

Abstract
Objective. To describe clinical fracture rates, back pain, and health-related quality of life (HRQOL) in postmenopausal women with osteoporosis who are receiving glucocorticoids (GC), during a 36-month study of teriparatide treatment for up to 18 months, with an additional 18-month followup period when patients were receiving other osteoporosis medications.
Methods. A prospective, multinational, observational study. Data for clinical fractures, back pain (by visual analog scale; VAS) and HRQOL (by EQ-5D) were collected over 36 months. Fracture data were summarized in 6-month segments and analyzed using logistic regression with repeated measures. Changes from baseline in back pain VAS and EQ-VAS were analyzed.
Results. Of 1581 enrolled women with followup data, 294 (18.6%) had antecedents of GC use. Of these, 49 (16.7%) patients sustained a total of 69 fractures during the 36-month study period. Adjusted odds of fracture were significantly decreased during the last year of followup compared with the first 6 months of teriparatide treatment: an 81% decrease in the 24 to < 30-month period (p < 0.05), and an 89% decrease in the 30 to < 36-month period (p < 0.05). There were significant reductions in back pain and improvements in HRQOL in both groups of GC users and nonusers.
Conclusion. Postmenopausal women with severe osteoporosis receiving GC, who were treated with teriparatide for up to 18 months, showed a reduced incidence of clinical fractures during the third year while receiving sequential osteoporosis treatments compared with the first 6 months, together with reduced back pain and improved HRQOL. Our results should be interpreted in the context of an uncontrolled observational study in a routine clinical setting.
Glucocorticoids (GC) are potent antiinflammatory and immunosuppressive agents widely used for the treatment of diseases including chronic lung disease, rheumatoid arthritis (RA) and other connective tissue diseases, and inflammatory bowel disease and after transplantation. GC use, however, is associated with adverse effects including rapid bone loss leading to osteoporosis and an increased risk of fracture1. Glucocorticoid-induced osteoporosis (GIO) is the most common cause of secondary osteoporosis and fractures, which may occur in 30% to 50% of patients receiving chronic GC therapy1. The mechanisms underlying GC-induced deterioration of bone quality differ from those in postmenopausal osteoporosis, and affect predominantly osteoblasts and decreased bone formation2,3. The negative effect of GC on bone quality is also reflected by the higher risk of fractures in GC users than nonusers with a similar level of bone mineral density (BMD)4, indicating that the increase in fracture risk in GC users is at least partly independent of BMD.
Teriparatide [recombinant human parathyroid hormone (1–34)] is a bone anabolic agent approved for the treatment of postmenopausal women and men with severe osteoporosis who are at high risk of fracture. Evidence from a randomized, double-dummy, active-controlled trial showed that teriparatide treatment of men and women with GIO resulted in greater gains in lumbar spine BMD and fewer new vertebral fractures, compared with alendronate therapy, after 18 and 36 months of treatment5,6. Although randomized controlled trials (RCT) are considered the “gold standard” for evaluating drug efficacy, the design of such studies limits the generalizability of their findings to everyday clinical practice7. Therefore, the conclusions of RCT can be complemented by observational studies, because their findings may have wider applicability to the patient population treated in regular clinical practice.
The effectiveness of teriparatide in regular clinical practice has been evaluated in the European Forsteo Observational Study (EFOS), a 36-month prospective observational study in the outpatient setting, designed to evaluate fracture outcomes, back pain, and health-related quality of life (HRQOL) in post-menopausal women with severe osteoporosis8. The aim of our predefined analysis was to describe the baseline characteristics, fracture outcomes, back pain, and HRQOL in the subgroup of EFOS patients who were concomitantly treated with GC at any time during the study (i.e., at baseline or at any time during the 36-month followup). We describe these outcomes both during active treatment with teriparatide for up to 18 months and in the subsequent 18-month followup period after teriparatide was discontinued, when most patients were receiving other osteoporosis medications.
The changes in clinical fracture risk, back pain, and HRQOL during the up to 18-month teriparatide treatment period and the 18-month followup period for the total study cohort have been reported previously9,10.
MATERIALS AND METHODS
Patients
Postmenopausal women with a diagnosis of osteoporosis who were about to initiate teriparatide treatment according to the clinical judgment and usual practice of the participating physicians were enrolled in EFOS, a multicenter, prospective, observational study conducted in 8 European countries (Austria, Denmark, France, Germany, Greece, Ireland, The Netherlands, and Sweden). Participating physicians specialized in the treatment of osteoporosis and its complications. Teriparatide treatment (20 μg once daily by self-administered subcutaneous injection; Forsteo, Eli Lilly, Windlesham, UK) was initiated at the baseline visit. Patients were followed for the duration of their teriparatide treatment, which they could discontinue at any time, with followup visits at 3, 6, 12, and up to 18 months after initiation of teriparatide. Patients were asked to return for 2 additional visits at about 6 and 18 months after discontinuing teriparatide treatment.
Patients were excluded from the study if they were currently being treated with an investigational drug or procedure, or had any contraindications as described in the teriparatide product label11. There were no further restrictions regarding patient selection. All study participants provided written informed consent prior to enrollment and were able to withdraw at any time without any consequences in their medical attention. The study was approved by local ethics committees or review boards, depending on local requirements, and was conducted from April 2004 (first patient enrolled) until February 2009 (last patient completed) in accord with the ethical standards of the Declaration of Helsinki. The study design and characteristics of the EFOS patient population have been described in detail8.
