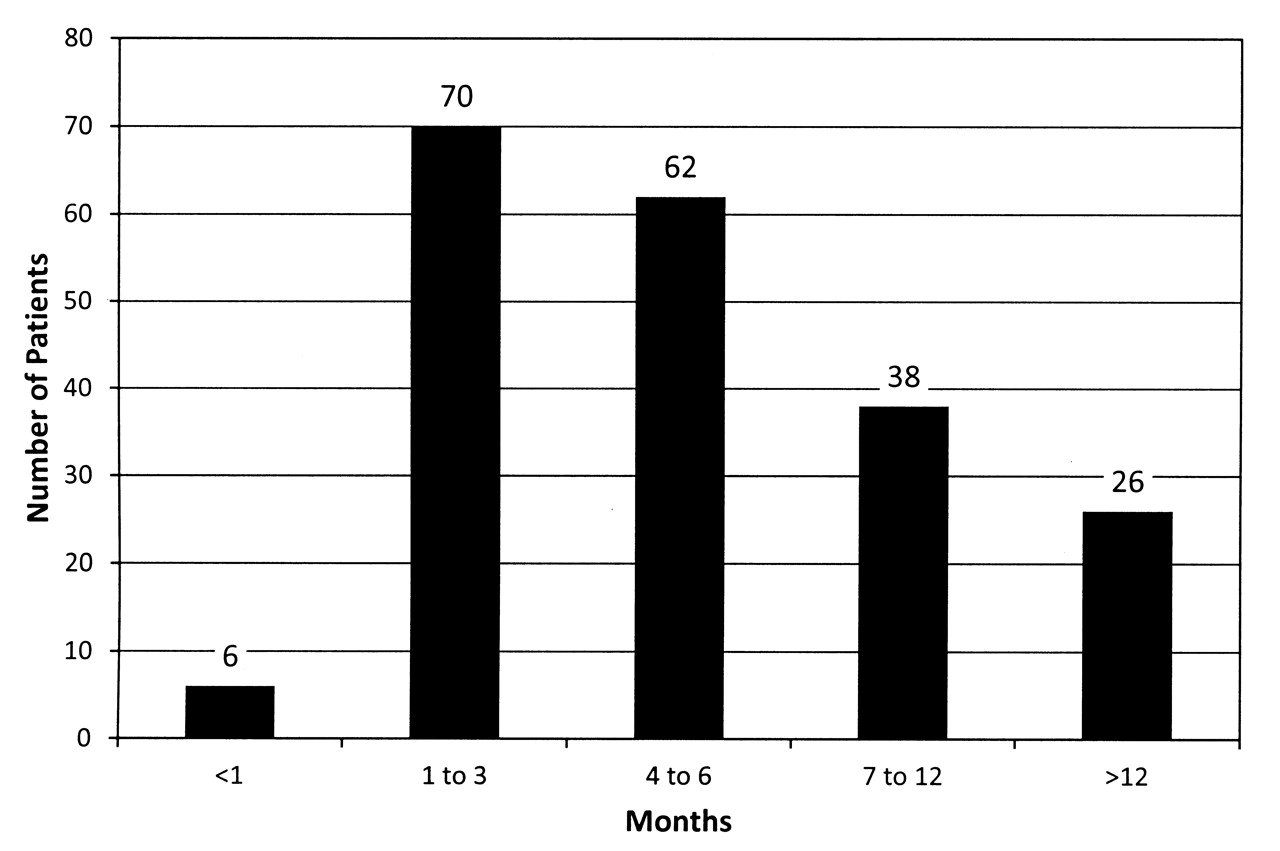
A total of 482 charts were reviewed in Edmonton, Alberta; 151 were included in our study. Reasons for exclusion were as follows: patients who had been first seen by a rheumatologist for RA or suspected RA before 2000 (n = 45) or patients for whom there was not enough information available from the chart to accurately determine timelines relating to referral intervals, diagnosis, and/or treatment (n = 286). There were various reasons why information was not complete, including letters not present in the paper chart or diagnosis made in a different locale. In addition, we evaluated similar unpublished data from Calgary, the other major urban center in Alberta, for comparison. The data were not normally distributed, and thus both means and medians are reported. Using the data from study Part 1 above, patients ultimately seen by a rheumatologist presented to a family doctor a mean of 9.8 months (median 4.0 mo, range 0–128 mo) after first experiencing consistent and regular joint symptoms (Figure 1). On average, these patients were then referred to and seen by a rheumatologist at a mean 1.2 months (median 0.8 mo, range 0–8 mo), with a total mean time between symptoms and rheumatology consultation of 11 months (median 5.0 mo, range 0–129 mo; Figure 2).

