

Abstract
Objective. To describe morbidity, organ damage, mortality, and cause of death in patients with antiphospholipid syndrome (APS).
Methods. Descriptive analysis of 135 patients. Patients were clustered according to initial event: arterial thrombosis including stroke (AT; n = 46), venous thrombosis including pulmonary emboli (VT; n = 53), or pregnancy morbidity (PM; n = 36). Disease progression according to initial event and prevalence of organ damage was observed.
Results. APS occurs among young individuals (mean age 33.3 ± 11.9 yrs). One-third of the patients have APS secondary to systemic lupus erythematosus (SLE) or SLE-like disease. A broad spectrum of clinical manifestations mark the disease onset even before diagnosis. The pattern of initial presentation is preserved with regard to second event; VT is followed by VT (84%), AT is followed by AT (95%), and PM is followed by PM (88.9%). The highest morbidity is attributed to neurologic damage. PM is more likely to be followed by a second event, yet is associated with less organ damage than AT and VT. After a mean followup of 7.55 years, 29% of patients experienced organ damage and 5 died, with Systemic Lupus International Collaborating Clinics score associated with increased mortality (HR 1.31, 95% CI 1.07–1.60, p = 0.01, per 1-unit increase); hematological malignancies occurred in 2 patients after a cumulative followup of 1020 person-years. Coexistent SLE adds significant damage in patients with APS.
Conclusion. APS is a disease of young individuals, who experience increased morbidity. Neurologic damage is the most common cause of morbidity. AT at presentation as well as coexistent SLE are associated with poor outcome.
Antiphospholipid syndrome (APS) is an immune-mediated acquired thrombophilia characterized by recurrent venous and/or arterial thrombosis and/or pregnancy morbidity1,2. A requirement for the diagnosis is the presence of antiphospholipid antibodies (aPL) detected as anticardiolipin (aCL) antibodies, antibodies to ß2-glycoprotein I (anti-ß2-GPI) by ELISA or lupus anticoagulant (LAC) using coagulation assays, present on 2 occasions 12 weeks apart. APS may occur alone (primary, PAPS) or in association with other autoimmune diseases, mainly systemic lupus erythematosus (SLE) or lupus-like disease (secondary, SAPS)3. Clinical manifestations of APS are associated with the size and site of the occluded vessels. Clinical features of venous thrombosis are superficial and deep-vein thrombosis, cerebral venous thrombosis4, retinal vein thrombosis, pulmonary emboli, pulmonary arterial hypertension5, and Budd-Chiari syndrome6. Clinical features of arterial thrombosis are migraines, strokes, transient ischemic attacks7,8, myocardial infarctions9, Libman-Sacks endocarditis9, arterial thrombosis of upper and lower extremities, ischemic leg ulcers, digital gangrene, avascular necrosis of bone10, miscarriages due to ischemia of the placenta, retinal artery occlusion that leads to transient vision loss, renal artery stenosis and glomerular lesions2,11, and infarcts of spleen, pancreas, adrenals, and peritoneum12,13.
Progression in patients after longterm followup is not well studied. However, the disease is characterized by increased morbidity and mortality14,15,16; immune-suppression does not halt thrombotic recurrences17; arterial is usually followed by arterial and venous by venous thrombosis; and autoimmune hemolytic anemia connotes serious APS18. Additionally, endstage organ damage such as renal failure in the context of APS nephropathy11,19 or cognitive dysfunction4 associated with central nervous system (CNS) white-matter lesions characterizes a relatively high percentage of patients with APS.
We describe clinical characteristics and associations with initial manifestations of the disease, clinical features of organ damage, mortality, and cause of death in patients with APS after a longterm followup.
MATERIALS AND METHODS
Study cohort
This cohort comprised 135 consecutive patients, 89 patients with PAPS and 46 with SAPS3, who fulfilled the revised APS classification criteria2, with no prior selection according to disease severity, type of initial manifestation, or the referral pathway. We included both PAPS and SAPS in our study since the clinical profile of APS is similar in SAPS and PAPS14,20. Patients were followed on a regular basis every 2–6 months with additional unscheduled visits and hospitalizations when needed at the Department of Pathophysiology, University of Athens. Our department is the largest referral center for autoimmune diseases in Greece and nearly one-fourth of our patients are referred to us by smaller departments and private practitioners. Patients were treated with a target international normalized ratio between 2.5 and 3.521. Retrospective information on disease pattern and progression was collected from patients’ files and cross-validated with information from patients’ interviews. Patients were categorized in 3 groups according to their initial clinical manifestation — arterial thrombosis including stroke (AT; n = 46), venous thrombosis including pulmonary emboli (VT; n = 53), and pregnancy morbidity (PM; n = 36).
