

Abstract
Objective. To describe 3 cases of scleritis associated with etanercept use for rheumatoid arthritis (RA) and to review the literature related to inflammatory eye diseases associated with the use of etanercept.
Methods. Three cases of severe scleritis during etanercept therapy were analyzed. A systematic review of the literature in PubMed, Embase, and the Cochrane Library was performed, from 1962 to July 2010.
Results. Three patients with seropositive RA developed scleritis 7–28 months after initiation of etanercept, for the first time during their long-lasting disease. In all patients the underlying disease had responded well to anti-tumor necrosis factor therapy. Ocular inflammation went into remission after discontinuation of etanercept, and no other relapses were observed. One patient experienced a dechallenge-rechallenge phenomenon (improvement in symptoms following discontinuation of the agent, then reappearance or worsening of symptoms on reexposure to the agent). Forty-two cases of inflammatory eye diseases believed to be associated with the use of etanercept have been reported in the literature: 33 uveitis, 8 scleritis, 1 orbital myositis, concerning 16 patients with RA, 10 with juvenile idiopathic arthritis, 14 with ankylosing spondylitis, and 2 with psoriatic spondyloarthropathy. Dechallenge was performed in 28 patients, leading to resolution of symptoms. Rechallenge was done in 6 cases, with clear exacerbation.
Conclusion. Ocular inflammation is paradoxically a potential adverse effect of etanercept, even in previously uninvolved eyes.
The widespread use of tumor necrosis factor-α (TNF-α) blockers has led to the recognition of paradoxical adverse effects, defined as the onset or exacerbation of disorders that are usually improved by TNF-α antagonists. Cutaneous psoriasis, Crohn’s disease, and uveitis exacerbations have been extensively reported. Scleritis, a serious and vision-threatening ocular disease, has recently been described as another possible paradoxical effect of anti-TNF-α agents and particularly of etanercept1. Scleritis is a destructive inflammatory eye disease characterized by scleral edema and inflammatory cell accumulation in the sclera. Untreated, the inflammatory process may extend to adjacent tissues, causing uveitis, glaucoma, retinal detachment, and perforation of the globe. About 50% of cases are idiopathic, with the majority of the others having an associated systemic connective tissue disorder. In about half of these patients, the systemic illness is a nodular seropositive RA. The overall prevalence of scleritis in patients with RA is reported to range from 0.67% to 6.3%2,3.
We describe 3 cases of severe anterior scleritis following the administration of etanercept for RA. The scleritis was temporally related to etanercept injections. Drug discontinuation resulted in rapid resolution. We systematically reviewed the literature concerning inflammatory eye disease associated with the use of etanercept: 42 cases were identified and will be reviewed.
MATERIALS AND METHODS
Study selection
A systematic literature search was performed in PubMed Medline, Embase, and Cochrane Library databases from 1962 to July 2010 without a limit on years of publication or journal, using the following key words: “scleritis” (MeSH Terms) OR “scleritis” (All Fields) OR “uveitis” (MeSH Terms) OR “uveitis” (All Fields) OR “orbital myositis” (MeSH Terms) OR “orbital” (All Fields) AND “myositis” (All Fields) OR “orbital myositis” (All Fields) OR ocular (All Fields) AND “inflammation” (MeSH Terms) OR “inflammation” (All Fields) AND “TNFR-Fc fusion protein” (Substance Name) OR “TNFR-Fc fusion protein” (All Fields) OR “etanercept” (All Fields). The limits were English or French languages. In addition, reference lists of the reports initially found were hand-searched to identify additional relevant reports. We also included abstracts of the American College of Rheumatology (ACR) and European League Against Rheumatism meetings from 2006 to 2010. The inclusion criteria were all articles with case reports of inflammatory eye disease with etanercept therapy. The exclusion criterion was a prior eye episode except in flares with dechallenge-rechallenge phenomenon.
Data collection
Two investigators (CGV, CG) selected the articles and collected the data, using a predetermined form. For each case report, these data were collected: demographic characteristics (sex, age), rheumatic disease features and duration, extraarticular manifestation, duration and dose of etanercept treatment before onset of inflammatory eye disease, type of ocular disease, dechallenge-rechallenge, and concomitant treatments [disease-modifying antirheumatic drugs (DMARD), corticosteroids, nonsteroidal anti-inflammatory drugs (NSAID), and bisphosphonates].