Assessments
Patient demographic characteristics, risk factors for osteoporosis and falls, drugs related to the risk of osteoporosis (including GC), and disease status were recorded at the baseline visit8. The number and type of previous and current medications for the treatment of osteoporosis were recorded. Diagnosis of osteoporosis was based upon axial or peripheral dual x-ray absorptiometry measurements of BMD and was confirmed following review of medical reports by the treating physician. Incident clinical vertebral and nonvertebral fragility fractures during the observational period were diagnosed and confirmed by review of the original radiographs and/or the radiology or surgical reports at the investigational site. A new or worsened clinical vertebral fracture was defined as the presence of a confirmed radiographic vertebral fracture associated with signs and/or symptoms suggestive of vertebral fracture(s)12.
Back pain was self-assessed by patients at each study visit using a 100-mm visual analog scale (VAS), ranging from 0 = no back pain to 100 = worst possible back pain. Patients also completed a back pain questionnaire that recorded the frequency and severity of back pain, limitations of activities, and days in bed due to back pain in the previous month9.
HRQOL was measured at each visit using the European Quality of Life Questionnaire (EQ-5D)13, where patients assess their perceived overall health status on a VAS (EQ-VAS) that ranges from 0 (worst imaginable health state) to 100 (best imaginable health state), and classify their own health status according to 5 dimensions of health (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each of which is scored on a 3-point scale (no problems, some problems, or extreme problems). The Health State Value (HSV) was calculated from the 5 EQ-5D dimensions using the UK scoring algorithm to allow comparisons among countries14.
Statistical analysis
For data analyses, the total study cohort included all patients with a baseline visit and at least 1 followup visit. The post-teriparatide cohort included those patients who discontinued teriparatide at any time between baseline and 18 months and had at least 1 post-teriparatide followup visit. Patients were categorized as being GC users or nonusers. Patients in the GC user group were those who were taking GC at the baseline visit or at any time during the study.
Descriptive statistics, such as frequencies, percentages, means, SD, and ranges, were used to describe the GC user and nonuser groups. Between-group comparisons were made using chi-square or Fisher’s exact tests (categorical variables) or the Kruskal-Wallis test (continuous variables).
The number of fractures occurring in GC users and nonusers was summarized in 6-month periods. For each group, a logistic regression with repeated measures was used to assess the change in number of patients with 1 or more fractures over time15,16, giving an analysis of the odds of 1 or more fractures. Patients were included in the model at all observed periods, regardless of whether they had experienced a fracture during a previous period. The repeated observations of each patient were assumed to be related, but no further assumptions were made about the relationship. Unadjusted and adjusted analyses were performed that included age, prior bisphosphonate use, and fracture in the last 12 months before starting teriparatide. Contrasts were made between the odds of fracture in the first 6 months of treatment (0 to < 6 months) and each subsequent 6-month interval.
Back pain and HRQOL were summarized over the teriparatide treatment period and after teriparatide discontinuation for the GC user and nonuser groups. Changes in back pain VAS from baseline were analyzed using a mixed model of repeated measures (MMRM), adjusting for back pain VAS at baseline, number of previous fractures, age, diagnosis of RA, duration of previous bisphosphonate therapy, and history of fracture in the 12 months before entering the study. Variables analyzed using the sign test were the number of patients reporting an improvement, no change, or worsening from baseline in the severity of back pain, frequency of back pain, and limitation of activities due to back pain. The median change from baseline in the number of days in bed due to back pain was analyzed using the Wilcoxon signed-rank test.
A similar MMRM was used to assess the change from baseline in EQ-VAS, including its baseline value. The number of patients reporting an improvement, no change, or worsening from baseline in each of the 5 EQ-5D domains was analyzed using the sign test. Changes from baseline in EQ-5D HSV were assessed using the Wilcoxon signed-rank test because this parameter has a nonparametric distribution.