Our study was approved by the Ethics Committee of the National University of Athens.
Definitions
Arterial and venous thromboses were defined and documented according to a combination of compatible clinical features and imaging findings22. Pulmonary embolism was detected by imaging techniques in the context of the appropriate clinical setting. Stroke was defined as a rapid onset of focal CNS signs and symptoms. If the symptoms were sustained for only a few minutes the event was characterized as a transient ischemic attack. Documentation of stroke required brain magnetic resonance imaging (MRI). Myelopathy was defined as a rapidly progressive spinal cord syndrome with limb weakness, incontinence, and bilateral sensory loss accompanied by a sensory level, not related to cord compression. Spinal MRI and cerebrospinal fluid examination were performed to exclude other syndromes. Cognitive function was routinely assessed during the followup period through the Mini-Mental State examination23. Epilepsy, seizures, diplopia, transient vision loss, migraine, and chorea were defined on clinical grounds. Pregnancy morbidity was defined according to the recently revised APS classification criteria2. Pulmonary arterial hypertension (PAH) was defined as described24. Confirmation of acute respiratory distress syndrome required the following: acute onset, bilateral infiltrates on chest radiography, pulmonary artery wedge pressure ≤ 18 mm Hg or absence of clinical evidence of congestive left heart failure, and refractory hypoxemia with PaO2:FiO2 < 200. Pericarditis and Libman-Sacks endocarditis were diagnosed by heart ultrasonography, which was performed at least once in all patients. Budd-Chiari syndrome was documented by ultrasound and hemodynamic assessment of the portal vein blood flow, showing obstruction. Renal involvement classified as SLE nephritis25 or APS nephropathy2,11 was documented by renal biopsy. Thrombocytopenia and leukopenia were defined as platelet count < 100 × 109/l–1 and white blood cell count < 4 × 103/l–1, respectively, confirmed at least twice, 12 weeks apart. Autoimmune hemolytic anemia and chronic disease anemia were also recorded. Anticardiolipin antibodies (considered positive when absorbance values were > 40 IgG or IgM phospholipid units or the 99th percentile of normals) and anti-ß2-glycoprotein I (GPI) antibodies (considered positive when absorbance values were > 99th percentile of normals) were measured by a standardized ELISA2. Antinuclear antibodies were detected by immunofluorescence, using Hep2 cells as substrate and anti-dsDNA antibodies by ELISA26,27; C3 and C4 complement levels measured by nephelometry and LAC were recorded28,29. Patients with inherited thrombophilias as the sole explanation for thrombosis were excluded.
Documentation of organ damage included severe cognitive dysfunction and dementia, neurologic damage (severe paralysis prohibiting performance of usual tasks, myelopathy), renal failure, severe heart failure, severe PAH, amputation due to vascular events, myocardial ischemia, APS nephropathy, and catastrophic APS (CAPS)30,31,32. The Systemic Lupus International Collaborating Clinics (SLICC) damage index was used to assess accumulated organ damage33. Deaths and cause of death were recorded.
Statistical analysis
Categorical variables were compared by chi-square test. Continuous variables were reported as mean (SD) or median (IQR) and compared using the t test statistics. Cumulative damage (reported as SLICC damage index) was treated as a continuous variable, and the effect of confounders (age, sex, SLE, CAPS, arthritis, type of initial event) was adjusted for time of followup, using a multivariable regression technique, with step-by-step backward elimination of insignificant covariates. Incidence rates were reported for outcomes of interest, and the Kaplan-Meier method with log-rank p was used to assess probabilities of second vascular event. All statistics were 2-tailed and were considered statistically significant if p < 0.05. Stata v8 (Stata Corp., College Station, TX, USA) was used for data analysis.
