

Abstract
Objective. Optimizing therapeutic strategies to induce remission requires an understanding of the initial features predicting remission. Currently no suitable model exists. We aim to develop a remission score using predictors of remission in early rheumatoid arthritis (RA).
Methods. We used a dataset from a UK randomized controlled trial that evaluated intensive treatment with conventional combination therapy, to develop a predictive model for 24-month remission. We studied 378 patients in the trial who received 24 months’ treatment. Our model was validated using data from a UK observational cohort (Early RA Network, ERAN). A group of 194 patients was followed for 24 months. Remission was defined as 28-joint Disease Activity Score < 2.6. Logistic regression models were used to estimate the associations between remission and potential baseline predictors.
Results. Multivariate logistic regression analyses showed age, sex, and tender joint count (TJC) were independently associated with 24-month remission. The multivariate remission score developed using the trial data correctly classified 80% of patients. These findings were replicated using ERAN. The remission score has high specificity (98%) but low sensitivity (13%). Combining data from the trial and ERAN, we also developed a simplified remission score that showed that younger men with a TJC of 5 or lower were most likely to achieve 24-month remission. Remission was least likely in older women with high TJC. Rheumatoid factor, rheumatoid nodules, and radiographic damage did not predict remission.
Conclusion. Remission can be predicted using a score based on age, sex, and TJC. The score is relevant in clinical trial and routine practice settings.
Rheumatoid arthritis (RA) is a heterogeneous disease with variable longterm outcomes that are difficult to predict. Its course ranges from drug-free remission to severe joint damage and extraarticular manifestations1. Better treatment has reduced the severity of RA2,3 and, in particular, early intensive treatment has improved both clinical and radiological outcomes4. As a consequence, remission has become the main treatment aim in early RA. Contemporary therapies such as intensive treatment with disease-modifying antirheumatic drugs (DMARD) and combined use of DMARD with biologics have made remission a realistic target5. Optimizing therapeutic strategies to induce remission requires an understanding of the initial features predicting remission; currently no suitable model exists.
We have developed a predictive model for 24-month remission in patients with early RA treated in a randomized controlled trial (RCT) using methotrexate (MTX), steroids, and combination DMARD6. We validated this predictive model using data from a UK cohort — the Early RA Network (ERAN)7. These datasets provide a unique comparative assessment of remission in clinical trial and routine practice settings in patients seen across a large number of UK specialist centers.
MATERIALS AND METHODS
Clinical trial patients
The Combination of Anti-Rheumatic Drugs in Early RA (CARDERA) trial recruited patients with RA of < 2 years’ duration who had evidence of clinically active disease. The trial involved 42 specialist rheumatology centers in England and Wales. Details have been published previously6. A total of 467 patients were recruited, and 378 patients remained on trial treatment and had full datasets at 24 months; analyses of remission were restricted to this group. Patients were assessed initially and then every 6 months for 24 months. The trial compared 4 treatment regimens, which were allocated randomly to equal numbers of patients. These regimens comprised MTX monotherapy; MTX and cyclosporine; MTX and prednisolone; and MTX, cyclosporine, and prednisolone.
Observational cohort patients
ERAN is an inception cohort of patients with newly diagnosed RA who were recruited from 19 centers across the United Kingdom. It reflects contemporary routine care of patients with early RA7. We analyzed data collected from 2002 to 2007. The 194 patients who completed 24 months’ followup at the time of analysis were evaluated. Patients were assessed at first presentation, at 3–6 months, and at 12 and 24 months. Treatment was determined by the supervising clinician. Initial DMARD monotherapy, given to 94% of patients, comprised MTX (47%), sulfasalazine (42%), hydroxychloroquine (7%), leflunomide (2%), gold injections (1%), and cyclosporine (0.5%). Four percent of patients received 2 DMARD initially and 2% started initial triple DMARD therapy. Oral or intramuscular steroids were used in 70% of patients.
Clinical variables
Remission was defined as a 28-joint Disease Activity Score (DAS28) of < 2.68. The following initial variables were present in both the clinical trial and the observational study: age, sex, rheumatoid factor (RF) positivity, rheumatoid nodules, Health Assessment Questionnaire (HAQ) scores, tender joint count for 28 joints (TJC28), swollen joint count for 28 joints (SJC28), erythrocyte sedimentation rate (ESR), and patient global assessments (PGA). Initial Larsen scores and Medical Outcomes Study Short-Form 36 scores were also available in the clinical trial.
