

Abstract
Objective. Studies have shown that aortitis may be present in half the patients with recent-onset giant cell arteritis (GCA). We assessed whether aortitis at diagnosis affects longterm outcome in patients with GCA.
Methods. We retrospectively analyzed the longterm outcome of a prospective cohort of 22 patients with biopsy-proven GCA who all had aortic computed tomography (CT) evaluation at the time of diagnosis of GCA between May 1998 and November 1999. Longterm outcome, especially vascular events such as aortic aneurysm, mortality, relapses of GCA, and requirement for steroids, was assessed in 2011 by chart review and patient/physician interviews.
Results. At disease onset, 10/22 patients had aortitis on CT scan. Patients with and without aortitis had similar baseline characteristics, including cardiovascular risk profile. At the time of the study, 12/22 (57%) patients had died. Vascular causes of death were more frequent in patients with aortitis (5/7 vs 0/5; p = 0.02). A higher number of vascular events was noted in patients with aortitis (mean events per patient 1.33 vs 0.25; p = 0.009). Stroke was more frequent in patients with aortitis. These patients seemed to exhibit a more chronic or relapsing disease course, and they were less likely to completely discontinue steroid therapy (p = 0.009, log-rank test).
Conclusion. Our study suggests for the first time that inflammatory aortic involvement present at onset of GCA could predict a more chronic/relapsing course of GCA, with higher steroid requirements and an increased risk for vascular events in the long term.
Giant cell arteritis (GCA) is the most common form of systemic vasculitis, involving large and medium-size arteries in people over age 60 years, with a particular tropism for branches of the external carotid arteries1. GCA is a well-known cause of aortitis, which can ultimately lead to life-threatening complications such as aortic dissection or aortic aneurysm rupture and sudden death2,3,4,5,6. According to retrospective studies, aortic involvement occurs in 3%–18% of patients with GCA2,6,7,8,9. However, most authors consider this frequency to be underestimated10,11,12, although prospective imaging studies are scarce. Indeed, in a previous prospective cross-sectional study using aortic computed tomographic (CT) scanning, we showed that abnormal thickening of the aortic wall was present in 45.5% of patients with newly diagnosed GCA, significantly more frequently than in the controls13. Using CT scans, Prieto-González, et al have reported a 65% rate of aortic involvement in GCA14. In other studies using 8-fluorodeoxyglucose positron emission tomography (18F-FDG PET), a similar proportion of patients with GCA was diagnosed with asymptomatic aortic inflammatory involvement12,15,16.
Aortitis can be present at the initial stage of GCA, and may also reveal the disease4,10. However, aortic complications such as aortic aneurysms mostly occur many years after the diagnosis5,6,7,8,9. Longterm followup studies in GCA have to date not included systematic and standardized imaging of the aorta5,17,18,19,20,21. Thus, the longterm prognostic significance of aortic involvement in GCA remains unknown.
In our previous work, we investigated 22 patients with newly diagnosed biopsy-proven GCA and found that almost half (10/22) had aortic involvement on CT scan13. The aim of our present study was to describe the longterm outcome of this cohort, in order to analyze the prognostic significance of initial aortic involvement in GCA.
MATERIALS AND METHODS
Study design
Between May 1998 and November 1999, 22 consecutive patients with newly diagnosed biopsy-proven GCA were included in a prospective aortic imaging study. Aortic helical CT scanning was used to describe aortic wall abnormalities at the time of diagnosis of GCA, and compared to controls13. There were no planned followups after the time of CT scanning in this first study. From January to March 2011, i.e., 12 years later, we undertook this retrospective study to assess patients’ outcome.
Inclusion criteria and baseline investigations
Inclusion and exclusion criteria of the cohort have been reported13. Briefly, all patients were > 55 years of age, had temporal artery biopsy-proven GCA, and fulfilled at least 3 of 5 criteria of the American College of Rheumatology for the diagnosis of GCA. Aortic helical CT scanning was performed within 4 weeks after the diagnosis of GCA, and analyzed by the same radiologist (BD).
Cardiovascular risk factor assessment, detailed cardiovascular examination, and blood tests [C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), fasting blood glucose, and cholesterol level] were performed at baseline, before the initiation of corticosteroid therapy.
