

Abstract
Objective. Nonsteroidal antiinflammatory drugs (NSAID) are among the most common medicines used by pregnant women. Published data are controversial regarding fetal safety following intrauterine exposure to NSAID. We investigated exposure to NSAID in the first trimester in a large cohort of infants and fetuses.
Methods. A computerized database of medications dispensed from 1998 to 2009 to all women registered in the “Clalit” health maintenance organization in Southern Israel was linked with 2 computerized databases containing maternal and infant hospitalization records. Pregnancy terminations for medical reasons were analyzed. The following confounders were controlled for: parity, maternal age, ethnicity, maternal pregestational diabetes, maternal inflammatory disease, and year of birth or pregnancy termination. First trimester exposure to nonselective cyclooxygenase (COX) inhibitors and to selective COX-2 inhibitors as groups and to individual drugs was analyzed.
Results. There were 110,783 pregnancies during the study period: 109,544 singleton births and 1239 pregnancy terminations for medical reasons. In total, 5267 mothers were exposed to NSAID during the first trimester of pregnancy: 5153 to nonselective COX inhibitors and 114 to COX-2 selective inhibitors. Exposure to NSAID in the first trimester, as groups (nonselective COX and selective COX-2 inhibitors) and as individual drugs, was not associated with an increased risk of major congenital malformations in general (adjusted OR 1.07, 95% CI 0.96−1.21 for nonselective; and adjusted OR 1.40, 95% CI 0.70−2.78, for selective COX-2 inhibitors), although an increased risk for musculoskeletal malformations was found following exposure to COX-2 selective inhibitors (adjusted OR 3.39, 95% CI 1.37−8.34).
Conclusion. Intrauterine exposure to NSAID was not associated with increased risk for major congenital malformations. Further studies are needed to assess the risk for malformations after exposure to COX-2 selective inhibitors.
Nonsteroidal antiinflammatory drugs (NSAID) are among the drugs most widely used by women during the first trimester of pregnancy1. This chemically heterogeneous group of drugs, which acts by inhibiting production of prostaglandins through inhibition of cyclooxygenases (COX) 1 and 2, is indicated mostly for their antipyretic, analgesic, and antiinflammatory effects2. NSAID are divided functionally into 2 major classes: ibuprofen, indomethacin, naproxen, diclofenac, etodolac, lornoxicam, and nabumetone are classified as nonselective COX inhibitors, while celecoxib, etoricoxib, and rofecoxib are classified as COX-2 selective inhibitors.
Several studies have assessed the risk of major congenital malformations after exposure to nonselective COX inhibitors during the first trimester of pregnancy. Three studies3,4,5 have detected an increased risk for cardiac malformations, orofacial clefts, gastroschisis, and major malformations in general after exposure to ibuprofen, diclofenac, and indomethacin, while 3 other studies6,7,8 failed to detect such risk. To our knowledge, no study has reported on the fetal safety of any COX-2 selective inhibitor.
We report the results of a large population-based cohort of pregnant women, attempting to quantify fetal risks following exposure to NSAID.
MATERIALS AND METHODS
A population-based retrospective cohort study was conducted, including all women 15−45 years of age who were registered in Clalit Health Services, Beer Sheva, and had a singleton delivery or a pregnancy termination for medical reasons at Soroka Medical Center (SMC), Beer Sheva, between January 1, 1998, and December 30, 2009. Clalit Health Services is the largest health maintenance organization in the country, in which 70% of the women in the southern district of Israel aged 15−49 years are insured. SMC is the regional hospital, in which 98% of the deliveries take place.
We linked 3 computerized databases that draw information directly from original sources — 2 from SMC and one from Clalit Health Services. The Obstetrics and Gynecology Department deliveries database includes maternal demographic information, including mother’s age and ethnic group (Jewish or Bedouin Muslim), parity, health status during pregnancy and delivery, self-report smoking status during pregnancy, gestational age at delivery, and delivery results (perinatal death, infant’s birth weight, and APGAR score at 1 and 5 min). The diagnoses are reviewed routinely by a trained medical secretary before entry into the database. Information regarding major malformations diagnosed in newborns or infants until the age of 12 months was collected from the Demog-International Classification of Diseases-9 (ICD-9) database, which includes demographic and medical information of patients admitted to SMC. Information on drugs dispensed to mothers during the first trimester of pregnancy was collected from the Clalit Health Services medication database, including the date the drug was dispensed, the Anatomical Therapeutic Chemical classification codes of the drugs (including the commercial and generic names), the dose schedule, and the dose dispensed in terms of the defined daily dose (DDD; i.e., the assumed average maintenance dose per day). A fourth database, which included data on pregnancy terminations done for medical reasons, was searched manually from the registry of the Committee for Termination of Pregnancies at SMC.