RESULTS
Patient disposition and characteristics
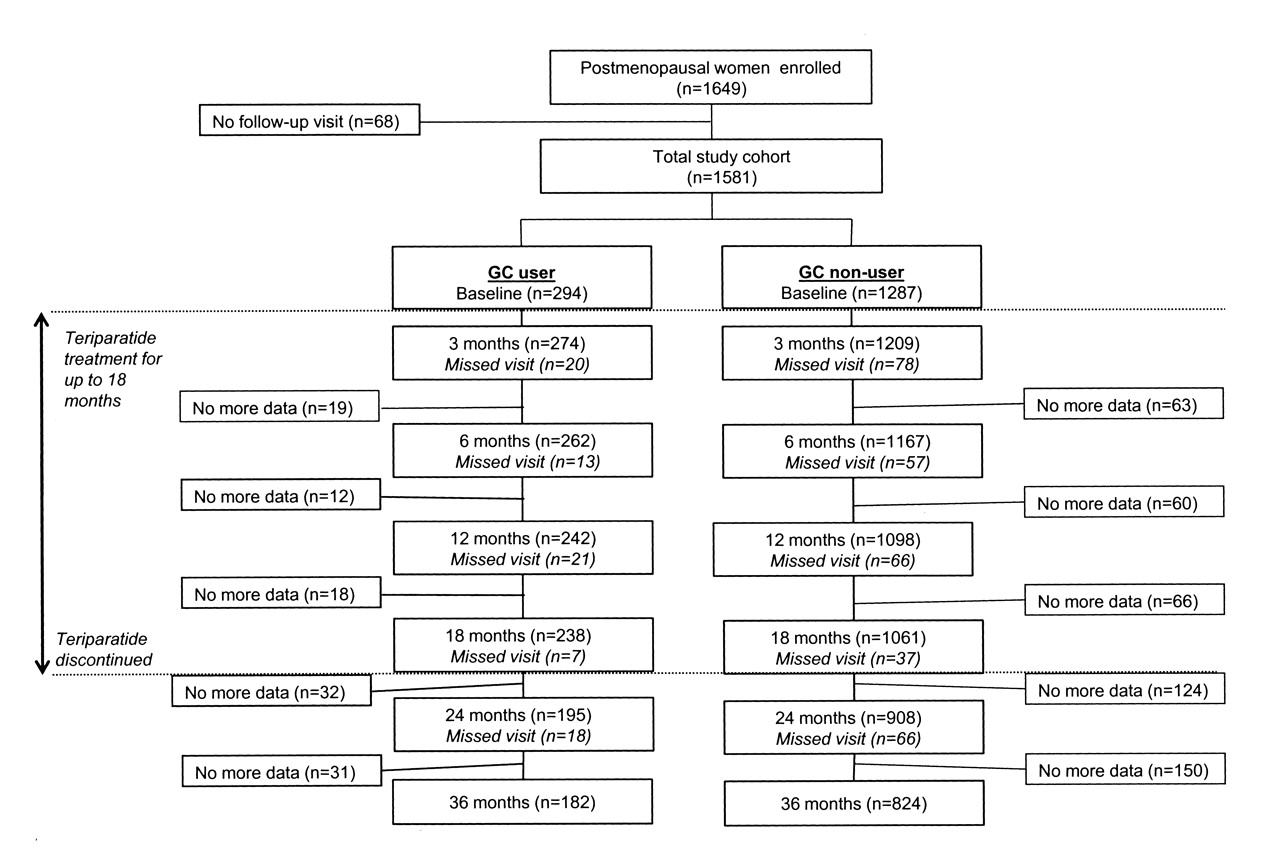
A total of 1649 post-menopausal women were enrolled in EFOS, and 1581 had a baseline visit and at least 1 postbaseline visit (the total study cohort). Of these 1581 patients, 294 (18.6%) were GC users and 1287 (81.4%) were GC nonusers. Figure 1 shows the patient disposition over the course of the study for GC user and nonuser groups.
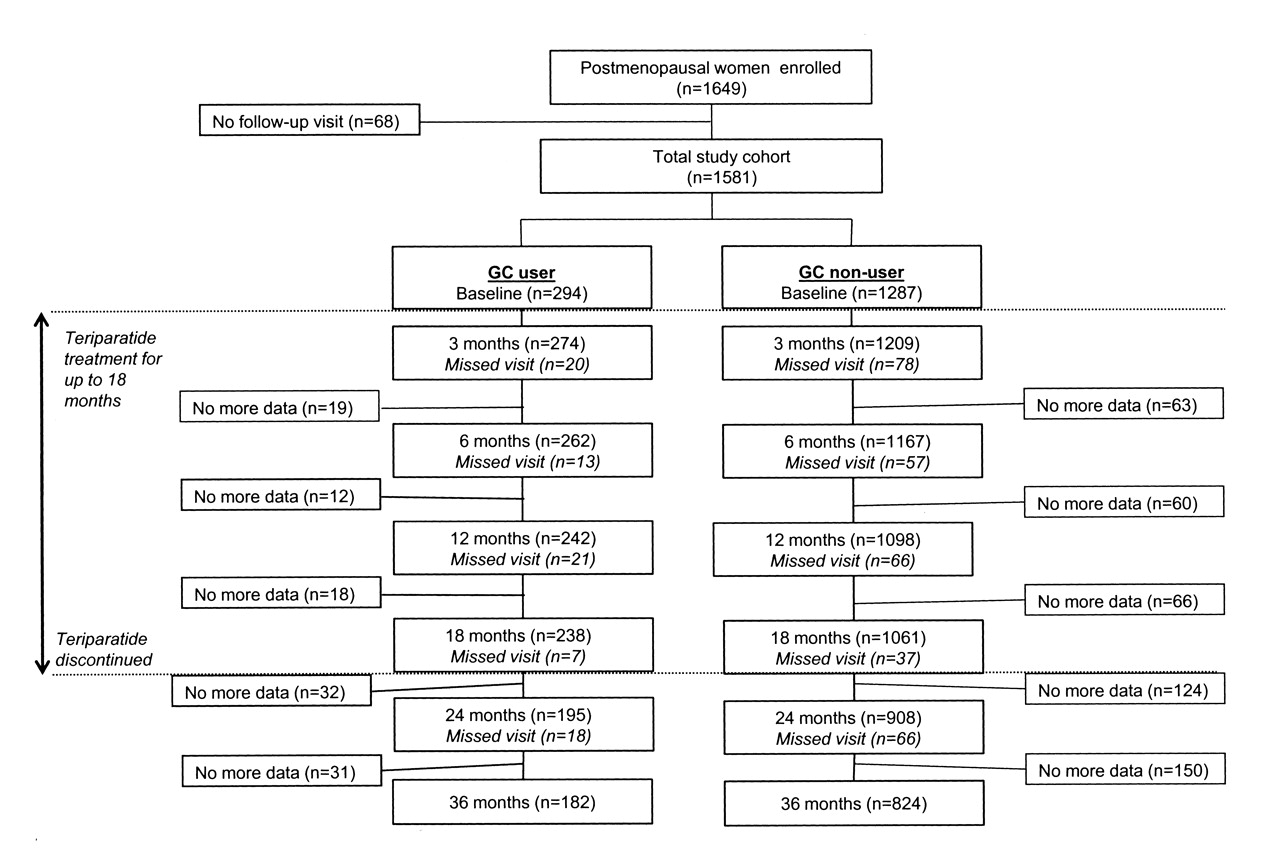
Patient disposition, representing the total study cohort: all patients with a baseline visit and at least 1 post-baseline visit. GC: glucocorticoid.