Thoraco-abdominal aortic CT scans were analyzed for the presence or absence of aortic aneurysm, ectasia, dissection, stenosis, thrombus, and atherosclerosis. Maximum thickness of the aorta wall was also measured. Thickness of the aortic wall > 2 mm was considered aortic thickening. The following criteria were used to define aortitis: thickening of aortic wall > 2 mm without adjacent atherosclerotic plaque and/or new diagnosis of aortic aneurysm/ectasia. Aneurysm was defined as aortic dilatation with loss of wall parallelism. Abnormal dilatation without loss of wall parallelism was considered as aortic ectasia. Our study design did not include subsequent aortic imaging and hospital physicians in charge of the patients were free to choose how aortic changes were to be monitored.
Each patient provided signed informed consent to participate. The study protocol was approved by the ethics committee of Nantes University Hospital and was in compliance with the Declaration of Helsinki.
Assessment of longterm outcome
In 2011, we investigated the longterm outcome of this cohort by interviewing patients, families, and general practitioners (GP) as well as, if needed, radiologists, vascular surgeons, cardiologists, and angiologists. It should be noted that some of the GP were not aware of whether asymptomatic aortitis had been suspected on initial CT scans. Community-based physicians’ medical charts and hospital discharge letters were sought when needed. Institutional review board approval was obtained for patients’ personal medical data to be reviewed and collected. Data were collected using a standardized form including time and cause of death, detailed cardiovascular events, hospitalization, progression of steroid dosage, and date of definitive discontinuation of corticosteroid therapy. We used the following definition of “definitive steroid discontinuation”: for patients alive at the time of analysis: steroid discontinuation without any new steroid requirement for 6 years (72 months); and for patients deceased at the time of analysis: steroid discontinuation without any new steroid requirement in the 3 months preceding death.
Relapses of GCA were also recorded. Relapses were defined by recurrence of unexplained elevation of inflammatory markers (CRP > 20 mg/l) with symptoms and physical examination signs of GCA, leading a physician to increase or resume corticosteroid therapy. Vascular events were defined as occurrence of aortic dissection and/or aneurysm, occurrence of obliterating arteriopathy, stroke, and coronary artery disease, and were used as specific outcomes in our study. Outcome and cause of death of each patient were systematically separately analyzed by 2 different examiners experienced with GCA (AN, CA).
Data reporting and statistical analysis
Comparisons were made between patients according to aortic involvement at the time of diagnosis of GCA. Categorical variables are expressed as percentages and compared using chi-squared tests or Fisher’s exact tests when any of the expected cell counts of a 2 × 2 table was < 5. Comparisons of quantitative variables were performed using the nonparametric Mann-Whitney U test. All tests were 2-sided and a p value < 5% was considered statistically significant. Survival, steroid discontinuation, and time to first vascular event curves were established using the Kaplan-Meier method and comparisons of curves were by log-rank test.
RESULTS
Cohort characteristics
At diagnosis, 12 patients had no aortic involvement (GCA-noAo), whereas 10 had aortitis (GCA-Ao) including 1 with symptomatic aortitis (dissecting aortic aneurysm). Among the latter, 7 had focal thickening of the wall of the descending thoracic aorta (average thickness 3.28 ± 0.75 mm), 2 had an aneurysm of the ascending thoracic aorta, and 2 had an ectasia of the thoracic aorta. These 4 patients with aortic aneurysm/ectasia all had arterial hypertension. The 2 groups were similar in terms of cardiovascular risk factors, clinical presentation, and inflammatory measures (Table 1). They also received similar initial steroid regimens, i.e., oral prednisone 0.7–1 mg/kg/day. One patient of each group initially received 3 daily intravenous pulses of methylprednisolone 240 mg. For each physician in charge of the patients, the objective was to cure GCA and to try to discontinue steroids after 18–24 months of treatment, independently of aortic status.
Baseline characteristics of patients with (GCA-Ao) and without aortitis (GCA-noAo) at GCA onset. Data represent number (percentage) or mean ± SD.