The 4 databases were encoded and linked by personal identification numbers (numbers assigned at birth by the Interior Ministry and used throughout life) to create a registry of medications dispensed during the first trimester of pregnancy and of pregnancy outcomes. We used the unique identification number of the hospitalization given at SMC to the mother and to the newborn to link the mother and the infant’s identification number.
The study was approved by the local institutional ethics committee in accord with the principles of the Declaration of Helsinki. In accord with Ministry of Health regulations, the institutional ethics committee did not require written informed consent because the data were obtained anonymously from medical files, with no participation of patients.
Study design
Two main exposure groups were defined according to the type of NSAID the woman was exposed to during the first trimester: the nonselective COX inhibitors group comprised infants or fetuses exposed in utero to ibuprofen, diclofenac, naproxen, indomethacin, etodolac, lornoxicam, or nabumetone; whereas the COX-2 selective inhibitors group comprised those exposed to celecoxib, etoricoxib, or rofecoxib during the first trimester of pregnancy. Infants or fetuses not exposed to any of the drugs during the first trimester were classified as the unexposed group. Analysis also investigated specific drugs from the nonselective COX inhibitors group. An infant or fetus was defined as exposed if an NSAID was dispensed to the mother during the first 13 weeks of pregnancy. The first day of the last menstrual period was defined as the first day of gestation.
First trimester exposure to NSAID was also characterized by the total number of DDD dispensed. DDD for prescription NSAID are as follows9: ibuprofen 1200 mg, diclofenac 100 mg, indomethacin 100 mg, naproxen 500 mg, etodolac 400 mg, lornoxicam 12 mg, nabumetone 1000 mg, etoricoxib 400 mg, celecoxib 200 mg, and rofecoxib 25 mg. The total DDD dispensed during the first trimester were stratified into 3 categories: 1 to 5, 6 to 10, and 11 and more. Some women in the cohort were also exposed to other medications during the first trimester of pregnancy.
We investigated the risk for major malformations after exposure to NSAID during the first trimester of pregnancy for singleton live births or stillbirths, and for pregnancy terminations for medical reasons. We used the definitions of major and minor congenital malformations developed by the Metropolitan Atlanta Congenital Defects Program of the Centers for Disease Control and Prevention10,11,12. Chromosomal diseases were excluded. In subclass analyses of major malformations, the following specific defects were examined: anencephaly (ICD-9 code 740); spina bifida (741); other anomaly of the nervous system (742); anomalies of the eye (743); anomalies of the ear, face, and neck (744); bulbus cordis anomalies and anomalies of cardiac septal closure (745); other anomalies of the heart (746); other anomalies of the circulatory system (747); anomalies of the respiratory system (748); cleft palate and lip (749); other anomalies of the upper alimentary tract (750); other anomalies of the digestive system (751); genital anomalies (752); anomalies of the urinary system (753); musculoskeletal deformities (754); other anomalies of the limbs (755); other musculoskeletal anomalies (756); and anomalies of the integument (757). Congenital malformations were diagnosed by board-certified neonatologists at the SMC neonatology unit.
Statistical analysis
We used the SPSS program, version 17 (IBM SPSS), for statistical analysis. Characteristics of mothers from the exposed and unexposed groups were compared by chi-square or Fisher’s exact tests for categorical variables and the Student t test for continuous variables. We used a multivariate logistic-regression model to determine whether exposure to NSAID was independently associated with an increased risk of major congenital malformations adjusting for maternal age, parity, ethnic group (i.e., Jewish vs Bedouin Muslim), pregestational diabetes mellitus, maternal inflammatory disease, and year of birth or pregnancy termination. A categorical multivariate logistic-regression model was constructed to determine whether greater exposure in terms of DDD was associated with an increased risk for major congenital malformations. OR and 95% CI were computed.