The demographic and baseline characteristics of the GC users and nonusers are summarized in Table 1. Compared with the GC nonuser group, the GC user group was younger, had a higher frequency of surgical menopause, a higher lumbar spine BMD T score, a higher frequency of previous bisphosphonate use, and more frequent need to use their arms when standing up from a chair (Table 1). In addition, a significantly higher percentage of patients in the GC user group had RA, chronic obstructive pulmonary disease, or chronic hepatopathy, and were taking concomitant chronic medications such as antihypertensives, benzodiazepines, antiarrhythmics and anti-depressants (Table 1). At baseline, the GC user group had a lower HRQOL as indicated in a significantly lower mean EQVAS and median EQ-HSV compared with the GC nonuser group (Table 1).
Baseline characteristics of glucocorticoid (GC) users and nonusers.
Teriparatide treatment and osteoporosis medications after teriparatide treatment
The median duration of teriparatide treatment was similar in the GC user and nonuser groups: 545 days (Q1, Q3: 503, 554) and 542 days (Q1, Q3: 520, 555), respectively. Persistent use of calcium and vitamin D throughout teriparatide treatment was reported by 74.7% of the GC users and 68.2% of GC nonusers.
After teriparatide was discontinued, there were 156 GC users and 753 GC nonusers in the post-teriparatide cohort. The majority of GC users took osteoporosis medication after teriparatide (n = 149, 95.5%): 109 (69.9%) took any antiresorptives, mainly bisphosphonates (n = 96, 61.5%). Other antiresorptives were used much less frequently after teriparatide was discontinued and included estrogens or raloxifene (8.3%) and calcitonin (5.1%). Calcium and vitamin D were widely used after teriparatide was stopped in the GC users (89.7% and 87.8% of patients, respectively). Similarly, 706 (94.0%) of the GC nonusers took osteoporosis medication after teriparatide: 532 (70.8%) took any antiresorptives, mainly bisphosphonates (n = 478, 63.6%). The use of other antiresorptives and of calcium and vitamin D was similar to the GC users group.
Fracture outcomes
The incidence of fractures during teriparatide treatment (0 to < 18 months) and after teriparatide was discontinued (18 to < 36 months, when most patients were receiving other osteoporosis medications) in the GC user and nonuser groups is shown in Table 2. In the GC user group, 49 (16.7%) women sustained 1 or more fractures during the 36-month study period. Of the 69 fractures, 21 (30.4%) were vertebral, and 48 (69.6%) were nonvertebral: 38 (55.1%) of all fractures were main nonvertebral fractures at the humerus (n = 12), leg (n = 9), hip (n = 8), forearm/wrist (n = 7), and sternum/ribs (n = 2). Table 2 shows a significant decrease in the adjusted odds of fracture in the last 2 time periods compared with the first 6 months of teriparatide treatment (0 to < 6 months), i.e., the decrease was 81% in the 24 to < 30-month period and 89% in the 30 to < 36-month period after teriparatide had been discontinued.
Fracture incidence during teriparatide treatment (0 to < 18 months) and after teriparatide was discontinued [(18 to < 36 months) in glucocorticoid (GC) users and nonusers (total study cohort)]. The shaded section covers the period from 18 to < 36 months’ followup when teriparatide had been discontinued and the majority of patients were receiving other osteoporosis medications.
To determine whether changes in GC use during followup may have influenced the incidence of fractures, we performed a posthoc analysis repeating the logistic regression model but adding current GC use during each 6-month period as a time-varying covariate. As for the predefined analysis, the adjusted odds of fracture were significantly decreased (compared with the first 6-month period) during the last year of followup, i.e., there was an 88% decrease in the 24 to < 36-month period (p = 0.003) and a 94% decrease in the 30 to 36-month period (p = 0.004).
In the GC nonuser group, 159 (12.4%) women sustained 1 or more fractures during the study. Of the 189 fractures, 66 (34.9%) were vertebral and 123 (65.1%) were nonvertebral; 91 (48.1%) of all fractures were main nonvertebral fractures at the forearm/wrist (n = 34), hip (n = 19), sternum/ribs (n = 17), leg (n = 12), and humerus (n = 9). Table 2 shows a significant decrease in the adjusted odds of fracture for GC nonusers at every time period, compared with the first 6 months of teriparatide treatment (0 to < 6 months).
The adjusted odds of fracture were significantly higher in the GC user group at 6 to < 12 months (OR 2.26, 95% CI 1.20–4.18, p = 0.007), 12 to < 18 months (OR 2.12, 95% CI 1.08–4.15, p = 0.029), and 18 to < 24 months (OR 2.48, 95% CI 1.20–5.10, p = 0.014), compared with the GC nonuser group.