By February 2011, none of the patients still alive were lost to followup. The mean followup of the overall cohort was 94 months (7.83 yrs). Each patient had undergone regular visits with their GP and comprehensive medical records, including relapses of GCA and dosage of steroids, were available for the analysis.
Survival and vascular events
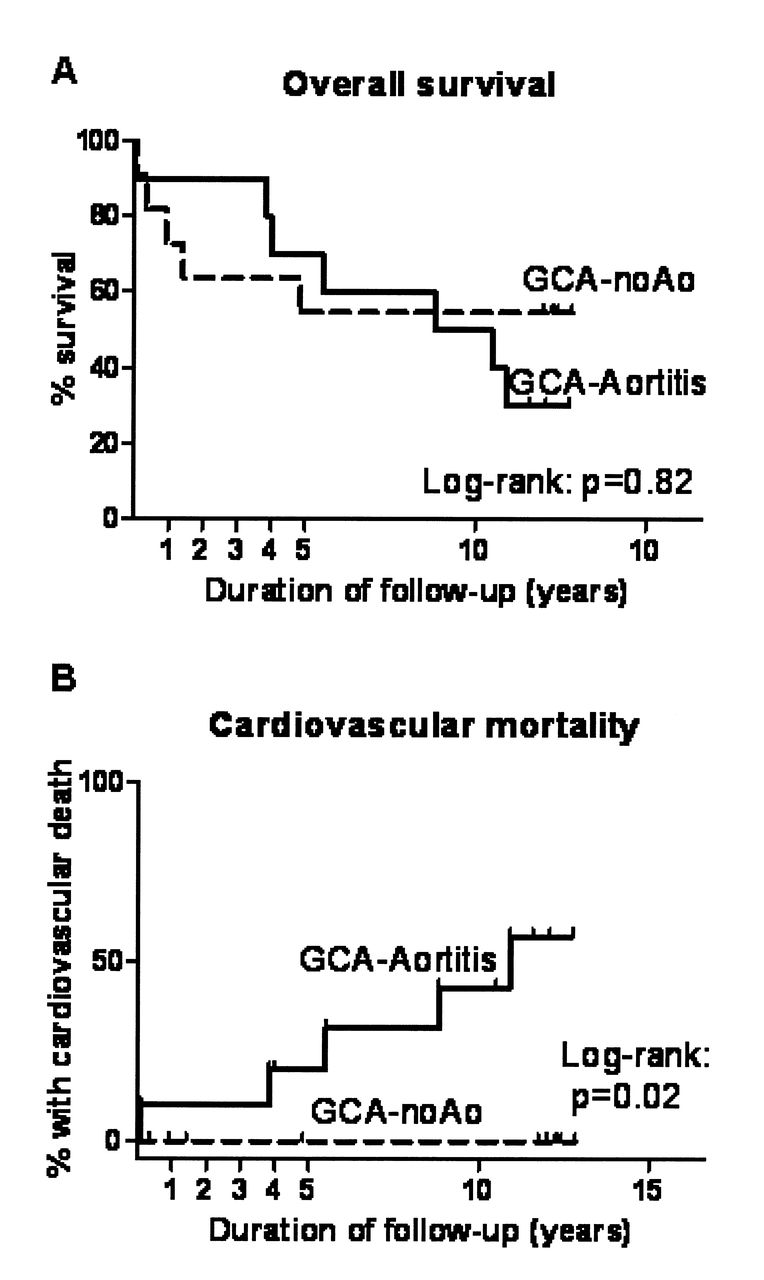
At the time of our study, 54% of patients had died. There were 7 deaths (70%) in the GCA-Ao group, compared to 5 (42%) in the GCA-noAo group (p = 0.53). Among 7 deaths in the GCA-Ao group, 5 had a vascular origin, whereas no vascular causes of death were noted in the GCA-noAo group (p = 0.027). In the GCA-Ao group, causes of death were rupture of abdominal aortic aneurysm, dissection of thoracic aortic aneurysm, stroke, stage IV obliterating arteriopathy, coronary artery disease with congestive heart failure, sepsis related to urinary tract infection, and road accident (n = 1 each). Causes of death in the GCA-noAo group were bladder tumor, colon neoplasia, acute renal failure, pneumonia, and advanced dementia (n = 1 each). Survival curves are reported in Figure 1. Overall survival was similar in the 2 groups (Figure 1A), but vascular mortality (Figure 1B) was increased in patients with aortitis at diagnosis (p = 0.02, log-rank test).