RESULTS
There were 109,544 singleton births and 1239 pregnancy terminations (468 because of fetal malformation and 771 other medical causes) at SMC between 1998 and 2009. Overall, 5153 (4.65%) women were exposed to nonselective COX inhibitors and 114 (0.01%) were exposed to COX-2 selective inhibitors during the first trimester of pregnancy.
Comparison of maternal characteristics among the 2 exposed groups and unexposed mothers is presented in Table 1.
Characteristics of women exposed to nonselective COX inhibitors or COX-2 selective inhibitors, and unexposed women*.
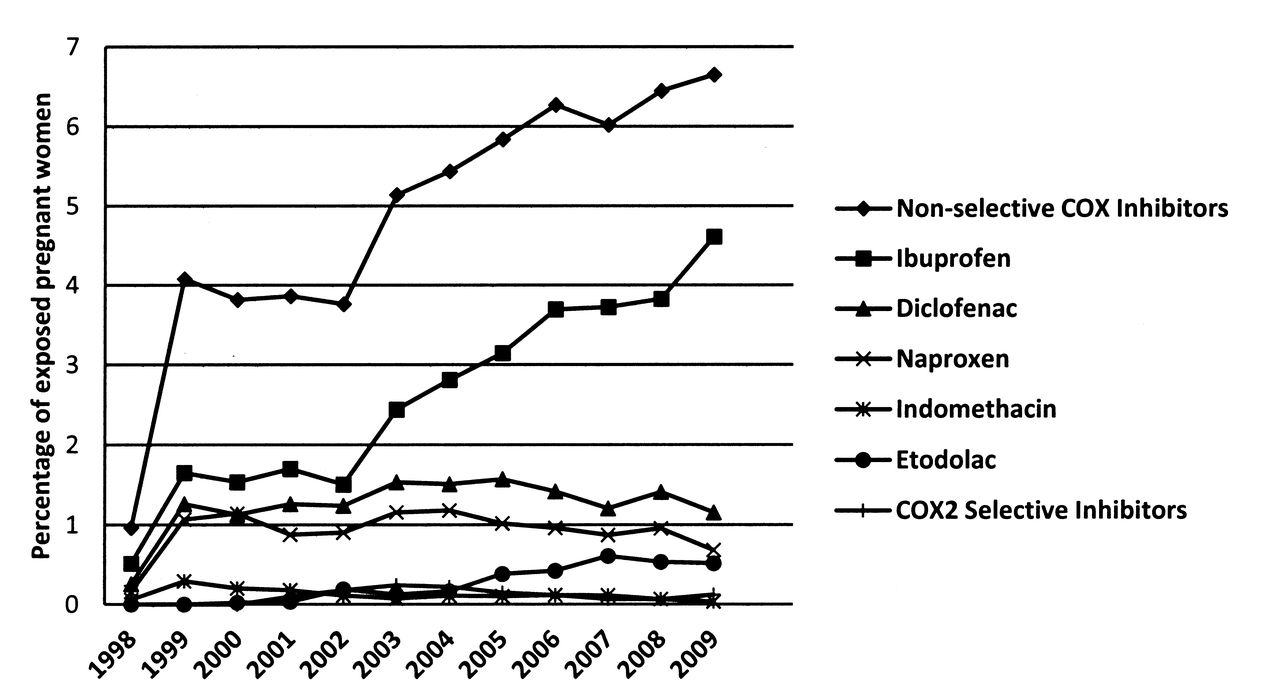
The use of NSAID by women during the first trimester of pregnancy increased sharply between 1998 and 2009, predominantly due to the rising use of ibuprofen, which was the most commonly dispensed NSAID during those years (Figure 1).

Exposure rates of pregnant women to whom NSAID were dispensed during the first trimester of pregnancy, according to the birth year of their offspring or year of pregnancy termination. NSAID: nonsteroidal antiinflammatory drugs; COX-2: cyclooxygenase-2 inhibitors.