Table 3 summarizes the incidence of clinical fractures after teriparatide discontinuation in the GC users and nonusers (the post-teriparatide cohort). There was a significant reduction in the clinical fracture rates during the last 12 months of followup for GC users only.
Fracture incidence after teriparatide was discontinued in glucocorticoid (GC) users and nonusers (post-teriparatide cohort).
A posthoc analysis repeating the logistic regression model but adding current GC use during each 6-month period as a time-varying covariate in the GC user group gave results similar to those in Table 3. Compared with the first 6 months after teriparatide was discontinued (0 to < 6 months), there was a significant decrease in the adjusted odds of fracture at 6 to < 12 months (OR 0.08, 95% CI 0.01–0.57, p = 0.012) and 12 to < 18 months (OR 0.07, 95% CI 0.01–0.46, p = 0.005) after teriparatide discontinuation.
Back pain
Figure 2 shows significant reductions in adjusted mean back pain VAS scores from baseline at each postbaseline visit in both the GC user and nonuser groups, with no significant differences between the groups. Similar results were obtained when the model was repeated including GC use as a time-varying covariate (data not shown). Results from the back pain questionnaire show significant reductions from baseline in back pain frequency and severity, limitations of activities due to back pain, and number of days in bed due to back pain during teriparatide treatment in both the GC user and nonuser groups (Table 4). These changes were maintained after teriparatide was discontinued. The only differences seen between the GC user and nonuser groups were a greater change in severity of back pain and fewer days in bed due to back pain after teriparatide was discontinued in the GC nonuser group (Table 4).
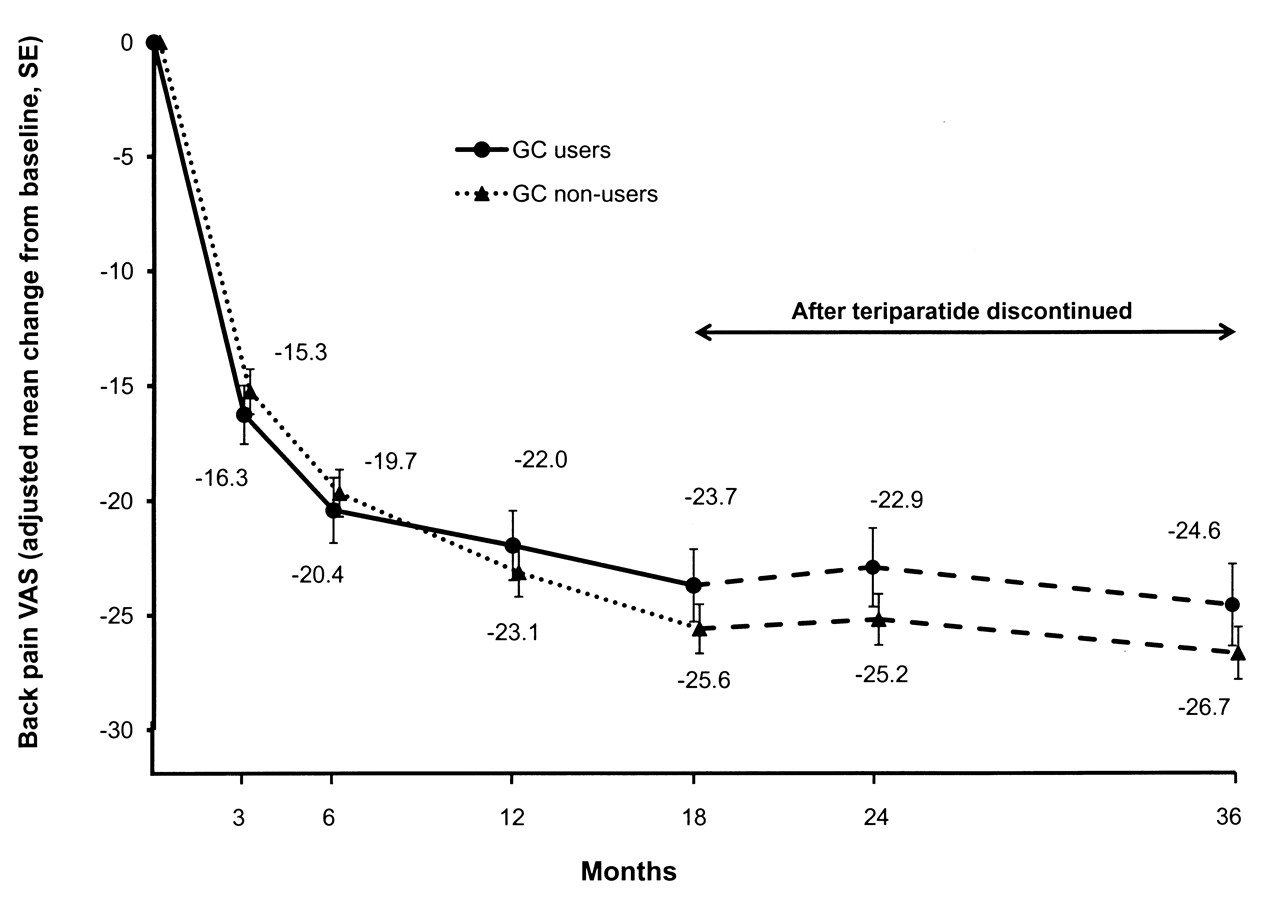
Adjusted mean change in back pain visual analog scale (VAS) from baseline during treatment and after teriparatide discontinuation in glucocorticoid (GC) users and nonusers. Model includes baseline back pain VAS score, number of previous fractures, fracture in 12 months before study entry, age, duration of previous bisphosphonate use, and diagnosis of rheumatoid arthritis. The unadjusted mean back pain VAS scores at baseline, 3, 6, 12, 18, 24, and 36 months and end of study (last observation carried forward) for the GC users were 58.4 (SD 27.4), 42.5 (SD 25.4), 37.9 (SD 25.9), 35.3 (SD 26.4), 32.8 (SD 26.1), 32.9 (SD 28.1), 31.3 (SD 27.6), and 36.9 (SD 28.8), respectively. For the GC nonuser group, the corresponding unadjusted mean scores were 57.6 (SD 26.4), 43.0 (SD 24.9), 38.4 (SD 25.3), 34.5 (SD 25.5), 31.7 (SD 25.4), 31.9 (SD 26.4), 28.8 (SD 26.0), and 32.7 (SD 26.9). Between-group difference for the unadjusted scores was significant only for end of study (p = 0.02, 2-sample t test). The unadjusted mean change from baseline to endpoint for the GC users and nonusers was −22.0 (SD 34.9) and −24.8 (SD 31.2), respectively. All values p < 0.001 versus baseline. SE: standard error.