RESULTS
Case reports
We identified 3 patients, whose main characteristics were collected retrospectively. All patients had RA, fulfilling the 1989 ACR criteria and resistant to conventional treatment with DMARD.
Patient 1
A 71-year-old man with a 19-year history of positive rheumatoid factor (RF) and anticitrullinated protein antibodies had erosive RA at the time of introduction of etanercept in October 2006. He presented cutaneous nodules as an extraarticular manifestation. Etanercept was given at the dosage of 25 mg twice a week as monotherapy. The treatment was well tolerated and articular manifestations were in remission when unilateral scleritis with uveitis developed in February 2009. He was treated with topical applications of corticosteroids, without any improvement. In March 2009 etanercept was discontinued, with a rapid resolution of ocular symptoms. Three weeks later the sclero-uveitis had disappeared, but the underlying articular disease was in flare. Adalimumab (40 mg/2 weeks) was successful and no ocular relapse was observed at a 1-year followup.
Patient 2
A woman had a 20-year history of RF-positive RA associated with cutaneous nodules and a sicca syndrome. A history of cutaneous vasculitis was noted. She was successfully treated with etanercept 25 mg twice a week for 7 months before developing a bilateral necrotizing scleritis. Ocular manifestations were treated with topical corticosteroids, without success. Systemic corticotherapy was temporarily beneficial, with secondary relapses. Only discontinuation of etanercept allowed remission, after 1 year. She was subsequently treated with infliximab (5 mg/kg) for 4 years and adalimumab (40 mg/2 weeks) for 2 years, and is currently receiving rituximab. No new scleritis relapses were observed.
Patient 3
A 44-year-old woman had erosive RA with positive RF since 1994. She never had extraarticular manifestations. In August 2003, etanercept 25 mg subcutaneously (SC) twice weekly was started, resulting in a dramatic clinical improvement, and within 3 months she went into remission. In November 2005 she developed severe bilateral scleritis with moderate anterior uveitis. She noted a worsening of her eye pain temporally related to etanercept injections and an improvement after transitory (1 week) discontinuation. She was treated with oral indomethacin and topical corticosteroids without efficacy. In May 2006, etanercept was discontinued and her ocular symptoms markedly improved. Because the joint disease flared, she decided to restart etanercept. Within 24 hours she experienced a dramatic ocular inflammation. She was hospitalized and etanercept was withdrawn. Three months later she remained free of ocular inflammation, but the joint disease was still active, despite 2 infusions of 1000 mg rituximab.