A total of 6505 (5.9%) infants and fetuses were diagnosed with 1 or more major congenital malformations until 12 months of age: 2751 (2.5%) exhibited cardiovascular system malformations, 1615 (1.45%) had musculoskeletal malformations, 942 (0.85%) had central nervous system defects, 495 (0.45%) had genital malformations, 405 (0.36%) were diagnosed with urinary system malformations, 349 (0.31%) had gastrointestinal tract malformations, 290 (0.26%) exhibited respiratory malformations, 146 (0.13%) had cleft palate, 28 (0.025%) had integument system malformations, and 27 (0.02%) had ear, face, and neck malformations.
The unadjusted and adjusted risk for major congenital malformations following exposure to NSAID during the first trimester of pregnancy is presented in Table 2. The rate of major malformations in the nonselective NSAID-exposed group was 6.5% (336 of 5152) compared to 5.8% (6164 of 105,537) in the unexposed group (crude OR 1.13, 95% CI 1−1.26; adjusted OR 1.07, 95% CI 0.96−1.21). The rate of major malformations in the COX-2 selective inhibitors exposure group was 7.9% (9 of 114) compared to 5.8% (6164 of 105,537) in the unexposed group (crude OR 1.38, 95% CI 0.69−2.73; adjusted OR 1.4, 95% CI 0.7−2.78). No association was found between exposure to any specific NSAID during the first trimester of pregnancy and major malformations. Further, excluding exposures during the first 4 weeks of pregnancy or including exposures 4 weeks before the first day of the last menstrual period yielded similar results.
The risk for major malformations in infants or fetuses after exposure to NSAID, compared to nonexposed.
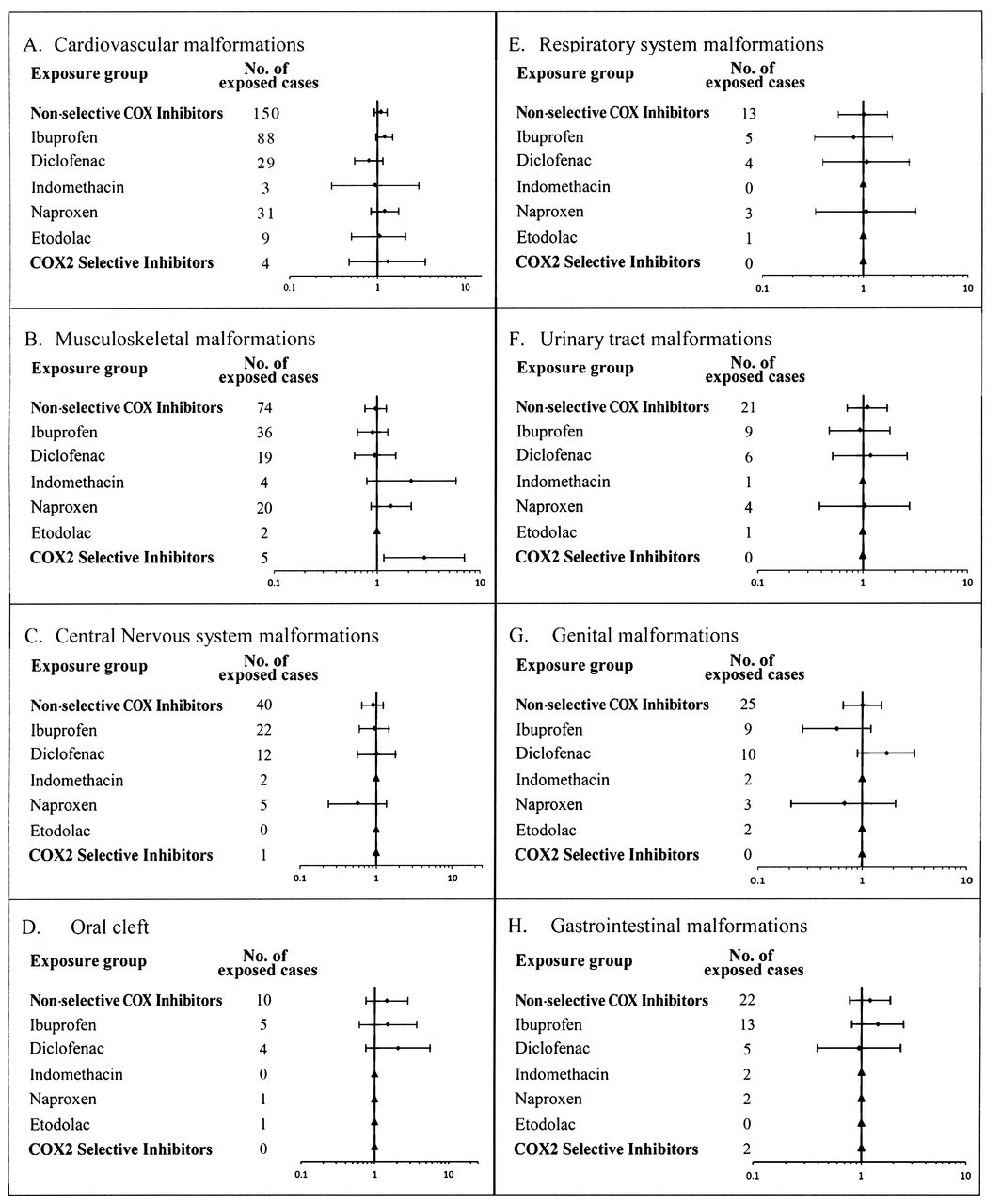
No increased risk was detected, before or after adjustment, for any subgroup of malformation with exposure to any type of NSAID on the first trimester of pregnancy (Figure 2), although an increased risk for musculoskeletal malformations was found following exposure to COX-2 selective inhibitors (adjusted OR 3.39, 95% CI 1.37−8.34).