Study Part 1. Total time between onset of symptoms and consultation visit with rheumatologist.

Study Part 1. Time between referral by primary care physician and consultation visit with a rheumatologist.
These data are in keeping with similar numbers (collected by author MC) from an in-progress study in Calgary, the major urban center in Southern Alberta. There, the mean wait time for the same interval (from symptom onset to rheumatologist visit) is 12.5 months, a difference of 1.5 months, with 87.1% of patients having been seen within 12 months (Figure 3).
Study Part 1. Total time between onset of symptoms and consultation visit with a rheumatologist, data from Calgary, Alberta.
Timeliness of institution of DMARD therapy
Of the 151 patients reviewed in this part of our study, 149 (98.6%) received a prescription for DMARD at the time of the initial consultation for RA, irrespective of whether the diagnosis was confirmed at that visit or was merely highly suspicious and diagnosed later. The remaining 2 patients received DMARD within 1 week of the initial consultation.
Accuracy of coding for RA
Part 2 of the study looked at all patients coded with RA in the electronic records of 4 family physicians in a smaller urban center. All 31 patients so coded had been referred to a rheumatologist. His charts showed that patients coded with a diagnosis of RA (714 or 714.0 depending on individual practice preferences), of which 22 (70.9%) truly had RA, and that 9 either did not have RA (n = 7) or the diagnosis was in question (n = 2). The alternative diagnoses of those who did not have RA included psoriatic arthritis, juvenile idiopathic arthritis, and polymyalgia rheumatica; however, all patients with this code had been seen by a rheumatologist.
Referral practices of family doctors
Parts 2 and 3 of the study examined the referral practices of primary care physicians with respect to suspected cases of RA. In Part 2, the results showed that all 31 patients coded as having RA and who were being followed by any of 4 family physicians in a small urban center in Alberta had been referred to a rheumatologist at least once, and in all cases the diagnosis had been confirmed by a rheumatologist, regardless of whether the final diagnosis was indeed RA or a different condition (see results above).
Further, data from Part 3 of the study, surveying the referral pattern of primary care physicians, indicated that, on average, 87.6% (median 90, range 50–100%) of their patients with RA had seen a rheumatologist at least once, and that the practitioners would refer patients with suspected RA to a rheumatologist 99.5% (median 100, range 90–100%) of the time. The response rate to this faxed, anonymous survey was 24/30 (80%). As discussed above, 3 survey response forms were excluded, bringing the total number included in the analysis to 21, thus bringing the proportion of usable responses to 70%.
DISCUSSION
Our study shows that, in Northern Alberta, patients with suspected RA wait a mean of 11 months from symptom onset to first consultation visit with a rheumatologist. As noted in Figure 3, these data are similar to the overall delay for the Calgary rheumatologist studied. At least in Edmonton, it appears that these patients are referred and seen by a rheumatologist in a timely manner once they present with symptoms suggestive of RA, consistent with earlier studies8,9. For comparison, a similar review carried out in Quebec showed a similar average referral wait time of 34.6 days for those patients who were eventually found to have an inflammatory arthritis4. Further, these patients are overwhelmingly almost immediately started on appropriate DMARD therapy once seen by a rheumatologist, a trend noted in a similar study with data from Toronto, Ontario10. These data contrast with those from studies from other Canadian centers, where it was reported that DMARD use by rheumatologists ranges from 58% to 84%3,10. Whether this reflects regional differences or an increased use of DMARD in more recent years remains unclear.
