

Sternocostoclavicular hyperostosis (SCCH), a rare, benign disorder, is frequently associated with skin lesions, but can occur without them. Patients showing only bone lesions initially may later develop cutaneous symptoms.
A 24-year-old white woman was referred for investigation of chronic pain and tenderness of the sternocostoclavicular region with minimal soft tissue swelling. The pain started 1 year before without history of trauma, low back pain, or arthritis. Examination did not reveal acne, palmoplantar pustulosis, or psoriasis. A range of laboratory examinations were normal: full blood count, erythrocyte sedimentation rate, C-reactive protein, rheumatoid factor, antinuclear antibody, serum alkaline phosphatase, and urinary hydroxyproline/creatinine ratio. HLA-B27 antigen was absent.
Computed tomography revealed dense osteosclerosis of the lower third of the sternal manubrium with bilateral ossification of the costoclavicular ligaments (Figure 1A) and erosions of the manubriosternal joint (Figure 1B). Partial ossification of the first right costochondral junction was present (Figure 1C). Magnetic resonance imaging (MRI) fast spin-echo T2-weighted coronal sequence with fat saturation showed bone marrow edema involving the lower third of the sternal manubrium (Figure 2A).
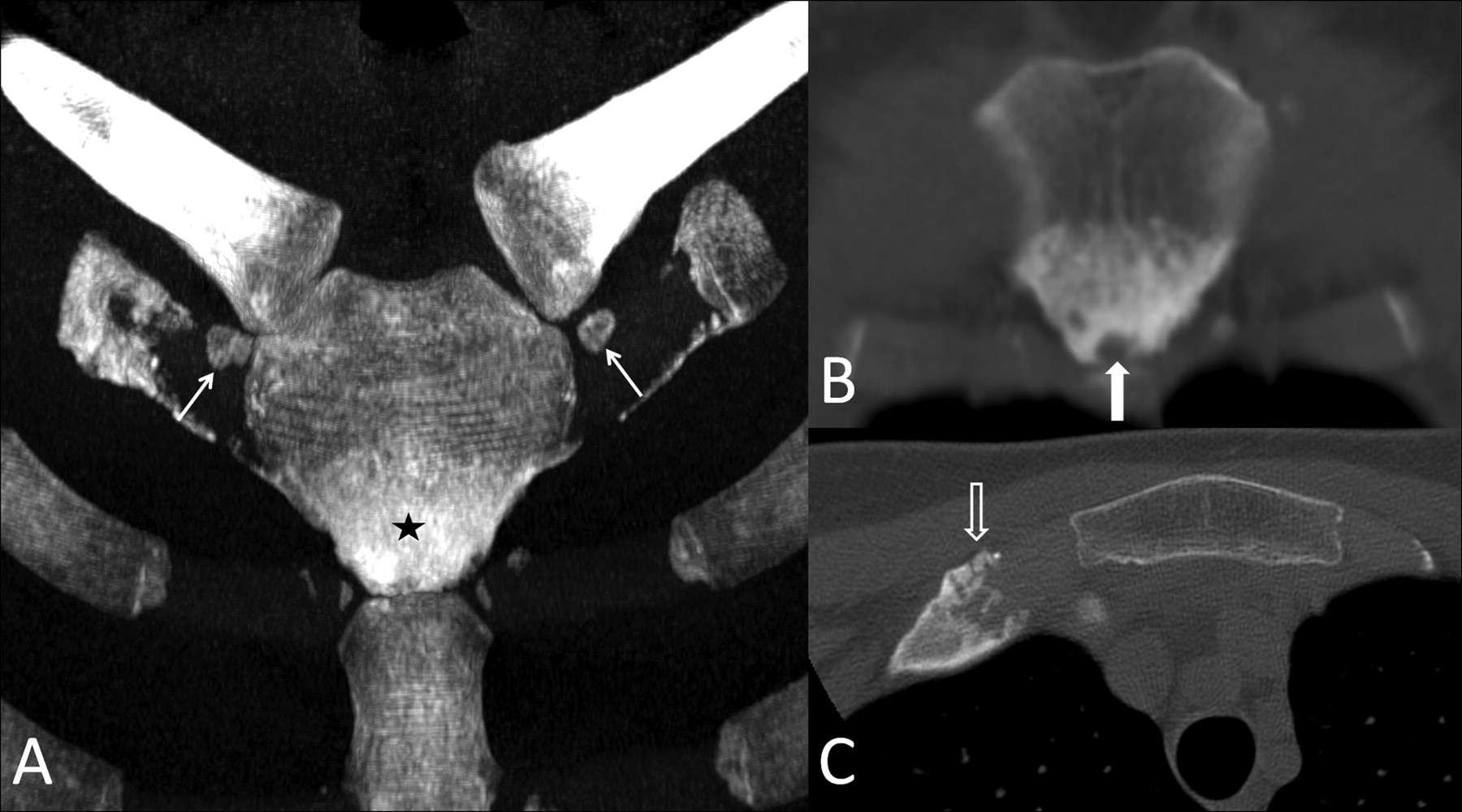
Volume-rendered computed tomography (CT) image (A) showing osteitis condensans of the sternal manubrium (black star) and bilateral ossification of the costoclavicular ligaments (arrows). The coronal reformatted (B) and the axial (C) CT images reveal an erosion of the sternomanubrial joint (white arrow) and partial ossification of the first right costochondral junction (black arrow).