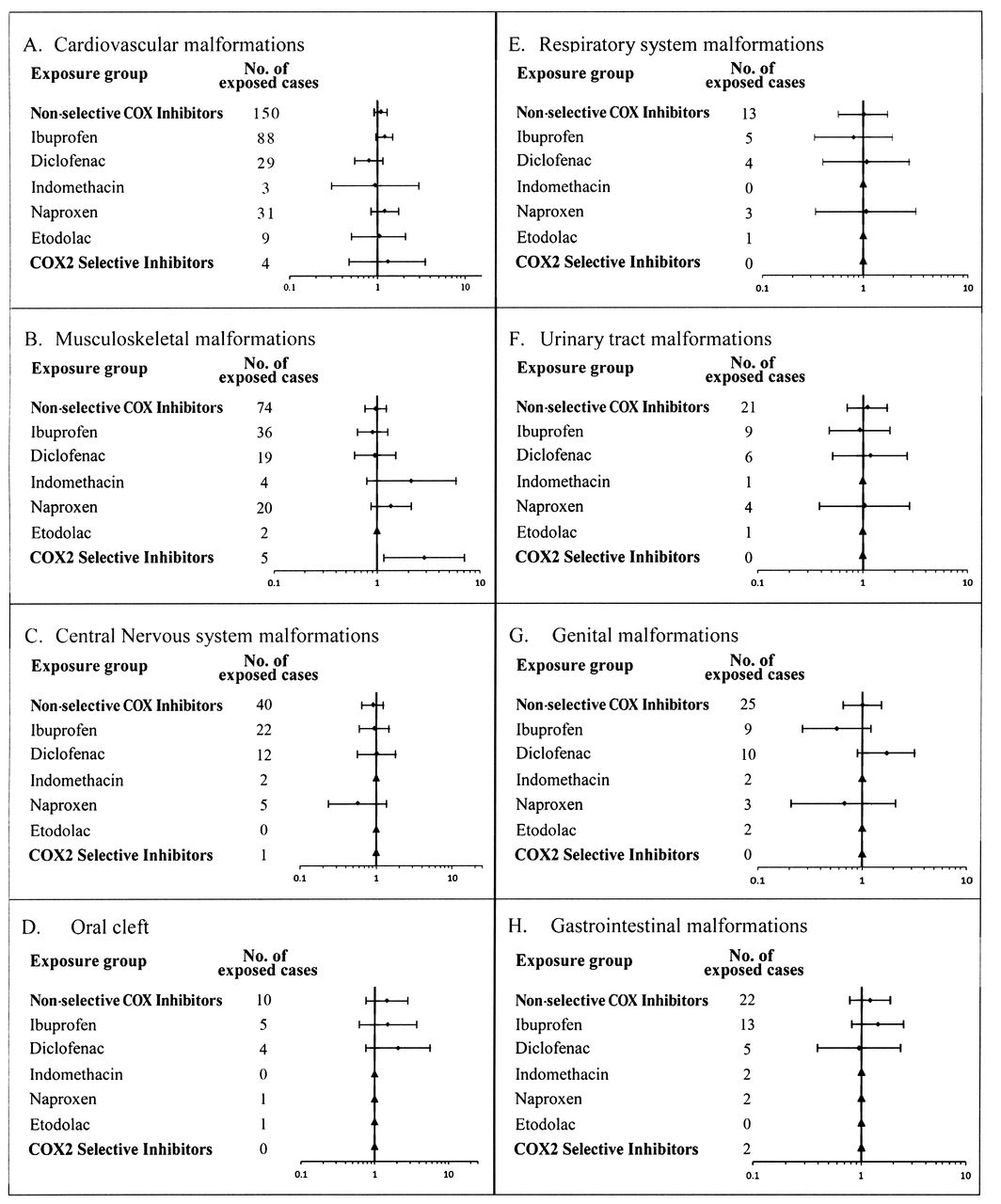
Adjusted OR for major malformations categorized by 8 organ systems following exposure to NSAID during the first trimester of pregnancy; OR were adjusted for maternal age, parity, ethnic group, pregestational diabetes mellitus, maternal inflammatory disease, and year of birth or termination of pregnancy. ▴ OR was not calculated because of fewer than 3 exposed cases. NSAID: nonsteroidal antiinflammatory drugs; COX: cyclooxygenase inhibitors.
There was no significant dose response in the association between NSAID and major malformations in univariate analyses, or after adjustment using a categorical multiple logistic regression (Table 3).
The risk for major malformations following first trimester exposure to NSAID stratified by defined daily dose (DDD)*.
DISCUSSION
Our study shows a steady increase in the use of NSAID among women in the first trimester of pregnancy. Despite this, our population-based retrospective cohort study failed to detect increased risk for major malformations following exposure to nonselective NSAID during the first trimester of pregnancy. Moreover, no association was found between nonselective NSAID and subgroups of malformations according to organ systems.
Our cohort included both infants born in singleton deliveries and fetuses from pregnancy terminations for medical reasons, which explains the relatively high rate of malformations as compared to other studies13. Further, malformations were documented not only in the neonatology unit after delivery, where all infants are examined by board-certified neonatologists, but also during hospitalizations up to 12 months of age. Previous studies have documented higher rates of malformations among Bedouin children as compared to Jewish14,15, a finding that has been attributed to high rates of consanguinity among Bedouins.