A system of referral triage has been initiated in many centers in an effort to improve timeliness of referrals and the quality of referral information. This process has been in place in Edmonton for the last year, and of the 3 consultant rheumatologists in the study, only 1 is currently participating. Further, the data presented here from Calgary were obtained from the charts of a rheumatologist not participating in that city’s referral triage system. The results, however, suggest that any delay in presentation may not necessarily be due to the referral/consultation process, but rather at the initial presentation to primary care. The reasons patients might delay presenting with arthritis symptoms to their primary care doctor are likely multiple, including, in some areas, a lack of primary care physicians.
There are a number of limitations to our study. One is that we were able to indirectly address the question of patients with significant RA not seeing a rheumatologist. In addition, of the total patients with RA reviewed, fewer than half the records included data required to accurately determine time-lines, but these were seen equally in charts from all 3 rheumatologists.
The survey of family physicians to determine probability of referring a suspected or confirmed patient with RA does not confirm what these physicians actually do in practice. Not all general practitioners were sampled, and we chose to sample from a group of walk-in clinics, without confirmation of how representative the referral practices are in these clinics compared to others in Northern Alberta. The survey of rheumatologist charts is limited to 151 confirmed cases of RA. As part of the study was also a chart review, we used the recorded description by the patients of their symptom duration prior to referral. It may also be that some of those patients who described symptoms for over 1 year before seeking attention had symptoms from other causes (such as myofascial pain, osteoarthritis, etc.) with which they were coping without medical care. Further, they may have had palindromic attacks of eventual inflammatory arthritis, which at first may have spontaneously remitted.
Previous results from the Canadian province of British Columbia indicate that over a 5-year period, only 48% of patients with suspected RA ever see a rheumatologist for their condition3. Data from Quebec province suggest an even lower rate, 27.3% being seen by a rheumatologist over the next 3.5 years, once diagnosed, with a median time to visit of 79 days for those consulted11. Our survey of primary care physicians in the Edmonton area suggests that referral practices in Northern Alberta might be different, as primary care physicians answered that they would refer a case of suspected RA to a rheumatologist 95.4% of the time. This contrasts with earlier published data, again from the province of Quebec, where family physicians in a similar survey suggested they would refer patients with suspected RA only 77.5% of the time12. Our survey was sent anonymously to primary care physicians practicing in facilities that also function as walk-in clinics. The data from the small number of surveys distributed, as well as this type of practice pattern, may not represent the referral patterns of family physicians throughout Northern Alberta.
However, our results do appear to be consistent with clinical practice, as all patients coded as having RA (irrespective of the true clinical diagnosis) from 4 family physicians in a small urban center had seen a rheumatologist at least once for their condition. The accuracy of coding of these patients as actually having RA appears to be consistent with previous data, as it was previously reported that computer databases for diagnosis of RA (i.e., clinical medial records) have a sensitivity of 89%, specificity of 74%, and that the agreement between databases and medical record review was poor (kappa = 0.54)13. Although coding accuracy is not perfect, it is reassuring that all RA-coded patients had seen a rheumatologist in consultation and would presumably have had appropriate management for their condition regardless of whether it was RA or a different diagnosis.
We were not able to directly address the question of patients with significant RA not seeing a rheumatologist. Nevertheless, we hypothesized that if this were so, then we should, as rheumatologists, be seeing patients who have had diagnosed (and therefore coded) but unreferred RA for many years. Of the 151 patients included in this study, none fit this description, and this was also true for Calgary patients.
Overall, our results suggest that, despite data from other Canadian centers indicating that patients with RA may not be referred to or seen by consultant rheumatologists as often or as quickly as guidelines recommend, this does not seem to be the case in Northern Alberta (and likely Alberta as a whole). Most patients referred to a rheumatologist are seen in a timely manner (within 3 months of referral). The fact that most of the delay in consultation appears to be prior to healthcare utilization suggests that greater education of the public and of family physicians is necessary to ensure more prompt referral of symptomatic patients. We were not able to delineate how much of that delay was due to patient delays in presentation and how much was due to delay in recognition of early arthritis by the primary care provider. The use of validated clinical decision-making tools may potentially be one avenue to aid in the screening and identification of patients with possible RA at the primary care level14,15.
Acknowledgment
We are grateful to Dr. H. Niall Jones for participating in this audit.
- Accepted for publication November 9, 2011.








{kind=link}
{kind=link}
{kind=link}