

Abstract
Objective. Antinuclear antibodies (ANA) are a serological hallmark of systemic autoimmune rheumatic diseases (SARD) such as systemic lupus erythematosus (SLE). While a number of ANA patterns detected by indirect immunofluorescence (IIF) have diagnostic significance, autoantibodies producing the dense fine speckled (DFS) pattern have been reported to be more prevalent in healthy individuals than in SARD.
Methods. Sequential samples submitted for ANA testing were screened for anti-DFS antibodies by IIF (n = 3263). Samples with the DFS pattern were tested for anti-DFS70/lens epithelium–derived growth factor (LEDGF) antibodies by ELISA and by a novel chemiluminescence assay (CIA, Quanta Flash DFS70). Sera from patients with various diseases and healthy individuals were tested for anti-DFS70/LEDGF antibodies by CIA. A cohort of 251 patients with SLE was used to analyze serological and clinical associations of anti-DFS70 antibodies.
Results. The frequency of anti-DFS antibodies by IIF was 1.62%. The prevalence of anti-DFS70/LEDGF antibodies as detected by CIA in the different cohorts was 8.9% in healthy individuals, 2.8% in SLE, 2.6% in rheumatoid arthritis, 4.0% in asthma, 5.0% in interstitial cystitis, 1.7% in Graves’ disease, and 6.0% in Hashimoto’s thyroiditis. Of note, the prevalence of anti-DFS70/LEDGF antibodies was significantly higher in healthy individuals compared to patients with SARD (p = 0.00085). In SLE results, anti-DFS70/LEDGF antibodies were not significantly associated with clinical features or other autoantibodies typically found in SLE. Only 1/7 SLE sera showed anti-DFS70/LEDGF, but no other autoantibody reactivity.
Conclusion. “Monospecific” anti-DFS70/LEDGF antibodies may represent a biomarker for differentiating SARD from non-SARD individuals, but there is a need for a reliable assay to ensure reactivity to DFS70.
- ANTINUCLEAR ANTIBODIES
- DENSE FINE SPECKLES ANTIBODIES
- LENS EPITHELIUM–DERIVED GROWTH FACTOR
- AUTOANTIBODIES
- SYSTEMIC LUPUS ERYTHEMATOSUS
- AUTOIMMUNE DISEASE
The presence of autoantibodies, including antinuclear antibodies (ANA), directed against intracellular antigens is a hallmark of systemic autoimmune rheumatic diseases (SARD)1. The indirect immunofluorescence (IIF) assay is one of the most commonly used routine tests for detection of ANA, and it was recently recommended as the screening test of choice by a study group of the American College of Rheumatology (ACR)2. Anti-dense fine speckled 70 (anti-DFS70) antibodies were initially identified as an ANA IIF pattern from a patient with interstitial cystitis3, but they were later associated with various other conditions4.
The typical DFS IIF staining pattern is recognized as uniformly distributed fine speckles throughout the interphase nucleus and on metaphase chromatin3,4,5. Since a 70-kDa protein was detected by immunoblotting, the antigen was initially termed DFS70, but the primary target autoantigen was eventually identified as the lens epithelium–derived growth factor (LEDGF)6 or DNA-binding transcription coactivator p75 (reviewed by Ganapathy and Casiano4). This protein was highly expressed in prostate tumor tissues7 and has a number of physiological functions, including serving as a cofactor for human immunodeficiency virus replication through an interaction with viral integrase8.
Since the first description, anti-DFS70/LEDGF antibodies have been reported in the sera of patients with a variety of chronic inflammatory conditions (as reviewed4), in patients with cancer7, and even in certain healthy individuals9. Dellavance, et al evaluated over 10,000 ANA-positive samples by IIF and immunoblot; they reported that anti-DFS70 antibodies were common among ANA-positive individuals with no evidence of SARD and that among autoimmune patients bearing this autoantibody, over half had evidence of autoimmune thyroiditis10. The highest prevalence of anti-DFS70 antibodies has been reported in patients with Vogt-Harada syndrome (66.7%)11 and atopic dermatitis (30%)3,12, followed by apparently healthy individuals (∼10%)4,9, while prevalence in SARD is significantly lower (∼2%−3%)4. Considering the prognostic and longterm outcome of individuals with anti-DFS70 antibodies, it was recently reported that none of 40 healthy individuals with isolated anti-DFS70 reactivity developed a SARD within an average 4-year followup13. Therefore, it was suggested that the presence of isolated anti-DFS70 antibodies could be taken as strong evidence against a diagnosis of SARD such as systemic lupus erythematosus (SLE)9,13,14,15.