Our findings are consistent with 3 previous studies, 2 cohort studies6,7, and a case-control study8. In contrast, 3 studies have reported an increased risk for major malformations after exposure to NSAID during the first trimester of pregnancy. In a population-based cohort study3, an increased risk for cleft palate was found following first trimester use of naproxen (OR 2.61, 95% CI 1.01−6.78), although no significant association was found between the use of NSAID and major malformations in general. The second, a population-based nested case-control study4, reported a significantly increased risk for major malformations following exposure to NSAID (OR 2.21, 95% CI 1.72−2.85). The study included only 30% of the provincial population, all of whom were insured by the public health insurance program because of low socioeconomic class, as compared with our study, which included about 70% of the district population of all socioeconomic classes. The third, a nested case-control study5, found a significantly increased rate of first trimester ibuprofen use among mothers of newborns diagnosed with gastroschisis compared to matched healthy newborns. Exposure was assessed by an interview with the mother after delivery, with a possibility for recall and reporting bias. All 3 studies did not adjust for multiple deliveries or diabetes mellitus, both known to be significantly associated with major malformations.
Our study is the only one to include data derived from pregnancy terminations for medical reasons, and data for major malformations were collected up to 12 months of age. Our results are corroborated by dose-response analysis conducted for the drugs’ DDD. Enrolling 5267 infants and fetuses exposed to NSAID during the first trimester of pregnancy, our study is by far the largest to date. Further, no published study to date assessed the fetal safety of exposure to COX-2 selective inhibitors or to etodolac.