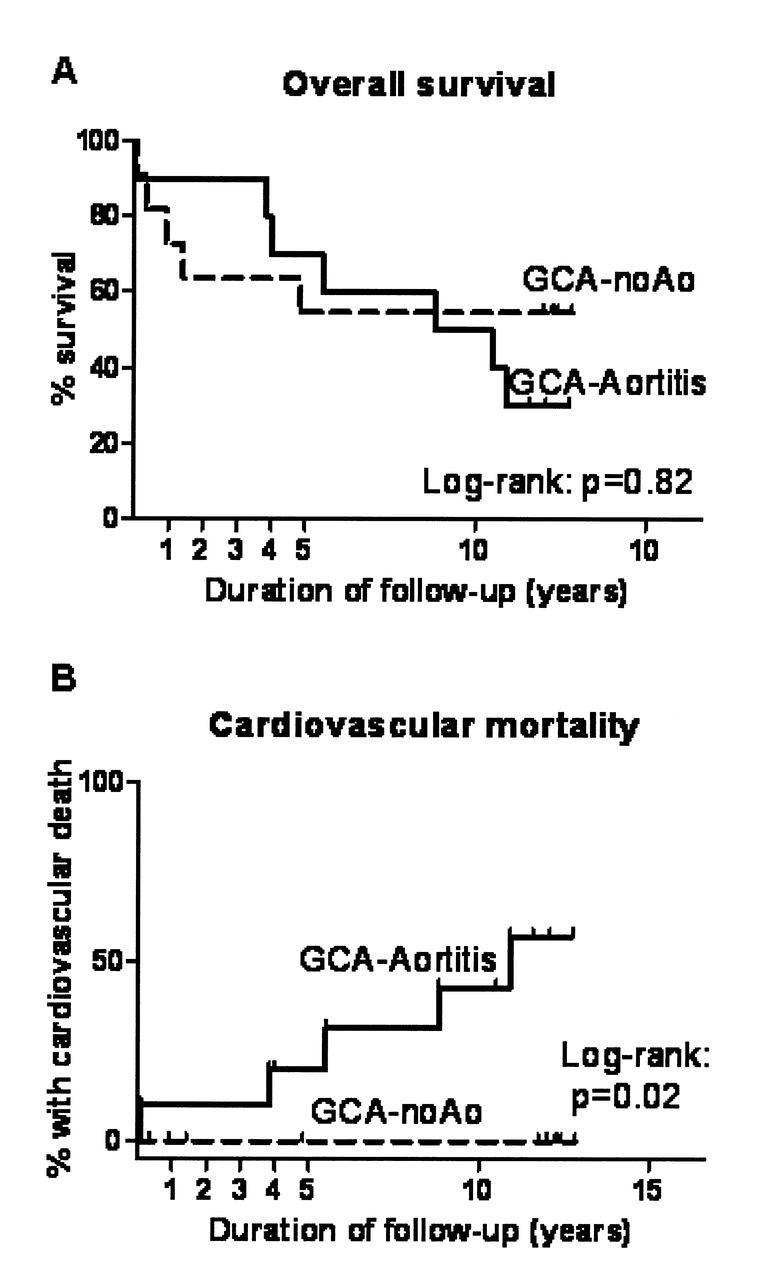
Cumulative probability of survival (A) or death of vascular origin (B) in giant cell arteritis (GCA) patients with aortitis (GCA-Aortitis) and without (GCA-noAo) at GCA onset. Hash marks indicate censored individuals.
At last followup, a higher rate of vascular events was found among patients with aortitis: 13 events had occurred in 7 patients in this group (mean number of vascular events per patient = 1.33), compared to 3 events in 5 patients without aortitis (mean 0.25 events per patient; p = 0.009). Details regarding types of vascular events are reported in Table 2.
Vascular outcome at last followup of patients with (GCA-Ao) and without aortitis (GCA-noAo) at GCA onset. Data represent number (percentage).