Back pain questionnaire results for glucocorticoid (GC) users and nonusers. Total number varies for each variable due to missing data. Percentages given for each variable refer to the total number available for that variable.
Health-related quality of life
Figure 3 shows a significant improvement from baseline in EQ-VAS in both the GC user and nonuser groups at all postbaseline visits. The increase in EQ-VAS was significantly higher in the GC nonuser group than in the GC user group at the 12-month visit only. Results similar to those in Figure 3 were obtained when the model was repeated including GC use as a time-varying covariate (data not shown). The percentage of GC users and nonusers reporting some/extreme problems for each of the 5 EQ-5D domains is summarized in Table 5. There were significant improvements from baseline (p < 0.001, sign test) in all 5 domains during teriparatide treatment that were maintained after teriparatide was discontinued.
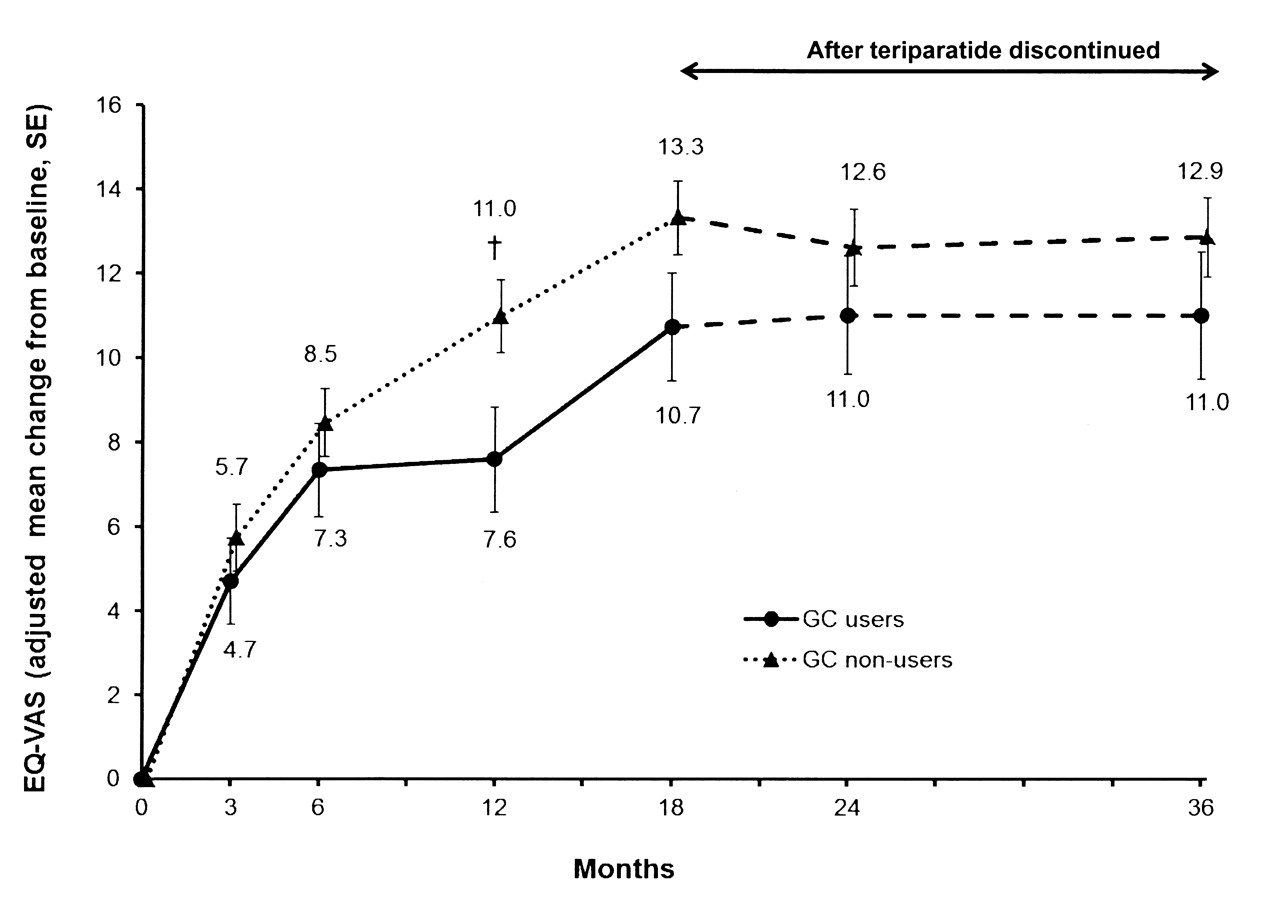
Adjusted mean change in European Quality of Life Questionnaire visual analog scale (EQ-VAS) from baseline during treatment and after teriparatide discontinuation in glucocorticoid (GC) users and nonusers. Model includes baseline EQ-VAS score, number of previous fractures, fracture in 12 months before study entry, age, duration of previous bisphosphonate use, and diagnosis of rheumatoid arthritis. For GC users, unadjusted mean EQ-VAS values at 0, 3, 6, 12, 18, 24, and 36 months and end of study (last observation carried forward) were 48.8 (SD 22.2), 55.7 (SD 19.2), 58.9 (SD 20.9), 59.8 (SD 22.4), 63.5 (SD 22.1), 63.6 (SD 24.5), 64.8 (SD 24.2), and 60.0 (SD 24.3), respectively. The corresponding values for the GC nonuser group were 52.8 (SD 21.9), 59.7 (SD 19.9), 62.6 (SD 19.8), 65.6 (SD 21.1), 68.3 (SD 21.1), 68.2 (SD 21.9), 69.6 (SD 22.0), and 65.9 (SD 22.9). Between-group difference for the unadjusted scores was significant at every timepoint (p < 0.05, 2-sample t test). The unadjusted mean change from baseline to endpoint was 12.1 (SD 28.7) and 12.9 (SD 26.2) in the GC user and nonuser groups, respectively. All values p < 0.001 versus baseline. †p < 0.05 versus GC user group.
Percentage of glucocorticoid (GC) users and nonusers reporting problems (some/extreme) in each of the EQ-5D domains. Number varies for each variable and at each timepoint due to missing data. Percentage given for each variable refers to the total number available for that variable.
In the GC user group, median (Q1, Q3) HSV values were significantly increased (p < 0.001, Wilcoxon signed-rank test) from baseline at all postbaseline visits and were 0.689 (0.516, 0.796) at 18 months and 0.691 (0.516, 0.812) at 36 months. The same was seen in the GC nonuser group, where the median (Q1, Q3) HSV values were 0.725 (0.620, 0.848) and 0.760 (0.587, 1.000) at 18 and 36 months, respectively.
DISCUSSION