Statistical analysis
Data were analyzed using Stata version 10 (StataCorp, College Station, TX, USA). Individual variables were assessed descriptively as median values and interquartile ranges (IQR). Univariate and multivariable logistic regression models were used to estimate the associations between baseline variables that are potential predictors of remission at 24 months. In this analysis, variances were adjusted for intersite effect using Huber-White sandwich (robust) estimator. Analyses were restricted to those individuals with complete data at 24 months. All continuous measures were entered into the models in this format. The results were presented as univariate and multivariate OR with 95% CI and p were 2-tailed throughout. Those variables that had p values ≤ 0.05 in the univariate analysis were carried forward into multivariate analysis. We also assessed whether variables were colinear for the final model; we considered variables were correlated if their correlation coefficient was > 0.5. The regression coefficient (β) of the variables from the final model was used to estimate the score. The predictive model was calculated to be
We also derived a simplified remission score, based on the factors identified in the regression analysis.
The area under the curve from the receiver-operating characteristic (ROC) was used to assess the model’s ability to discriminate between patients in remission and those not in remission.
RESULTS
Patients and remission rates
The clinical trial randomized 467 patients. There were 259 women (68%); their median age was 54 years (IQR 46, 64 yrs); 259 (68%) of them were RF-positive, and 82 (22%) had rheumatoid nodules (Table 1). There were full datasets at 24 months for 379 (81%) of the patients, and analyses were restricted to this group. Seventy-four (20%) were in remission at 6 months, 15% were in remission at 12 months, and 21% at 24 months. The proportion of patients who did not achieve remission at any point during the study was 65%. Fourteen percent achieved remission at 1 timepoint, 8% at 2 timepoints, and 7% had sustained remission over all timepoints.
Patient characteristics of the Combination of Anti-Rheumatic Drugs in Early RA (CARDERA) clinical trial and the Early RA Network (ERAN) observational cohort.
The observational cohort had enrolled 194 patients who had completed 24 months’ followup. The cohort included 140 women (72%); their median age was 56 years (IQR 47, 66 yrs); 72% were RF-positive, and 28% had nodules (Table 1). Twenty-four percent achieved remission at 6 months, 20% at 12 months, and 30% of patients achieved remission at 24 months. Twenty-three percent achieved remission at one timepoint, 12% at 2 timepoints, and 4% had sustained remission over all timepoints. The baseline characteristics of these 2 cohorts were similar with the exception of the baseline disease activity, which was expectedly higher in the RCT (Table 1).
Multivariate remission score: regression analysis of clinical trial data
Univariate analysis showed significant associations (p < 0.05) between remission at 24 months and age, sex, baseline HAQ, TJC28, SJC28, and patient global scores. Multivariate logistic regression analyses showed that only age, sex, and TJC28 remained independently associated with remission at 24 months. RF, nodules, and baseline Larsen score did not affect remission (Table 2). The final model was assessed for correlations between variables to exclude colinearity; the correlation coefficient was < 0.5.
Baseline variables predictive of remission at 24 months in the Combination of Anti-Rheumatic Drugs in Early RA (CARDERA) clinical trial using univariate and multivariate logistic regression.