The low prevalence of anti-DFS70/LEDGF autoantibodies in patients with SARD represents a potentially important biomarker to discriminate SARD from ANA-positive healthy individuals and/or other inflammatory conditions such as atopic dermatitis. The reasons underlying the observed relatively low prevalence in SARD are unclear, but may include demographic and racial (genetic) factor16, influence of therapeutic interventions (i.e., corticosteroids, immune suppression), and/or technologies used to detect the autoantibody.
Because ANA and related autoantibodies are generally considered reliable biomarkers for SARD and are included in the classification criteria for SLE17, ANA testing on HEp-2 substrates outside a proper clinical framework may yield a sizable portion of ANA-positive individuals without consistent evidence of SARD, purportedly leading to inappropriate referrals to tertiary care specialists, anxiety in patients and physicians13, and inappropriate and potentially toxic therapies18. Understanding the clinical relevance of the full spectrum of autoantibodies detected in a diagnostic laboratory becomes even more crucial because of compelling evidence that autoantibodies may precede the clinical onset of SARD by many years19,20,21. Therefore, the concept of using anti-DFS70 antibodies as a diagnostic or prognostic discriminator of subjects with and without SARD is appealing. Accordingly, the principal aims of our study were to determine the frequency of anti-DFS70 antibodies in a diagnostic laboratory setting and then investigate the prevalence of anti-DFS70 antibodies in various disease conditions, especially in patients with SLE and in healthy individuals, using conventional IIF complemented by novel immunoassays for the detection of anti-DFS70 antibodies.
MATERIALS AND METHODS
DFS antibodies in sequential samples submitted for ANA testing
Sera samples (n = 53) with a DFS staining pattern were identified by IIF on HEp-2 cell substrates from 3263 sequential samples submitted for ANA testing (BC Biomedical Laboratories Ltd. during a 44-day audit period using the protocol described below.
Clinically defined samples
A second cohort included clinically defined samples from healthy individuals (n = 124; 86 women and 38 men), all with no known history of SARD, obtained from a commercial source (ProMedDx) and various pathologies (SLE, rheumatoid arthritis, asthma, atopic dermatitis, interstitial cystitis, systemic sclerosis, Graves’ disease, Hashimoto’s thyroiditis, multiple sclerosis, inflammatory bowel disease, cancer, Sjögren’s syndrome, infectious diseases, and other disorders). The average age of healthy individuals was 37 years (SD 13.1 yrs, range 17−60 yrs). The diagnosis of SARD was established according to criteria for the respective disease and as described22. The disease activity was defined based on the SLE Disease Activity Index (SLEDAI) using a cutoff value of 6. The international ANA reference serum panel available from the Centers for Disease Control and Prevention (CDC, Atlanta, GA, USA) was also tested for anti-DFS70 antibodies by Quanta Flash DFS7023. Patient identity was not disclosed and the data were used anonymously in accord with the Helsinki Declaration on human research ethics. Collection of patient samples was carried out according to local ethics committee regulations and, where required, approval was obtained from the respective institutional review board.
Immunofluorescence assays
The DFS samples were identified at BC Biomedical Laboratories Ltd. using the HEp-2010/Liver (Monkey) IIF kit (Euroimmun; catalog no. FA 1512-2010-1). Sera were screened at 1:80 dilution on slides prepared with a PhD instrument (Biorad). Reading and interpretation of the IIF patterns were done by an experienced technologist on a Zeiss microscope fitted with an LED light source.
ELISA and chemiluminescence anti-DFS70/LEDGF assays
Anti-DFS70 reactivity detected by IIF was confirmed by ELISA (MBL International) and by Quanta Flash DFS70 (Inova) testing. The semiquantitative MBL DFS70 ELISA Kit is used for detection of anti-DFS70 antibodies in human serum. The ELISA antigen is identical to LEDGF and the DFS70 ELISA is currently intended for research use only.
The Quanta Flash DFS70 assay is a novel chemiluminescence assay (CIA; research use only) that uses recombinant DFS70/LEDGF coated onto paramagnetic beads and is designed for the Bio-Flash® instrument (Biokit SA). The principle and protocol of the assay system have been described24. The relative light units (RLU) are proportional to the amount of isoluminol conjugate that is bound to the human immunoglobulin (Ig)G, which in turn is proportional to the number of anti-DFS70 antibodies bound to the antigen on the beads. The cutoff of the novel DFS70 CIA was established based on the comparison with the MBL DFS70 ELISA. The threshold was set to yield the highest degree of total percentage agreement.