Stroke occurred more frequently in patients of the GCA-Ao group (4/10) than in patients with normal aorta at diagnosis (n = 0; p = 0.03). Proportion of patients with at least 1 vascular event tended to be higher among patients from the GCA-Ao group, but this difference was not statistically significant (p = 0.098; Figure 2).

Cumulative vascular events in giant cell arteritis (GCA) patients with aortitis (GCA-Aortitis) and without (GCA-noAo) at GCA onset. Hash marks indicate censored individuals.
Corticosteroid therapy and relapses of GCA
Every patient of this cohort was treated with steroids alone and none subsequently received immunosuppressive agents or steroid-sparing agents during the followup. The probability of definitive cessation of steroids was significantly lower in a patient with initial aortic involvement (p = 0.009, HR 0.16, 95% CI 0.04–0.6; Figure 3). Only 2/10 (20%) of these patients no longer took steroids at last followup, as compared to 8/12 (66%) in the other group (p = 0.04). Individuals’ progression of steroid dosages is depicted in Figure 4. Most patients of the GCA-noAo group had a more indolent course of vasculitis, with few patients requiring increasing steroid dosage. Conversely, patients from the GCA-Ao group frequently had increasing steroid requirements during their disease (Figure 4). At last visit, mean dosage of prednisone in the GCA-Ao group and the GCA-noAo group was 13.3 ± 20.45 mg and 8.75 ± 17.85 mg, respectively (p = 0.12).

Cumulative probability of definitive cessation of corticosteroid therapy (CS) in giant cell arteritis (GCA) patients with aortitis (GCA-Aortitis) and without (GCA-noAo) at GCA onset. Hash marks indicate censored individuals.