Developing multivariate remission score using clinical trial data
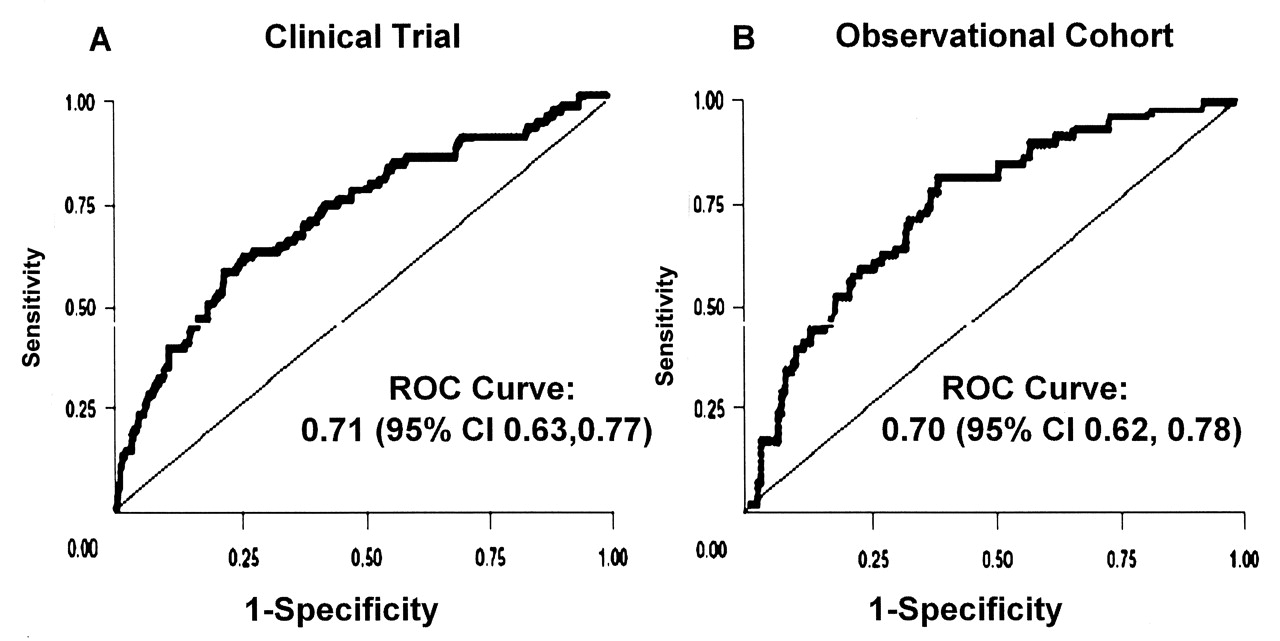
A multivariate remission score was generated using the coefficients from multivariable logistic regression analysis (Table 2). The remission score was 0.37 + (–0.03 × age) + (1.1 × sex†) + (–0.07 × baseline TJC28) [† sex: 1 for males, 0 for females). A higher value indicates a higher probability that the patient will achieve remission at 24 months. Remission scores were calculated for each patient with a full dataset in the clinical trial. The area under the ROC curve was 0.71 (95% CI 0.63, 0.77; Figure 1A). When the cutpoint for the probability of identifying those patients in remission was set at 50% or more, the positive predictive value of the model was 69% and the negative predictive value was 81%.
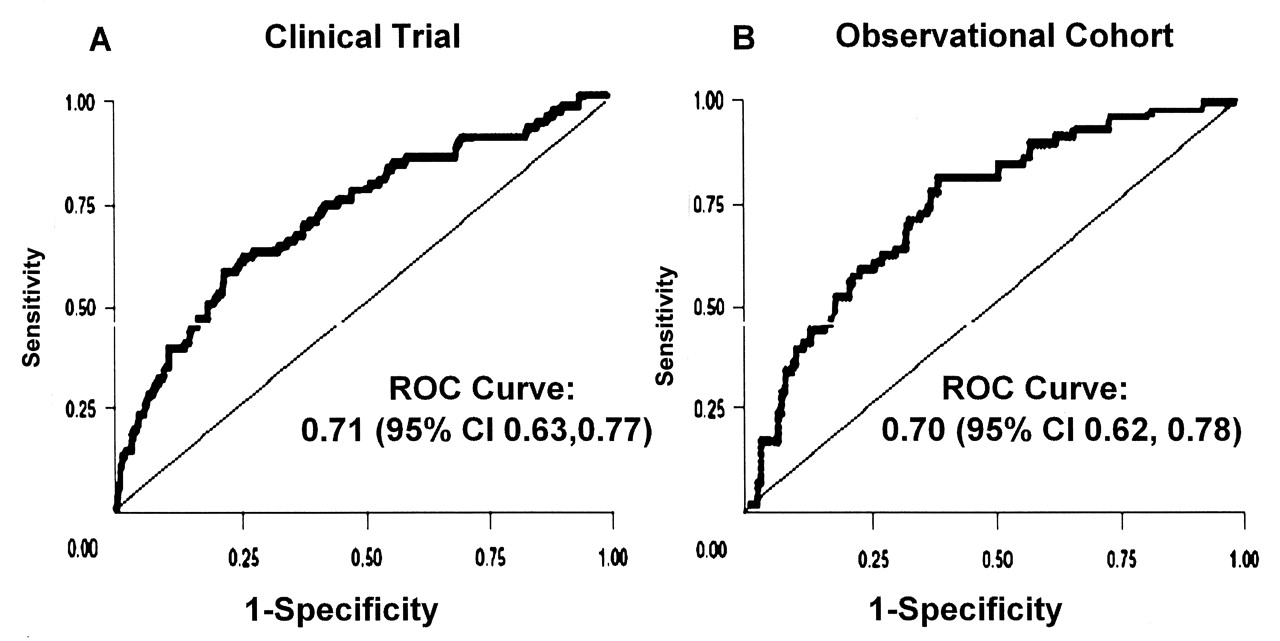
ROC curve for the remission score using the Combination of Anti-Rheumatic Drugs in Early RA (CARDERA) clinical trial (A) and the Early RA Network (ERAN) observational cohort (B).