RESULTS
APS is a disease of young individuals
Between January 2008 and September 2010, 135 patients (100 female, 35 male) fulfilling the revised APS criteria2 were enrolled for study. The mean age at entry was 33.3 (SD 11.9) years for the entire cohort, with no significant difference between men (33.9 yrs, SD 11.0) and women (33.4 yrs, SD 11.6; p = 0.83). The mean disease duration was 8.8 years (SD 5.3) and the mean duration of followup 7.55 (SD 4.89) years.
A wide spectrum of clinical findings mark onset of APS prior to diagnosis
Nearly one-fifth of patients experienced venous thrombosis and one-fourth of the women experienced fetal loss as presenting manifestations. Peripheral arterial events, strokes, and pulmonary emboli occurred in 4.5%, 7.4%, and 5.2% of patients, respectively. Epilepsy (1.5%) and headache/migraine (4.5%) of recent onset were recorded. Ischemic leg ulcers and digital gangrene were rare (Table 1).
Prevalence of clinical and laboratory characteristics at the onset of disease and during followup.
A wide range of clinical features associated with SLE or lupus-like disease, such as arthralgia, frank nonerosive arthritis, butterfly rash, maculopapular rash, and photosensitivity, characterized the disease onset. Despite anticoagulation, patients tended to experience thrombotic recurrences throughout the followup period, as described below. The same was true for clinical features unrelated to APS; thus their cumulative prevalence increased over time (Table 1).
The baseline profile of PAPS (n = 89) compared to SAPS (n = 46) patients showed insignificant differences: mean age at disease onset was 34.3 (SD 12.2) years for PAPS compared to 31.9 (SD 11.3) years for SAPS (p = 0.28). Female predominance was also similar between PAPS and SAPS (71.9% and 78.3%, respectively; p = 0.43). The initial vascular events also showed insignificant variation in PAPS (42.7% VT, 31.5% AT, 25.8% PM) compared to SAPS (32.6% VT, 39.1% AT, 28.3% PM; p = 0.50). Also with regard to PAPS versus SAPS, no significant differences were noted in anticardiolipin profile, including aCL-IgG (66.3% vs 78.3%, respectively; p = 0.15), aCL-IgM (68.5% vs 71.7%; p = 0.70), anti-ß2-GPI-IgG (36.0% vs 39.1%; p = 0.72), and anti-ß2-GPI-IgM (7.9% vs 15.2%; p = 0.18).
Association of initial events with clinical and serological features of APS
The presenting events were, in descending order, VT 53 (39.3%), AT 46 (34.0%), the majority of which was stroke (31/46), and PM 36 (26.7%). After stratification for type of the initial event, the 3 groups were similar with regard to demographics and clinical and immunologic profiles, with one notable exception, i.e., the significant association of PM with younger age, lower frequency of livedo reticularis, and lower frequency of detected anti-ß2-GPI-IgG compared to the VT and AT groups (Table 2).
Profile for the entire cohort stratified for type of initial manifestation.
Patients with initial VT, AT, or PM tended to develop a second undesired event, within a time interval ranging from 1 to 326 months (median 60 mo). The frequency of type of event was VT (22/72, 30.6%), AT (26/72, 36.1%), and PM (24/72, 33.3%). APS patients with an obstetric event at presentation were more likely to have a second undesired event (Figure 1). The median time elapsed from first event was 161 months for VT, 125 months for AT, and 24 months for PM (log-rank p = 0.001).

Time to a second undesired event if the initial event was venous thrombosis (VT), arterial thrombosis including stroke (AT), or pregnancy morbidity (Pregnancy). Time from the initial to a second undesired event was significantly different among the 3 groups.
After a cumulative followup of 887.5 person-years, a second undesired event occurred in 72 cases (6.76/1000 person-yrs, 95% CI 5.36–8.51). The pattern of initial presentation was preserved with regard to the second event, i.e., in cases of APS with VT at presentation the second event was also VT (84%), AT recurred with AT (95%), and pregnancy events recurred with pregnancy events (88.9%).
Arterial thrombotic events in patients with APS were not related to traditional risk factors for atherosclerosis
Patients with AT events were compared with the remaining patients with APS in terms of traditional risk factors for atherosclerosis; no statistically significant difference was found (Table 3).
Comparison of traditional risk factors between patients with arterial thrombosis (AT) at presentation and those with venous thrombosis (VT) or pregnancy morbidity (PM).