Progression of individual corticosteroid dose (prednisone equivalent) over time in patients with initial aortitis (GCA-Ao) or without (GCA-noAo).
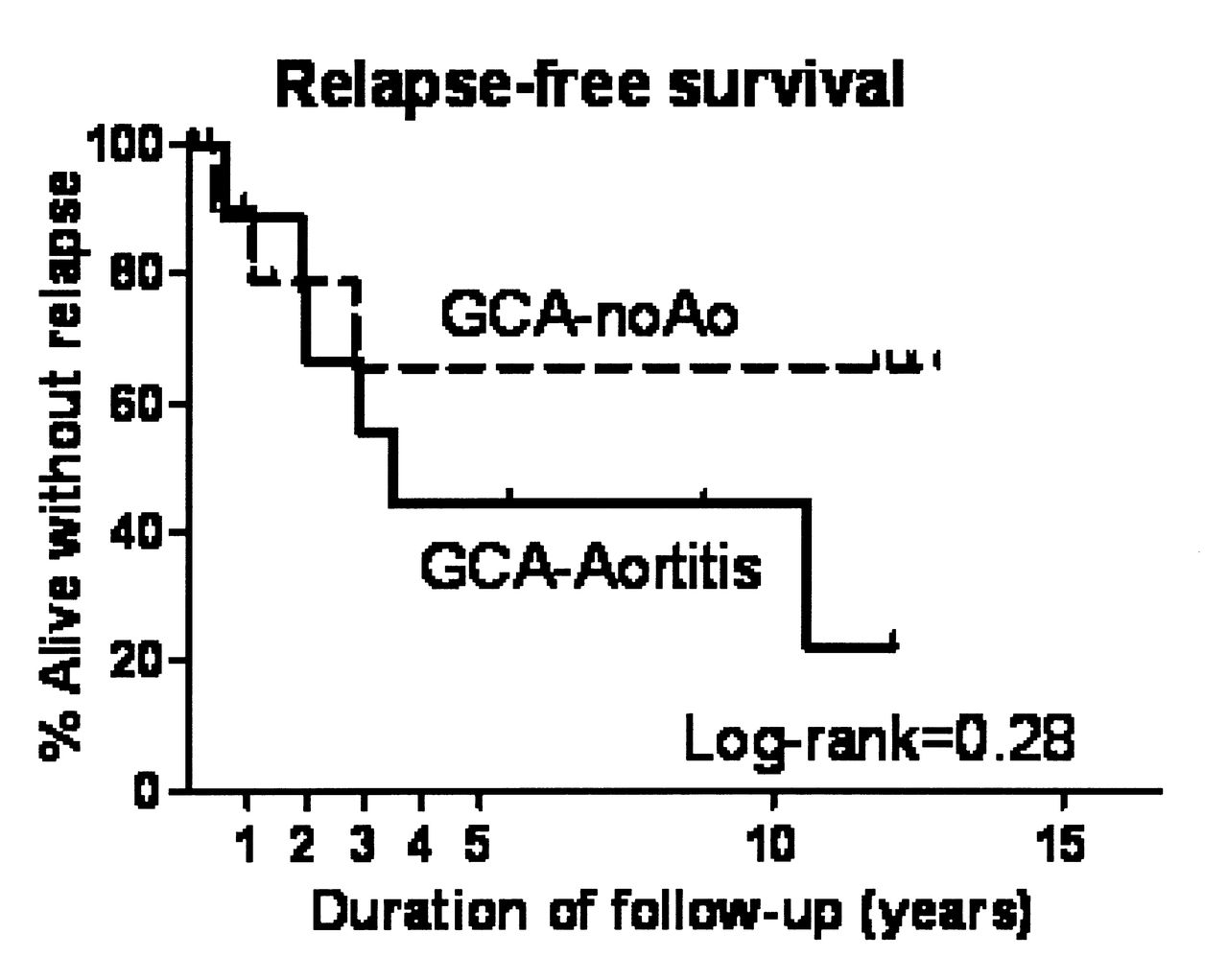
Relapses appeared to be more frequent in patients with aortitis: 6 of them (60%) had at least 1 relapse as compared to 3 (27%) in the other group (p = 0.14), and 5 (50%) had multiple relapses, whereas none of the patients without aortitis had multiple relapses (p = 0.012). In the GCA-Ao group, we recorded 16 relapses in 6 patients, compared to 3 in 3 patients in the other group. Mean numbers of relapses per patient were 1.6 in the GCA-Ao group and only 0.25 in the GCA-noAo group, and this difference was statistically significant (p = 0.037). Relapse-free survivals are compared in Figure 5. Longterm relapse-free survival was worse among patients with initial aortitis, but statistical analysis of cumulative relapse-free survival showed no significant differences (p = 0.28).
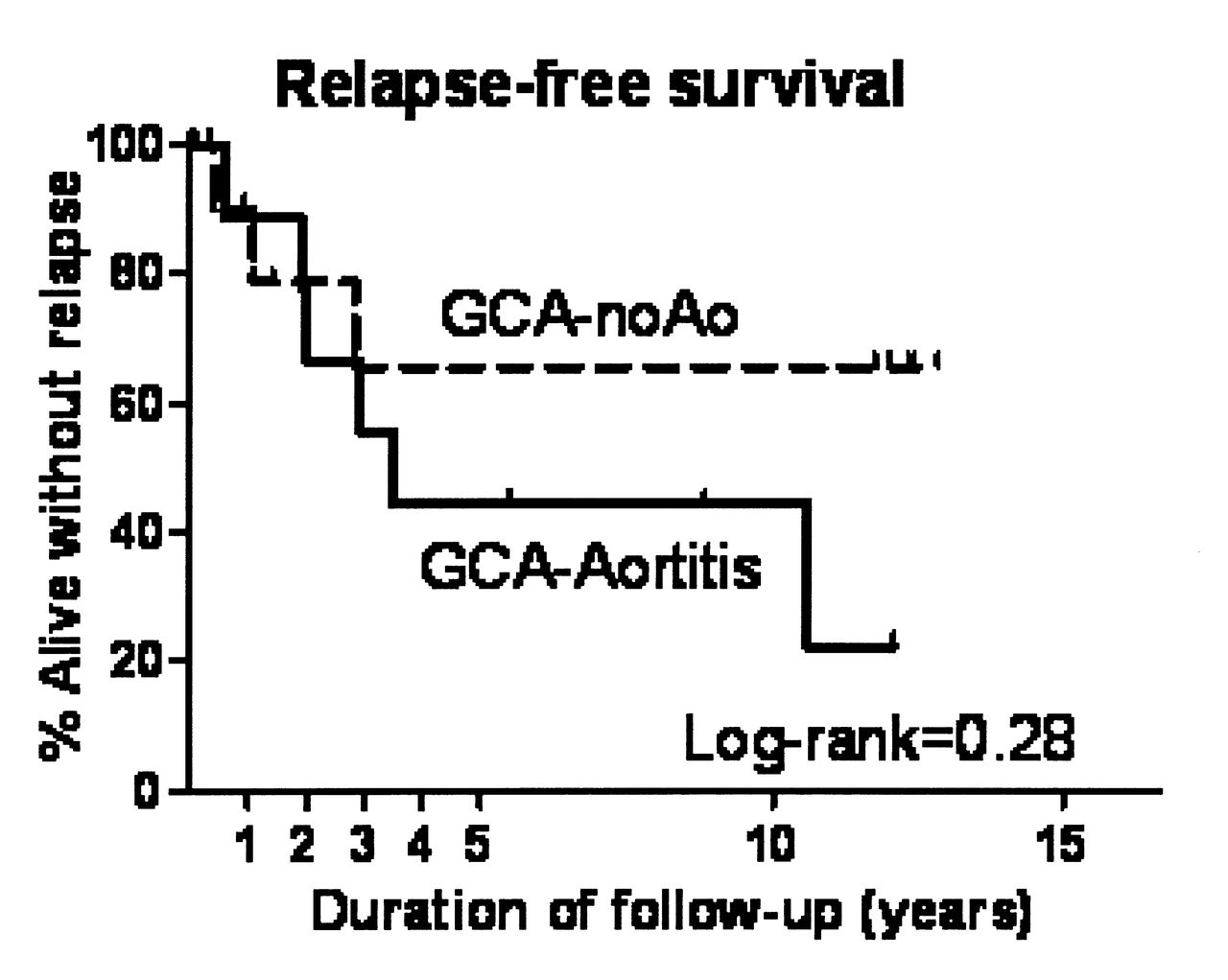
Cumulative relapse-free survival in giant cell arteritis (GCA) patients with aortitis (GCA-Aortitis) and without (GCA-noAo) at GCA onset. Hash marks indicate censored individuals.
DISCUSSION
We report the longterm outcome of 22 patients with GCA who had been investigated with aortic CT at diagnosis. To our knowledge, this study is the first to describe the longterm followup of patients with CT-defined aortic inflammatory involvement at the time of diagnosis of GCA. Indeed, only few large imaging studies have attempted to assess the prognostic significance of aortic involvement in GCA. Blockmans, et al performed an aortic CT scan in 46 patients who had undergone 18F-FDG PET at diagnosis of GCA, i.e., 46.7 ± 29.9 months before22. They found that FDG uptake in the aorta at onset correlated with the