Replicating multivariate remission score using observational data
Applying the multivariate remission score to patients in the observational study gave an area under the ROC curve of 0.70 (95% CI 0.62, 0.78; Figure 1B). The model correctly classified 71% of patients with a poor sensitivity of 29% but good specificity of 90%. The positive predictive value was 53% and negative predictive value was 74%.
Predictive model using multivariate remission score
The multivariate remission score was applied to predict the likelihood that patients would achieve remission at 24 months in both CARDERA and ERAN (Figure 2). Using the multivariate remission score, the more negative the scoring, the higher the likelihood that the patient would not achieve remission at 24 months. Overall, this approach correctly classified 80% of patients, but had a poor sensitivity (13%) despite good specificity (98%). Patients with low remission scores were unlikely to achieve remission at 24 months.

Predictive ability of multivariate remission scores in the Combination of Anti-Rheumatic Drugs in Early RA (CARDERA) clinical trial and the Early RA Network (ERAN) observational cohort.
Simplified remission score
Because clinicians may prefer not to use mathematical formulas when assessing patients, we also examined the components of the multivariate remission score with the intention of devising a simplified clinical tool for routine practice.
First, we divided patients by sex and then by age (under 50 and 50 years or older) and by baseline TJC (5 or less, 6–19, and 20 or more). The likelihood of achieving remission after 24 months was compared in the combined data from the CARDERA and ERAN datasets. The results of this comparison are shown in Figure 3. Men aged under 50 years who had a TJC 5 or lower when initially seen had high chances of remission at 24 months (71% of patients). In contrast, women aged over 50 years who had a TJC above 15 when first seen had a low chance of remission (11% of patients).

The relationship of 28-joint tender joint count, age, and remission according to sex in all patients.
Second, we created a simplified remission score by scoring 1 point for being male, 1 point for age < 50 years, 2 points for having TJC 5 or lower, and 1 point for TJC 6–15. This simplified remission score showed a high correlation with the multivariate remission score (Spearman’s correlation coefficient 0.80). For the purposes of comparison, we evaluated the likelihood of achieving DAS28 remission, low disease activity (DAS28 < 3.2), and high disease activity (DAS28 ≥ 5.1). The results are shown in Figure 4. High simplified remission scores (3 and 4), which were seen in 22% of patients, gave high chances of remission (37%–72%). They also gave high chances of low disease activity (47%–78%) and low chances of persistent high disease activity (12% or less). In contrast, low simplified remission scores (0 and 1), which were seen in 41% of patients, gave low chances of remission (7%–14%) and low chances of low disease activity (10%–20%), and high chances of persistent high disease activity (34%–67%).