Literature search results
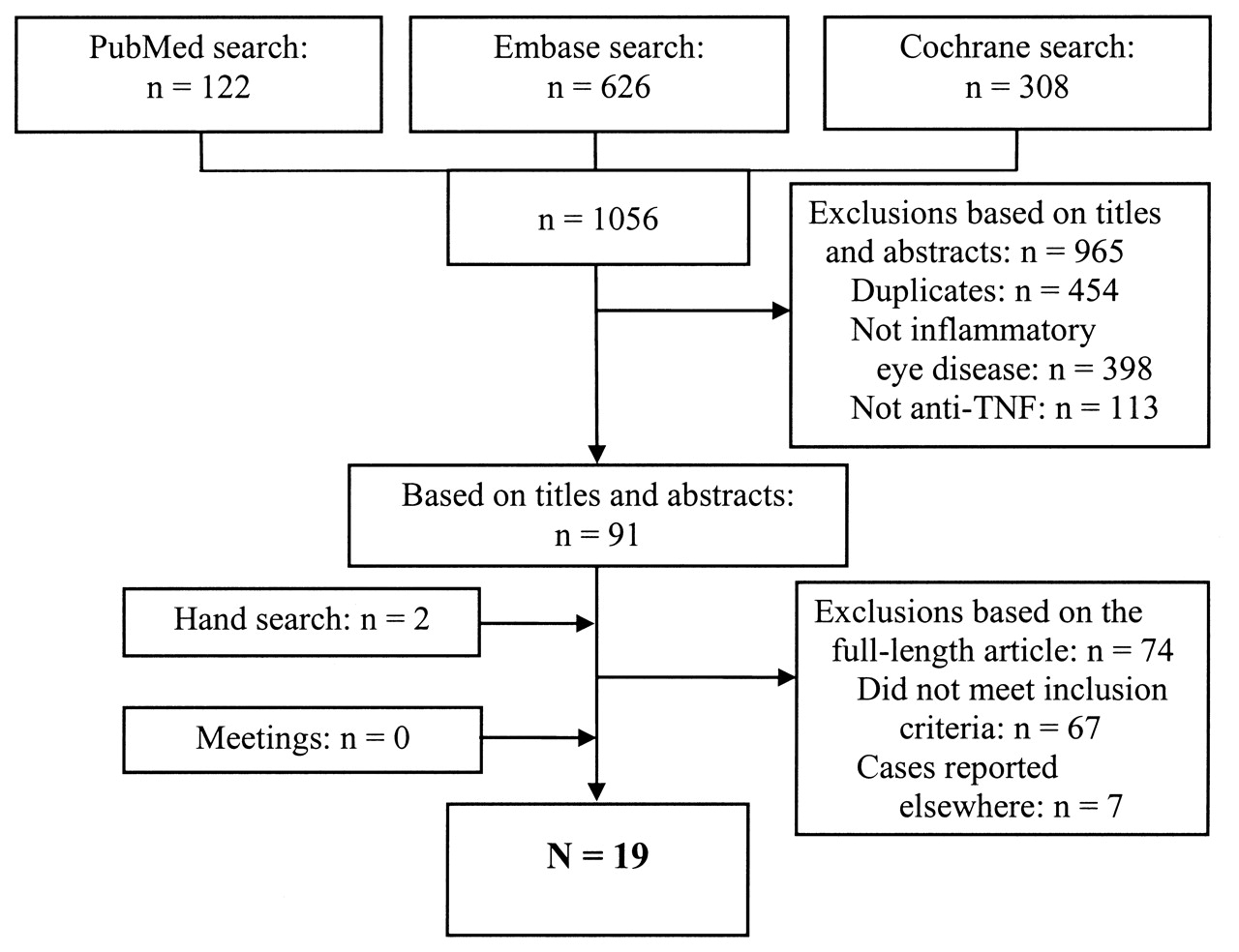
Initially, 1056 potentially relevant articles were screened. Forty-two cases of inflammatory eye disease believed to be associated with the use of etanercept were identified. Figure 1 shows the selection process.

The process of the literature search. TNF: tumor necrosis factor.
Patient characteristics
There were 16 patients with RA, 10 with juvenile idiopathic arthritis (JIA), 14 with ankylosing spondylitis, and 2 with psoriatic arthritis. The characteristics of the patients are given in Table 1. Eye involvement included 33 cases of uveitis, 8 of scleritis, and 1 case of orbital myositis (Table 2). Mean age of the patients was 43.4 ± 13.6 years, and 78% were women. The mean rheumatic disease duration was 11.6 ± 8.9 years.
Characteristics of patients with inflammatory eye disease associated with etanercept reported in the literature.
Subtypes of inflammatory eye diseases associated with etanercept. Results are expressed as mean ± SD.
Drug administration and causality assessment
Etanercept was given according to current dosing, e.g., 25 mg SC twice a week in adults and 0.4 mg/kg for JIA. In 16 patients the dosage was not reported. The average time between the beginning of etanercept therapy and the onset of symptoms was 12.8 ± 9.2 months, with exposure times ranging between 1 and 36 months. Dechallenge (discontinuation of the agent) was performed in 28 patients, leading to resolution of symptoms. Rechallenge (reexposure to the agent) was done in 8 cases, with clear worsening of symptoms in 6 cases. Bisphosphonate use, which can induce uveitis flares, was reported in 1 patient.
DISCUSSION
The potential of anti-TNF-α agents in ophthalmology has been the subject of increasing interest in recent years. All anti-TNF-α drugs currently in clinical use, namely the monoclonal antibodies infliximab and adalimumab, as well as the soluble TNF receptor etanercept, have shown efficacy in treating not only joint inflammation, but also extraarticular manifestations, including uveitis and scleritis.