The results of this subgroup analysis of the EFOS study showed that postmenopausal women with severe osteoporosis receiving GC, who were treated with teriparatide for up to 18 months in a routine clinical setting, had a reduced incidence of clinical fractures during the third year of observation, when the majority of them received subsequent treatment with calcium, vitamin D, and antiresorptive drugs. This finding was accompanied by reduced back pain and improved HRQOL during teriparatide treatment that was maintained after the drug was discontinued. The clinical characteristics of the patients enrolled in the EFOS study show that both groups of GC users and nonusers who were treated with teriparatide had severe osteoporosis, a highly impaired HRQOL, and were at very high risk of further fractures as indicated by their risk profiles at baseline. A high proportion of patients in both groups had previously used bisphosphonates, which was expected because bisphosphonates are routinely used as first-line treatment for postmenopausal osteoporosis. Although we did not collect the reasons for initiating teriparatide in our study, most of the treatment guidelines in the participating countries indicate that teriparatide can be used as a second-line treatment for severely osteoporotic patients who do tolerate or have contraindications to other osteoporosis medications, or who have sustained new fractures while taking other osteoporosis medications. However, in some countries teriparatide can be used as first-line therapy in patients with severe osteoporosis.
We performed a subgroup analysis based on GC use because it has been well established that treatment with GC significantly increases the risk for fragility fractures, especially in postmenopausal women17,18. Moreover, although both GIO and postmenopausal osteoporosis lead to bone loss and increased fracture risk, these bone metabolic disorders differ in their pathophysiological mechanisms2,3,19. Thus, chronic exposure to GC has various direct and indirect effects on bone tissue, with a primary effect on lowering bone formation due to inhibition of the differentiation, activity, and lifespan of the osteoblasts and osteocytes1,3,20. In contrast, postmenopausal osteoporosis is mainly characterized by an accelerated bone turnover secondary to an increased rate of bone resorption due to osteoclast hyperactivity that is not compensated for by adequate bone formation to maintain a normal bone balance. The histomorphometric analysis of biopsies from individuals receiving GC shows a greater reduction in bone formation at the cellular and tissue level compared with that noted in postmenopausal osteoporosis21. Moreover, it has been suggested that the combination of GC therapy in osteoporotic subjects receiving longterm treatment with potent antiresorptive drugs, such as bisphosphonates, may increase the risk for atypical subtrochanteric and diaphyseal femoral fractures22,23. Based on the pathophysiology of GIO, it has been suggested that pharmacological agents that stimulate bone formation and accelerate remodeling may be a more appropriate treatment option than antiresorptive agents for patients with GIO at high risk for fracture5,24,25.