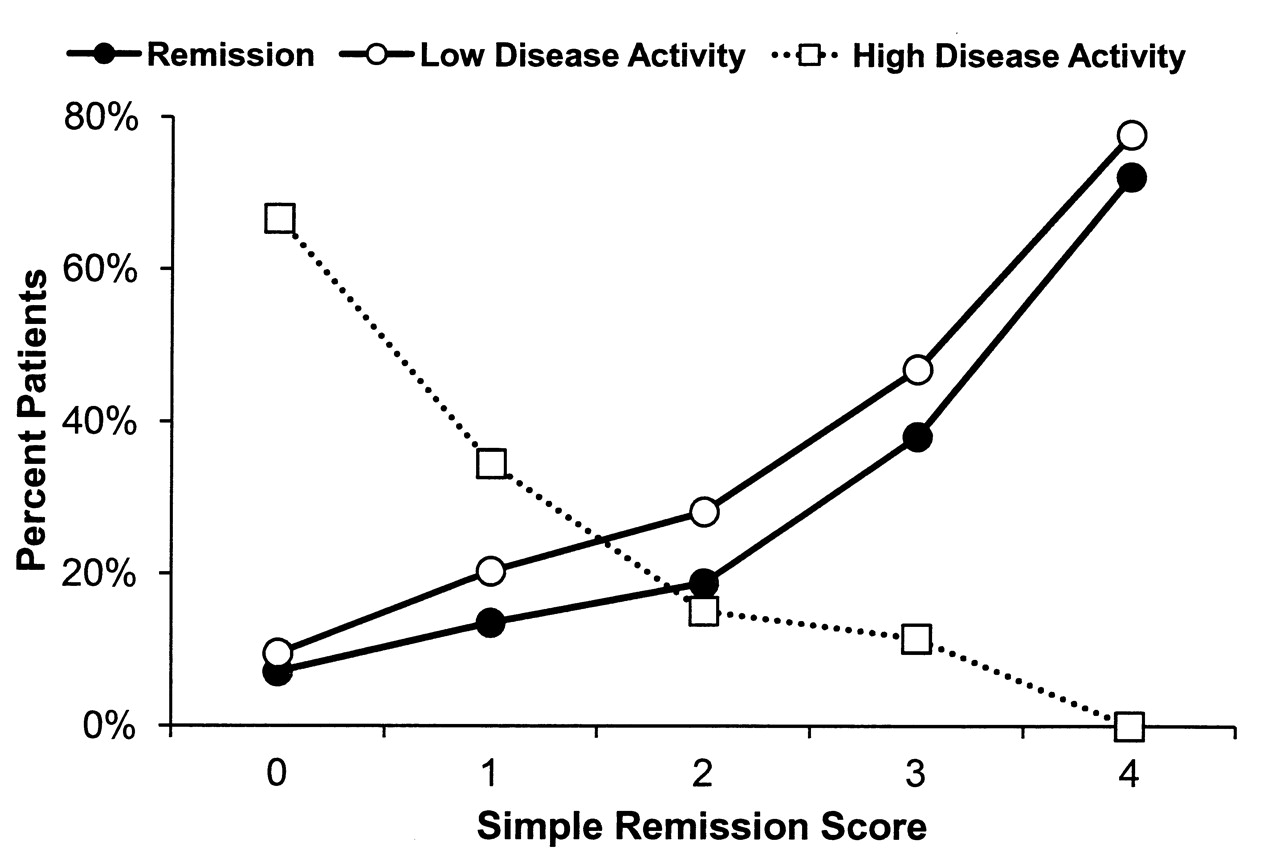
The ability of the simplified remission scores in predicting different disease states at 24 months in all patients.
DISCUSSION
We have developed a remission score using simple clinical assessments that correctly classifies over 70% of patients. The score is equally applicable in a clinical trial and routine practice setting. Three variables — sex, age, and initial TJC — are all that is required. There was a marked difference in the likelihood of remission between different groups. Men who are under 50 years of age with TJC 5 or lower were the most likely to be in remission at 24 months. RF, rheumatoid nodules, and radiographic damage did not contribute to the likelihood of remission. The simplified remission score is readily applied in routine practice, and is similar in approach to the Simplified Disease Activity Index9. The score is intended to identify those patients who are most likely to achieve remission as opposed to classifying the likelihood of predicting remission in all patients.
Assessing remission is complex, and observational studies and clinical trials report wide variations in remission rates5. Much of this variability reflects different definitions of remission. We used DAS28 remission occurring at a single timepoint. The conventional American College of Rheumatology (ACR) remission criteria10, which require sustained remission over 2 consecutive months, give substantially lower remission rates. The new ACR/European League Against Rheumatism criteria also give lower remission rates11. Sustained remission from 6 months onward was rare in both our patient groups. However, because sustained remission is associated with reduced radiological progression12, it should be the ultimate therapeutic aim. Data from the Quest RA study13, which provides international comparisons, also show that sustained DAS28 remission is uncommon.