subsequent diameter of the aorta, especially at the level of the ascending aorta, which is the preferential site of aortic inflammatory involvement in GCA. However, correlations between onset aortic imaging results and the subsequent clinical course were not reported. Similarly, Garcia-Martinez, et al investigated 54 patients in a cross-sectional study using aortic CT after a mean followup of 5.4 years of previously diagnosed GCA3. They found that patients with aortic dilation (22%) more frequently had weak systemic inflammatory responses, and fewer GCA relapses3. These authors concluded that aneurysm formation does not mainly result from persistent detectable GCA activity. Our results point to a possible deleterious prognostic significance of initial aortic involvement in GCA. Indeed, patients with initial aortitis were more susceptible to relapses, and received more prolonged steroid treatment. In the long term, 80% of them had to resume or could not withdraw from use of corticosteroids. To our knowledge, the correlation between aortic involvement and steroid dependence has never been demonstrated, although it was suspected by many authors10,12,23,24. Marie, et al reported a cohort of 48 with GCA-related aortitis where only 35% of patients were treatment-free at last followup. However, median followup was only 12 months in that study10. In the very long term, we found that in patients with aortitis at diagnosis, GCA frequently exhibited a chronic and relapsing course, whereas patients with normal aorta tended to have indolent, single-course, relapse-free, and curable GCA. Moreover, in our small but well-described cohort, fatal and nonfatal vascular events were more frequent in patients with signs of aortic involvement on the initial CT scan.