Organ damage occurred in 29% and death in 3.7% of patients with APS, in a mean period of 7.55 years
After a cumulative followup of 1020 person-years (median 7, IQR 4–10), organ damage was found to occur in 39 patients (28.9%). Altogether we recorded 1 case of heart failure, 5 cases of renal failure, 8 PAH, 24 neurologic damage, 9 cognitive dysfunction and dementia, 3 amputation, 1 myocardial ischemia, 6 APS nephropathy, and 4 cases of CAPS. At the end of followup, the damage rates stratified for the initial event were 30.2% (16/53) for VT, 34.8% (16/46) for AT, and 19.4% (7/36) for PM.
The highest morbidity was attributed to neurologic damage, with an estimated rate of 18.71 events/1000 person-years. After stratification for the initial event, no significant differences were found between groups with regard to organ damage. A notable exception was the significantly increased rate of neurologic damage in the AT group compared to the VT group (35.4/1000 vs 8.97/1000 person-yrs, respectively). Morbidity in the PM group was limited to APS nephropathy and neurologic damage (Table 4).
Qualitative characteristics of organ damage presented as rate (per 1000 person-years). Neurologic damage is the cause of highest morbidity. Patients with pregnancy morbidity (PM) rarely have organ damage compared to patients with arterial thrombosis (AT) or venous thrombosis (VT).
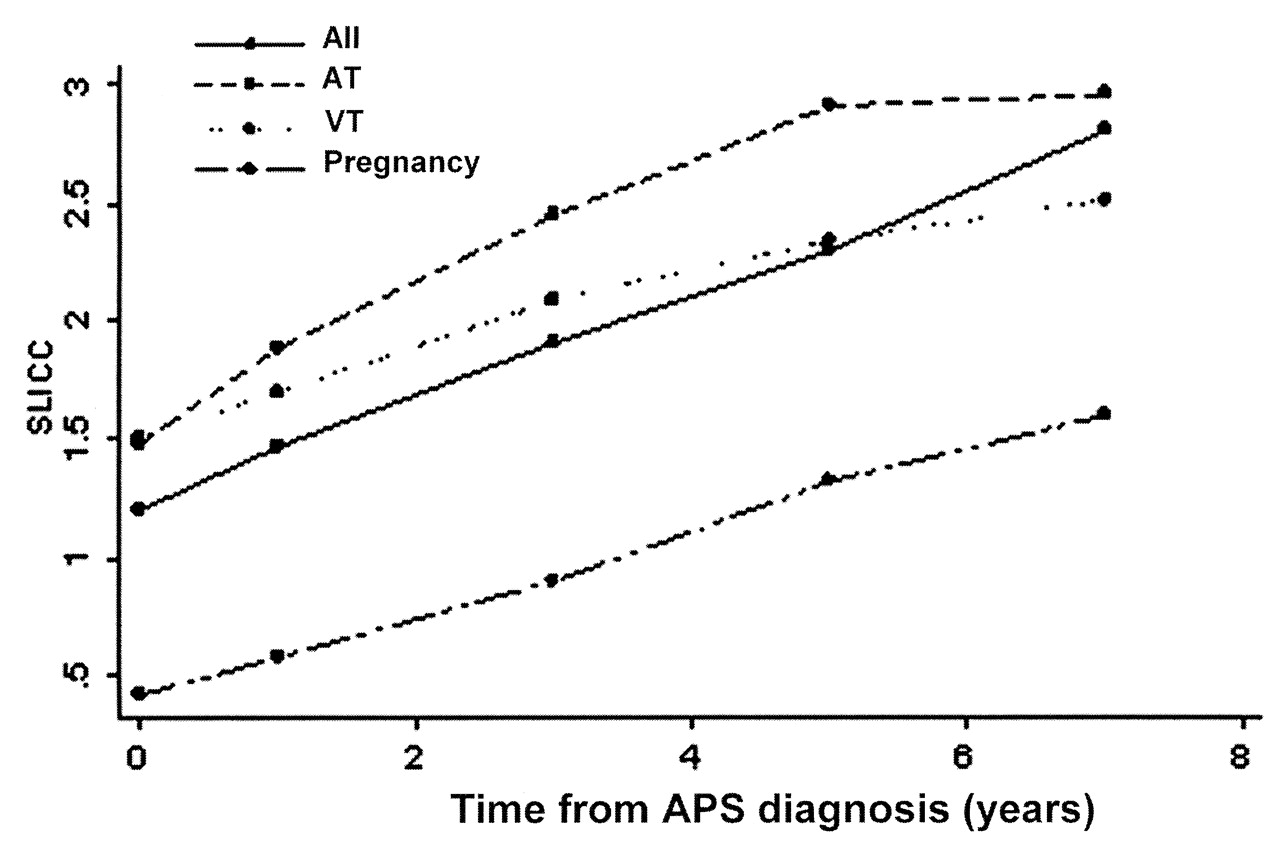
The SLICC damage index was utilized to assess accumulated damage that had occurred since the onset of APS. Median SLICC score at the end of followup was 2 (IQR 1–3). After stratification for the initial event, the PM group had the lowest score, whereas the AT group had the highest (PM < VT < AT; all comparisons significant). The mean SLICC score during followup is plotted in Figure 2, stratified for the initial event. It is shown that the SLICC index increased over time and that the PM group did consistently better over time compared to the VT and AT groups (all comparisons significant, p < 0.05, at timepoints 0, 1, 2, 3, 5, and 7 yrs).