Our study found an increased risk for musculoskeletal malformations following exposure to COX-2 selective inhibitors. This finding was based on a total exposure number of 114 and only 5 exposed cases, and therefore can be the result of a small exposure group or of multiple comparisons. Further studies are needed to assess the risk for malformations after exposure to COX-2 selective inhibitors.
A potential limitation of our study is that ibuprofen has also been available as an over-the-counter drug. The possibility that this medication was dispensed to pregnant women in pharmacies outside Clalit Health Services cannot be ruled out. In this case, infants or fetuses that were classified as unexposed in our study could have been exposed to the drug during the first trimester, creating a bias toward the null hypothesis. However, a subanalysis that included only prescription NSAID showed similar results, making ibuprofen teratogenicity unlikely. To address the potential effect of misclassification of those exposed into the unexposed group because of over-the-counter use of NSAID, we conducted the following sensitivity analysis. Assuming that nonselective NSAID were indeed a human teratogen causing an extreme of 10% malformation rate and that the number of fetuses that were exposed to NSAID was doubled (i.e., to 10,304), 50% of them were misclassified to the unexposed group: in this extreme scenario, the nonexposed group erroneously absorbs 515 malformed babies. These 515 malformed cases would increase the malformation rate in the unexposed group from 5.8% (i.e., 6164 of 105,537) malformed fetuses to 5.9% (i.e., 6279 malformed), which would decrease the teratogenic signal in the exposed group very marginally. Hence, even such an overt misclassification should not decrease the theoretical 10% malformation rate in the exposed group, because it would be grossly diluted by the 100-fold unexposed group (as shown in this sensitivity exercise).
Although it was not statistically significant, we found a relatively high OR for major malformations following exposure to indomethacin. There were only 12 exposed cases in the indomethacin subgroup (12/128, 0.093%; adjusted OR 1.76, 95% CI 0.96−3.19), divided sporadically among the various organ systems. Further, OR for malformations according to organ systems were lower. Therefore, the biological and statistical probability of an increased risk for malformations following exposure seems to be very low, suggesting that the nonsignificant OR of 1.76 is likely a random finding.
Our study used information on drugs dispensed for pregnant woman from the Clalit Health Services medication database; hence data regarding adherence to therapy were not available. However, previous studies using the same database found the rate of medication adherence to be higher than 90% for subgroups of women with deep vein thrombosis (DVT) and familial Mediterranean fever (FMF)16. Since DVT and FMF are serious medical conditions, it is unclear whether these high adherence rates can be generalized to women with indications for NSAID. Another study that used the same medication database found high rates of adherence for iron supplementation dispensed for Israeli children, as confirmed by laboratory tests17. Further, previous studies showed computerized pharmacy records had high rates of concordance with medication use in general18,19,20 and by pregnant women specifically21.
Our study lacks data about maternal febrile diseases or pain during the first trimester of pregnancy; therefore we could not address those indications of use in our data analysis. On the other hand, data regarding maternal inflammatory diseases were included in the analysis.
Some pregnant women in the cohort were exposed to other medications during the first trimester of pregnancy. Since no increased risk was found, those exposures were not excluded from the study. Analysis of the data including exposure to anti-folic acid derivatives yielded similar results.
We did not find an association between first trimester exposure to NSAID and stillbirths or preterm births. Although these adverse pregnancy outcomes may be related to major malformations, including them in data analysis did not change our overall results.
In this large cohort of infants and fetuses we found exposure to NSAID in the first trimester, as groups (nonselective COX and selective COX-2 inhibitors) and as individual drugs, was not associated with an increased risk for major congenital malformations. An increased risk for musculoskeletal malformations was found following exposure to COX-2 selective inhibitors. Further studies are needed to assess the risk for malformations after exposure to COX-2 selective inhibitors.
Acknowledgment
We thank members of the computer units of Clalit Southern District and Soroka Medical Center.
- Accepted for publication July 11, 2012.








{kind=link}
{kind=link}