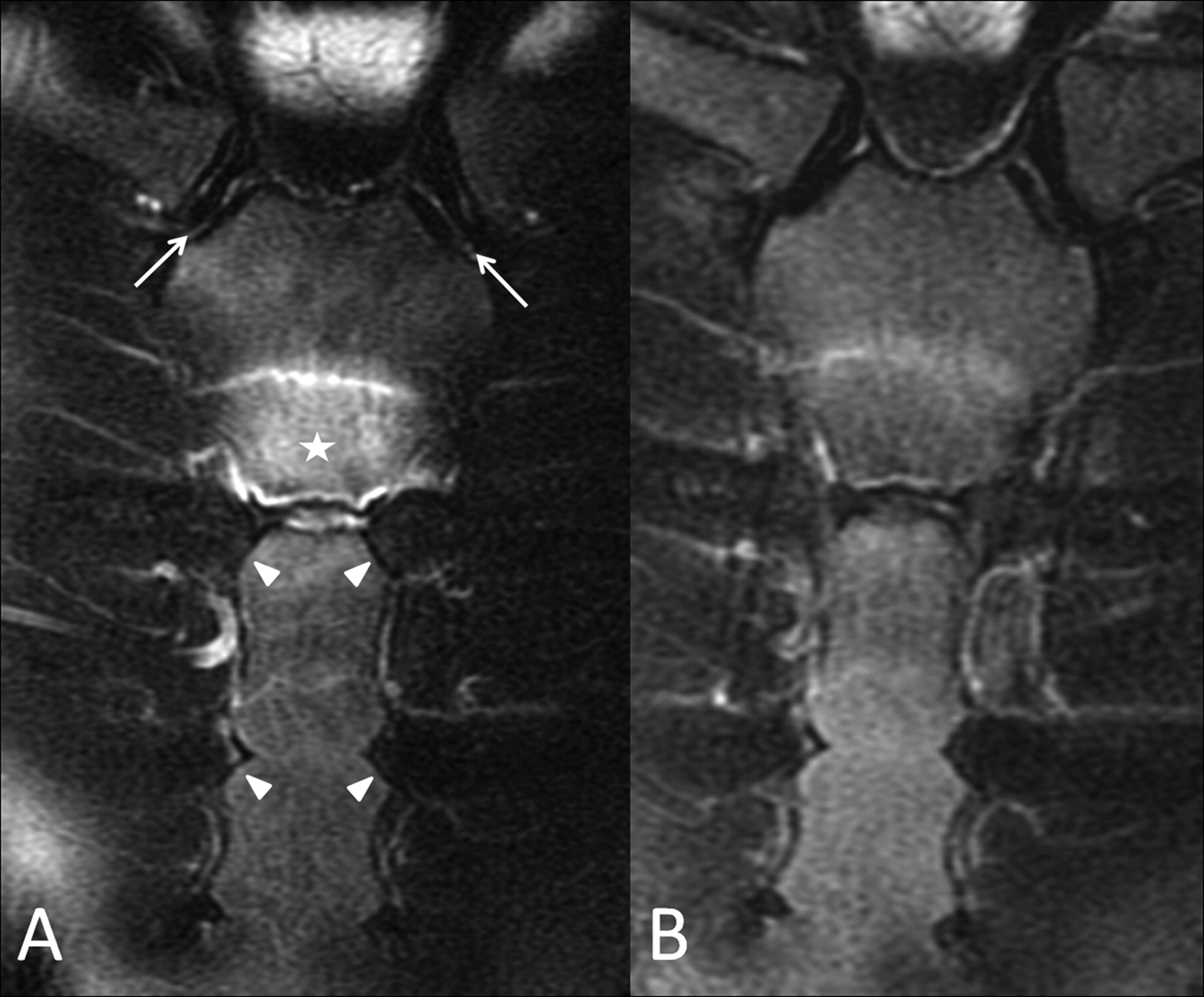
MRI fast spin-echo T2-weighted coronal sequences with fat saturation before (A) and after (B) 4 months of treatment with pamidronate, showing marked reduction of the bone marrow edema involving the sternal manubrium (white star in A). Both sternoclavicular joints and sternochondral junctions were unremarkable (arrow and arrowheads in A, respectively).
The clinical and radiological features of our patient were consistent with the diagnosis of SCCH1, which is frequently associated with peculiar skin lesions (i.e., palmoplantar pustulosis, acne conglobata, acne fulminans) and pathologically characterized by neutrophilic pseudoabscesses2.
SCCH can occur even without neutrophilic skin lesions, and patients who present with bone lesions alone may develop cutaneous manifestations over time2.
The patient was initially treated with a nonsteroidal antiinflammatory drug (meloxicam 15 mg/day) and a cycle of 6 consecutive monthly infusions of 30 mg of the bisphosphonate disodium pamidronate, a potent inhibitor of accelerated bone turnover3. She reported excellent relief of symptoms, and 4 months after her first pamidronate infusion, MRI showed marked reduction of sternal manubrium bone marrow edema (Figure 2B).








{kind=link}
{kind=link}