Recombinant DFS70/LEDGF antigen and Western blotting
Human recombinant DFS70/LEDGF antigen was generated as described25 and expressed as a polyhistidine (his)-tagged protein in insect cells (SF9 cells; Invitrogen) or e.coli (both antigens equivalent) according to the manufacturer’s instructions. Purification of the his-tagged DFS70/LEDGF antigen was accomplished using conventional affinity chromatography on nickel columns. Purity of the antigen was determined to be > 95% by gel electrophoresis. Sera positive for anti-DFS70 antibodies or displaying the DFS IIF patterns were also analyzed by Western blotting, using a partial-length recombinant DFS70/LEDGF protein (amino acids 349−435) that was separated by 4%−12% Bis-Tris gel electrophoresis and transferred to nitrocellulose sheets using an Invitrogen iBlot system. The assay protocol followed standard procedures and was similar to the method as described13.
Affinity purification of anti-DFS70 antibodies from human serum
For affinity purification 0.5 ml of rehydrated resin was equilibrated in 0.1 M NaHCO3, 0.5 M NaCl, pH 8.3. Then 1.5 ml of DFS70 antigen (1.9 mg/ml) was added to the resin and incubated at 4°C overnight. The next day, the resin was washed with 0.1 M NaHCO3, 0.5 M NaCl, pH 8.3, and blocked with 1 M ethanolamine, pH 8.0 for 2 h at room temperature. Finally, the resin was washed with 5 cycles of alternating pH (0.1 M sodium acetate, 0.5 M NaCl, pH 4.0, and 0.1 M Tris-HCl, 0.5 M NaCl, pH 8.0).
Equilibrated, the column was loaded with a total 10 ml of filtered serum containing anti-DFS70 antibodies. After washing with 10 mM Tris-HCl, 0.5 M NaCl, 0.09% sodium azide, antibodies were eluted using 0.1 M glycine-HCl, pH 2.8. The eluted fractions were neutralized using a 1:10 ratio of 1 M Tris, 2.5 M NaCl, 0.9% sodium azide, pH 8.8. Purified antibodies were diluted 1:3 into a negative IgG-stripped serum pool resulting in a final volume of 4.5 ml.
Detection of other autoantibodies
Antibodies to dsDNA, chromatin, SSA (Ro52 and Ro60), SSB/La, ribosome P, C1q, RNP, and Sm were detected by the corresponding Quanta Lite ELISA. In addition, C1q complexes were measured (Quanta Lite ELISA). All assays were performed according to the manufacturer’s instructions (all Inova).
Statistical evaluation
Data were statistically evaluated using Analyse-it software (version 2.03; Analyse-it Software Ltd.). Mann-Whitney U-test and Fisher’s exact test were carried out to analyze difference between groups, and p values < 0.05 were considered significant. Spearman equations were used to analyze agreement between the CIA and ELISA.
RESULTS
Anti-DFS antibodies in sequential samples submitted for ANA testing
Using IIF on HEp-2 substrate, 53/3263 (1.62%) sequential and unselected serum samples submitted for routine ANA testing were identified as showing the typical DFS staining pattern and were then confirmed to be positive for anti-DFS70 antibodies by ELISA and CIA. Of the 53 samples, 40 were from women and 13 from men; the mean age of women was 47.5 years (± 15.5 yrs, range 14−80) and thus not significantly different from the age of men (45.3 ± 11.9 yrs, range 25−63). No association between the anti-DFS70 reactivity and the age of individuals was observed. Of our 53 samples with a DFS pattern, 52/53 were positive for anti-DFS70 antibodies by CIA and 53/53 by ELISA. A quantitative comparison between the DFS70 ELISA (MBL) and CIA (Inova) showed an excellent quantitative correlation between the 2 methods as expressed by a Spearman correlation coefficient r = 0.91 (95% CI 0.84−0.95, p < 0.0001; Figure 1).

Quantitative correlation between dense fine speckled antibodies (DFS70) ELISA and Quanta Flash DFS70. The results of 53 sera were used to analyze the quantitative agreement between the 2 methods and an excellent correlation was found (r = 0.91, p < 0.0001, Spearman equation). Results obtained by Quanta Flash DFS70 are expressed as relative light units (RLU).