Teriparatide has a number of pharmacological effects that could counteract the main mechanisms of GC-induced bone loss. It increases the differentiation of bone lining cells and preosteoblasts into osteoblasts, enhances osteoblast function, and decreases osteoblast and osteocyte apoptosis26,27,28,29, resulting in an improvement of the microarchitectural properties of the bone and an increase in its strength30,31.
In a recent RCT in patients with GIO, Saag, et al5 showed that 18 months of teriparatide treatment resulted in a greater increase in BMD than alendronate treatment. Significantly fewer subjects had new vertebral fractures in the teriparatide group compared with the alendronate group (0.6% vs 6.1%, respectively; p = 0.004), while the incidence of nonvertebral fractures was similar in both groups (5.6% vs 3.7%; p = 0.36). In the subgroup of postmenopausal women with GIO, increases from baseline in lumbar spine BMD were significantly greater in the teriparatide group compared with the alendronate group (7.8% vs 3.7%; p < 0.001)32. In addition, there were fewer new vertebral fractures in the teriparatide group (0.9% vs 5.4% in the alendronate group; p = 0.05), and the incidence of nonvertebral fractures was similar in both groups (6.7% vs 4.2%; p = 0.36)32. On the basis of this RCT, the recently published American College of Rheumatology 2010 guidelines for the prevention and treatment of GIO now recommend teriparatide as an alternative treatment option to oral or intravenous bisphosphonates for patients at high risk of fracture33.
Observational studies can complement RCT because they provide information on the use and effectiveness of treatments in routine clinical practice. EFOS was conducted in a naturalistic setting without randomization to treatment and included a broader range of patients than those included in the pivotal RCT with teriparatide5,34.
Although it is difficult to compare the results of this observational study with the phase III RCT of teriparatide versus alendronate in GIO5,32, our findings suggest that in routine clinical practice in the European countries represented in EFOS, teriparatide is used in patients at higher risk than the population included in the RCT5. Compared with the subgroup of postmenopausal women included in the RCT32, GC users in EFOS were older (69.9 vs 61.9 years), had a lower lumbar spine T score (−3.1 vs −2.7), and had a higher frequency of prevalent vertebral fractures (85% vs 39%). Of note, we observed that in normal clinical practice, despite the current recommendations for calcium and vitamin D supplementation in GIO35, more than one-quarter of GC users did not consistently take these supplements during teriparatide therapy.
The results of our study revealed that the rapid improvements from baseline in HRQOL and back pain during teriparatide treatment were similar in GC users and nonusers. This improvement was significant in both groups, despite the worse baseline HRQOL of the GC users. The benefits with regard to back pain and HRQOL were maintained after teriparatide was discontinued, when most of the patients received subsequent antiresorptive therapy, mainly oral bisphosphonates.
Our study has several limitations. First, the number of patients in the GC users group was rather small (294 patients, 18% of total study cohort). Second, the study was not randomized and there was no comparator group to teriparatide, so we cannot attribute observed changes in any endpoint to teriparatide treatment. Third, although the risk of fracture is related to GC dose and duration of therapy1, we did not collect quantitative data on these variables. Fourth, our method for quantifying the fracture incidence may have led to an underestimation of fractures, because only symptomatic vertebral fractures were considered, and it is well known that between 60% and 70% of spine fractures are asymptomatic. Fifth, as the information on previous and concurrent medication use was based on patient self-report, it may be subject to recall bias. In addition, the back pain results must be interpreted conservatively because we did not collect information on the use of analgesics during the study. Finally, the study included only postmenopausal women, so the findings cannot be extended to men or premenopausal women.
As the safety of teriparatide has already been established and was not an objective of this observational study, adverse events were not recorded. Investigators were reminded to report any significant adverse events to the study sponsor. All spontaneously reported adverse events have been reported previously10 and confirm that teriparatide is well tolerated.
The strengths of our study include the recruitment of a diverse range of patients, many of whom had comorbidities or were taking concomitant medications often excluded in RCT, reflecting real-life clinical practice. Other strengths are the prospective examination of clinical fractures both during teriparatide therapy and after teriparatide discontinuation, the analysis of pain and HRQOL using validated patient-completed instruments, and the adjustment for potential confounding factors in the analyses, including age, prior bisphosphonate use, and previous fracture in the 12 months before starting teriparatide.
In our study of postmenopausal women with severe osteoporosis treated with teriparatide for up to 18 months and followed for an additional 18 months in a routine setting, those who were also receiving GC, and who were therefore at even greater risk of fracture, showed a reduced incidence of clinical fractures during the third year, when most patients were receiving sequential therapy with other osteoporosis medications. These patients also reported a significant reduction in back pain and an improvement in HRQOL during the 18 months of teriparatide treatment, which was maintained for at least 18 months after teriparatide was discontinued, when the majority of patients were receiving other osteoporosis medication. Our findings should be interpreted in the context of a noncontrolled observational study and the small number of GC users analyzed.
Acknowledgment
The authors thank all physicians and patients participating in EFOS. The authors also thank Christine Jones, Lilly Germany, for central study coordination; Clare Barker for the development of the statistical analysis protocol and the study analysis; and Deirdre Elmhirst for helping in the preparation of the manuscript.
Footnotes
-
The EFOS study is funded by Eli Lilly and Company.
- Accepted for publication October 27, 2011.








{kind=link}
{kind=link}
{kind=link}