Mean Systemic Lupus International Collaborating Clinics (SLICC) scores of patients at onset of antiphospholipid syndrome (APS; year 0) and measured at years 1, 3, 5, and 7. Pregnancy morbidity as an initial manifestation was associated with less organ damage than in the other groups of patients with APS. AT: arterial thrombosis group; VT: venous thrombosis group.
In multiadjusted regression analysis for the entire followup period, the type of initial event, CAPS, and coexistent SLE were significant moderators of damage. Pregnancy morbidity (ß coefficient = –1.01, p = 0.04) was found to be associated with less damage compared to VT and AT at presentation. CAPS (ß coefficient = 3.42, p = 0.01) and coexistent SLE (ß coefficient = 1.11, p = 0.01) add significant damage, after adjustment for confounders.
After a cumulative followup of 1020 person-years, 5 patients had died, 3 due to CAPS34, 1 by pulmonary emboli, and 1 by acute pulmonary edema. Only 1 out of 5 patients who died showed poor compliance to therapy. The remaining patients died due to disease activity and/or comorbidities. Four out of 5 patients who died had had organ damage during followup. SLICC score as a surrogate damage marker was associated with increased mortality (HR 1.31, 95% CI 1.07–1.60, p = 0.01, per 1-unit increase).
DISCUSSION
This was a retrospective analysis of the largest APS patient cohort from Greece focusing on morbidity, mortality, and organ damage after a longterm followup. A wide range of clinical findings characterized the disease onset: the most common were fetal loss, venous thrombosis, and arthralgia, followed by strokes, frank arthritis, butterfly rash, photosensitivity, peripheral arterial thrombotic events, and headaches and migraines. Similar patterns of disease presentation have been observed by others14,35,36. As the disease progresses the prevalence of initial clinical features increases, despite treatment. The prevalence of epilepsy/seizures increased from 1.5% to 14% during the followup; Cervera, et al described a total frequency of 7%14, and Shoenfeld, et al a total frequency of 8.6%37. Patients with pregnancy morbidity at presentation were more likely to experience a second event. The pattern of initial presentation was preserved. Thus, venous thrombosis was followed by venous thrombosis, arterial thrombosis by arterial thrombosis, as previously shown35,36,38, and pregnancy morbidity by pregnancy morbidity. Patients with an initial peripheral arterial thrombosis did not seem to constitute a distinctive subgroup, although it is notable that pregnancy morbidity was completely absent from this subgroup. The presence of autoimmune hemolytic anemia was associated with unfavorable outcomes, as shown previously36,39. Our study indicates that SLE and CAPS are significant moderators of damage and poor outcome in patients with APS. Indeed, SLE is a marker for poor outcome in patients with CAPS40, while APS-related thrombotic manifestations are a major predictor of irreversible organ damage and death in patients with SLE41.