Saurenmann, et al4 and Tynjala, et al5 analyzed the effects of infliximab and etanercept in cases of childhood uveitis and found that although both agents seemed beneficial, infliximab was associated with better clinical responses in a larger percentage of patients. Braun, et al, using data from recently performed trials, found that reduction of the number of anterior uveitis flares by agents directed against TNF-α was slightly more marked among patients treated with infliximab, but this difference was not significant6. Guignard, et al7, in a retrospective study, and Cobo-Ibanez, et al8, in a prospective study, suggested that anti-TNF antibodies lowered the rate of uveitis flares in patients with spondyloarthropathy, whereas soluble receptor did not seem to lower this rate. Galor, et al9 found a statistically significant superiority of infliximab in the control of ocular inflammation in cases of refractory uveitis. Moreover, in a recent registry-based study, Lim, et al10 reported a significantly greater number of cases of uveitis with etanercept in comparison with infliximab and adalimumab. Based on the results derived from 16 patients with rheumatic diseases, Smith, et al suggested that etanercept has limited efficacy for ocular inflammation even when it has efficacy for systemic disease11. The information on adalimumab for ocular disease is still very limited, although recently Restrepo and Molina reported a successful treatment of severe nodular scleritis with this agent12.
The first hypothesis that we can formulate to explain ocular involvement despite articular improvement with etanercept is that antibody-based TNF-α inhibition is superior to receptor decoy therapy for the treatment of ocular inflammation occurring in the course of rheumatic disease.
The alternative hypothesis, supported by the dechallenge-rechallenge phenomenon observed, is that scleritis can be a paradoxical effect of etanercept. Attribution analysis proposed by Miller, et al13 is a method to evaluate the likelihood of an association between an environmental exposure and an adverse event in rheumatic-related disease. According to the criteria of Miller, the specified primary attribution elements include temporal association, lack of likely alternative explanations, dechallenge (improvement in symptoms following discontinuation of the agent), rechallenge (reappearance or worsening of symptoms on reexposure to the agent) and biological plausibility (the likelihood of the agent causing the signs and symptoms, based on its known in vivo and/or in vitro effects).
The 5 primary elements of the attribution analysis suggest a relationship between etanercept and scleritis. Regarding the temporal relationship, the average time between the beginning of therapy and the onset of symptoms was 12.8 months, with exposure times ranging between 1 and 36 months. Patient 3 developed notable worsening of scleritis the day following the administration of etanercept. No likely alternative explanations could be elicited, except RA. A critical attribution element was the dechallenge-rechallenge phenomenon. A rechallenge effect was noted in scleritis for the first time in Patient 3 as well as in the 6 cases of uveitis reported by Taban, et al14, Reddy and Backhouse15, Coates, et al16, Lim, et al10, and Galor, et al9. In our 3 patients and in 28 patients from the literature, withdrawal with or without other measures resulted in either complete or partial improvement of eye symptoms.
Concerning biological plausibility, difficulties in explaining the underlying pathogenetic mechanism of etanercept-induced scleritis arise from a limited knowledge of the physiopathology of scleritis. A study showed that ocular infiltrating T cells from patients with active uveitis stimulated in vitro with soluble TNF-α receptors began to synthesize TNF-α17. Soluble receptors influence TNF-α activity in vitro and in vivo and maintain the balance between active, free TNF-α and the inactive form bound to its soluble receptors. The soluble forms in high concentrations act as inhibitors by competing with TNF-α cell-surface receptors. However, in lower concentrations, soluble receptors can prolong the biologic half-life of TNF-α by functioning as a carrier protein, protecting TNF-α from degradation and therefore stabilizing its activity18.
Another explanation is that TNF-R p55 is the most biologically active of the 2 receptors but that TNF-R p75 has a 5-fold higher affinity for TNF-α. When TNF-α levels are low, p75 TNF-R facilitates p55 TNF-R activity possibly by a ligand-passing mechanism or as a result of intracellular kinase activation19. Increasing levels of soluble p75 TNF-R by administering etanercept (p75 receptor fusion protein), or decreasing levels of circulating TNF-α by administering infliximab, may interfere with immune homeostasis and disease pathogenesis by as-yet undefined mechanisms, to potentially exacerbate a patient’s underlying tendency to develop inflammatory ocular disease.
These case reports and review raise the possibility that etanercept may precipitate an inflammatory reaction in pre-disposed individuals. However, this review had some limitations, including the retrospective design, the small number of reports, multiple observers, variable followup intervals, heterogeneity of the form of ocular inflammation, the type of systemic association, the population characteristics, and the difficulty in distinguishing an ocular inflammation related to a joint disease and an adverse event.
Ocular inflammation is paradoxically a potential adverse effect of etanercept even in previously uninvolved eyes. Patients being treated with TNF-α soluble receptors should be closely monitored for the development of ocular signs and symptoms in order to detect flares secondary to etanercept therapy.
- Accepted for publication September 20, 2011.








{kind=link}