In our cohort, a total of 4/22 (18%) patients developed an aortic symptomatic complication. This finding is in accord with results of studies that estimated a longterm incidence of aortic complications of 9.5%–17.9%2,8,9. Among these 4 patients, 3 had initial aortic involvement, as compared to 1/12 in the other group. Interestingly, the latter patient had a “halo sign” suggestive of aortitis on an abdominal aortic duplex sonography scan performed at disease onset. Hence, this discrepancy may be due to a lower sensitivity of CT scanning, which led to misclassification of this case. That is why duplex sonography and 18F-FDG PET could also be useful for the diagnosis of asymptomatic aortic involvement in GCA25,26.
We found that patients with aortic involvement suffered more vascular events during followup. However, we are aware that the reduced number of patients (10 vs 12 and 7 vs 5 for vascular mortality) in our study does not allow definitive conclusions regardless of the p values. Importantly, cardiovascular risk factors were not more prevalent in patients with initial aortitis as compared to others. Whether the increased number of vascular events in these patients can be related to vasculitic involvement of large vessels remains undetermined. This might be the case for some patients, because stroke or obliterating arteriopathy are rare but well-described clinical features in GCA. In our series, 4 patients with initial aortitis subsequently developed stroke in the followup. Coexistence of aortitis and stroke is not so common in GCA but has been reported, including in 2 cases at the very beginning of GCA4. In a recent retrospective study, Assie, et al pointed out that aortic involvement was a frequent finding in GCA patients with symptomatic upper/lower extremity artery involvement27. However, the latter is not systematically associated with a higher prevalence of vascular events28. Indeed, all patients with GCA appear to be at increased risk of cardiovascular disease2,29,30. Given that our patients with initial aortitis seemed to exhibit a more chronic disease course, this increase in vascular events may also result from accelerated atherosclerosis due to chronic systemic inflammation and/or prolonged corticosteroid therapy.
Our results prompt us to ask whether patients with CT signs of aortitis at onset of GCA would benefit from a more aggressive therapeutic approach, using immunosuppressants, for example. In our opinion, this question deserves consideration. A metaanalysis found that methotrexate could be an interesting option in GCA, but most controlled trials have failed to identify an effective steroid-sparing agent1,31,32,33,34. This may be because GCA exhibits a favorable course under steroid therapy in most cases35. It is possible that a subset of patients would benefit from more aggressive therapy, to prevent longterm vascular morbidity and mortality. In our experience and that of others14,15, CT scanning may suggest aortic involvement (aortic thickening, aneurysm, ectasia) in 45%–65% of patients with newly diagnosed GCA. Our data remain to be confirmed but our findings suggest that this involvement could predict a more aggressive form of GCA. Therefore, CT scanning may be an appropriate tool to identify patients to be enrolled in future therapeutic trials. We hypothesize that aortic imaging at onset will influence our therapeutic approach to GCA in the future. Until then, physicians should control cardiovascular risk factors, but also monitor screening of aortic involvement in GCA.
Our study has limitations such as its small size and the retrospective design. The small size leads us to be cautious about any conclusions. Moreover, there was no proof of the vasculitic nature of the different vascular events we observed, especially for the 5 patients who had aortitis at diagnosis and who died from vascular complications. The retrospective design probably prevented us from obtaining complete detailed information regarding disease course (relapses and steroid dosages) and steroid side effects. This is mainly due to the relatively long period we investigated. However, no living patient was lost to followup, each patient had regular medical examinations, and data were sufficiently complete in our opinion. Indeed, our long followup is a strong feature of the study, as is the standardized imaging of patients performed at GCA onset.
We describe for the first time the longterm outcome of a cohort of 22 patients with aortic CT evaluation at diagnosis of GCA. Despite some limitations, our study suggests that GCA-related aortitis is a particular disease subset that could exhibit a more chronic course and increased longterm vascular morbidity and mortality. Further studies are needed to confirm our findings and clarify their therapeutic implications.
- Accepted for publication July 31, 2012.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}