Not all patients with RA require identical treatment. Instead, therapy should be individualized on the basis of risk factors. The prediction of possible remission is one practical way of risk stratification when patients are first seen. We used prediction methods similar to those used to predict the progression of RA from undifferentiated inflammatory arthritis14 and the likelihood of radiographic progression in RA15. Our remission score was equally applicable in patients treated in a clinical trial and in routine practice, suggesting it is likely to be generalizable.
Our study has several limitations. First, it used data collected for other purposes, and neither the clinical trial nor the observational study was powered to investigate remission. A far larger dataset is needed to investigate all the potentially relevant factors. Second, we did not examine in detail the effects of treatment and did not adjust our model to take this into account. This was primarily because too few patients received prolonged intensive treatments. We appreciate that larger numbers of patients need to be examined to fully evaluate treatment effects and we are certain that more intensive treatment regimens will increase the likelihood of developing remission. Although the CARDERA study used cyclosporine, which is not a commonly used DMARD in routine clinical practice, it involved combination DMARD and steroids, which are approaches recommended by many leading bodies such as the UK National Institute for Health and Clinical Excellence16. Third, using a single timepoint of 2 years as the sole criterion for judging remission is insufficiently rigorous, and extended periods of remission would be a more clinically relevant target. However, a far larger database would be required. Finally, although the specificity of our remission score is high, its sensitivity is relatively poor. The use of a more extended range of clinical and laboratory markers might improve the prediction of remission in future, and more research is needed in this area. Comorbidities and ethnicity might also be important contributors, although a large patient population would be required to evaluate these in detail.
Sex, initial DAS28 scores, and age have all been reported as important determinants of remission17,18,19,20,21,22. Interestingly, we found that the dominant clinical predictor of remission was TJC rather than SJC or ESR. The reason for this is uncertain. It might reflect greater levels of agreement between observers when assessing TJC compared with SJC23. Other possible explanations include the greater weighting of TJC within the DAS28 score and the interrelationship between TJC and fibromyalgic RA24,25. Of equal importance, evidence of disturbed immunity, such as seropositivity for RF, was unrelated to the development of remission. Although we chose to use the individual components of the DAS28 rather than the DAS28 score itself to predict remission, using DAS28 instead of the TJC in the multivariate prediction model gave a similar area under the ROC curve.
The purpose of determining patients’ subsequent chances of remission when they are first seen is to enable treatment to be stratified so that those patients with the least chance of remission can be treated most intensively. Women with high initial TJC have less chance of remission and therefore merit more intensive treatment. The effect of sex is so marked that treatments might need to be adjusted for it, and possibly clinical trials should analyze men and women separately. Different risk stratifications by sex are recognized in a range of medical disorders, particularly in cardiovascular diseases26. The effect of age is more complex. Although the risk of remission was reduced in the elderly, it might be counterproductive treating elderly patients more intensively because they are likely to have more comorbidities and are potentially at risk of more adverse events27.
Remission in early RA can be predicted using 3 initial independent predictors: sex, age, and TJC. We created a multivariate remission score as well as a simplified remission score using these 3 predictors. These can be combined in a remission score that is best at predicting those patients who are unlikely to achieve remission at 24 months. This was validated in an independent observational cohort, to improve the robustness of our study. It is likely that a broader range of potential predictors needs to be examined, particularly extended imaging and laboratory biomarkers, before such predictive assessment is adopted in routine practice. However, it is unlikely that RF status, erosion scores, or extraarticular features (e.g., nodules) will provide more useful data. We accept that it is premature to base current treatment on our remission score; further work is required to optimize this approach. However, the concept of a predictive remission score would be useful to tailor treatment regimes at an individual patient level.
Footnotes
-
Supported by Arthritis Research UK and the National Institute for Health Research (NIHR). Dr. Ma is an NIHR Fellow and Dr. Scott an NIHR Senior Investigator. ERAN has received funding from Wyeth Pharmaceuticals and the Healthcare Commission.
- Accepted for publication November 8, 2011.








{kind=link}
{kind=link}
{kind=link}
{kind=link}