Increased prevalence of atherosclerosis has been reported in APS42. However, arterial thrombosis was not related to traditional risk factors for atherosclerosis in our study. Endothelial perturbation in the absence of other detectable traditional risk factors for atherosclerosis43 could explain the arterial thrombosis. Prevalence of plaque in patients with PAPS was similar to that of controls and less than that of patients with SAPS44, while plaques in APS and SLE were not associated with other predictors of atherosclerosis such as lipid indicators and cumulative steroid dose42. Hypertriglyceridemia, low high-density lipoprotein levels, and obesity are also the main components of metabolic syndrome, which was found to have a high prevalence among patients with PAPS, and increase the risk of cardiovascular disease45. In general, atherosclerosis may occur in patients with APS but not as commonly as previously thought46. Therefore, traditional risk factors for atherosclerosis are less involved in arterial disease, while anti-aPL antibodies appear to be the major agents47.
A high rate of morbidity and mortality was observed among patients with APS. The highest morbidity was attributed to neurologic damage, which was more common among patients with initial arterial thrombosis. Patients with pregnancy morbidity do consistently better over time compared to patients with venous or arterial thrombosis, as shown by the calculation of the SLICC damage index. To our knowledge this is the first attempt to assess and quantify organ damage in APS in order to illustrate the social and financial effects of the disease. Although it is validated only for SLE, the SLICC index includes damage caused by APS in its calculation. In the absence of a specific damage index for APS, the SLICC can be used to crudely measure damage in APS. Patients with SAPS are expected to have greater overall accrual of damage due to their underlying condition, as shown by our analysis. Deaths were observed in 5 patients (3.7%) after a cumulative followup of 1020 patient-years — despite intensive anticoagulation in 4 of them. This frequency is lower than, yet comparable to that described by Finazzi, et al (5%)48 and by Cervera, et al (5.3%)49. However, the causes of mortality were different. In our cohort, 3 cases with CAPS, 1 with pulmonary emboli, and 1 with acute pulmonary edema were documented. Bacterial infections, myocardial infarction, and stroke were the most frequent causes of death reported in the multicenter European study by Cervera, et al15, while vascular events and hematological malignancies were the most common causes of death reported by Finazzi, et al48. This inconsistency of the causes of mortality can be attributed to the small number of patients, which makes it difficult to draw definite conclusions. Hematological malignancies were observed in 2 (1.48%) patients over the entire followup period, 1 orbital mucosa-associated lymphoid tissue lymphoma and 1 splenic lymphoma, comparable to the 1 observed previously48. Both studies, however, underline a high incidence of hematological malignancies, mainly non-Hodgkin’s lymphomas, compared to the general population (3–14 cases per 100,000 person-yrs)49.
Our analysis showed no significant difference of the clinical and serological profiles of APS between cases of PAPS and SAPS at baseline. Vianna, et al20 reported that patients with PAPS and SAPS share a similar clinical picture of APS, apart from cardiac valve disease, which was more common in SAPS. In addition, antinuclear antibodies, low C4 complement component levels, and autoimmune hemolytic anemia occurred, as expected, at a higher incidence in SAPS, since they are SLE-related20. The large multicenter European study from Cervera, et al14 showed no significant difference in clinical features of APS between patients with PAPS and SAPS. It was shown that patients with SAPS more often experience arthritis, livedo reticularis, leukopenia, and thrombocytopenia, but these are also SLE-related14.
Our study has limitations because of its retrospective design. The recall bias and the limited generalizability of the findings due to the relatively small cohort in contrast to multicenter studies are acknowledged. However, in contrast to multicenter studies, most of which are also retrospective, we were able to evaluate the patients using standard methodology and protocols.
Our study indicates that APS occurs among young individuals and it is a cause of increased morbidity, with one-fourth of the patients progressing to organ damage in a mean time of 10 years from disease onset. The highest morbidity was attributed to neurologic damage, which was more common among patients with an arterial thrombosis as an initial manifestation. The type of initial presentation is preserved with regard to a second event and therefore arterial are followed by arterial and venous by venous thrombotic events, while pregnancy morbidity recurs with pregnancy morbidity. Pregnancy morbidity is more likely to be followed by a second event, yet is associated with less organ damage than arterial and venous thrombotic events. The SLICC damage index score increases over time and is associated with increased mortality. Coexistent SLE adds significant damage in patients with APS.
- Accepted for publication October 14, 2011.








{kind=link}
{kind=link}