Point prevalence of anti-DFS70/LEDGF antibodies in apparently healthy individuals and various disease groups
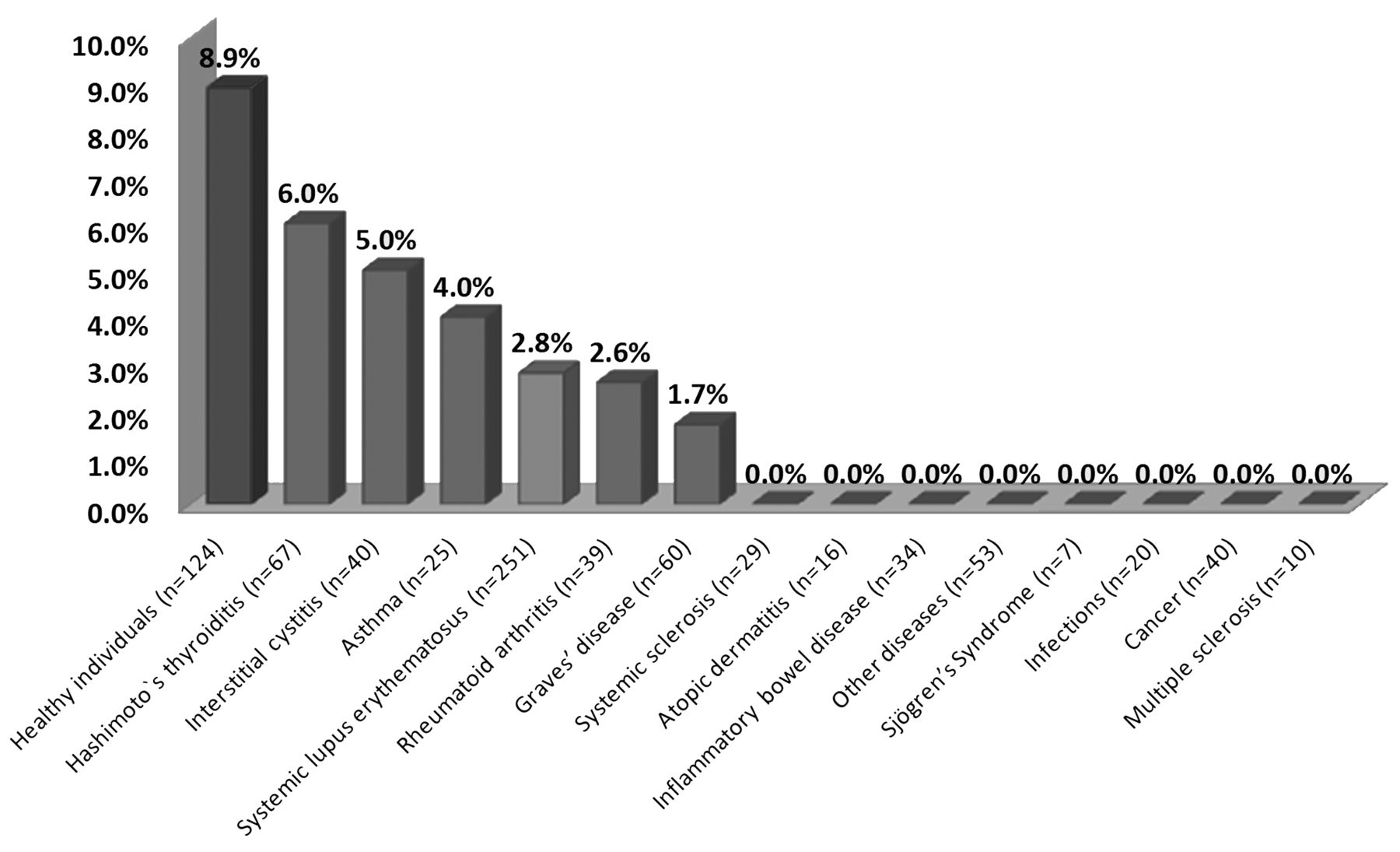
To verify that anti-DFS70 antibodies are not associated with SARD or certain manifestations, we investigated a possible association with clinical features in SLE. Anti-DFS70/LEDGF antibodies were detected in 11/124 (8.9%) of sera samples from healthy individuals. The prevalence in the disease cohorts varied between 0.0% and 6.0% (Figure 2). Of note, the prevalence of anti-DFS70 antibodies was significantly higher in healthy individuals (8.9%) compared to patients with SARD (2.8%; p < 0.001, Fisher’s exact test). The OR was 3.7 (95% CI 1.5−8.9). To confirm the low prevalence of anti-DFS70 antibodies in characteristic samples from patients with SARD, we also tested the CDC ANA reference samples by Quanta Flash and all were negative.
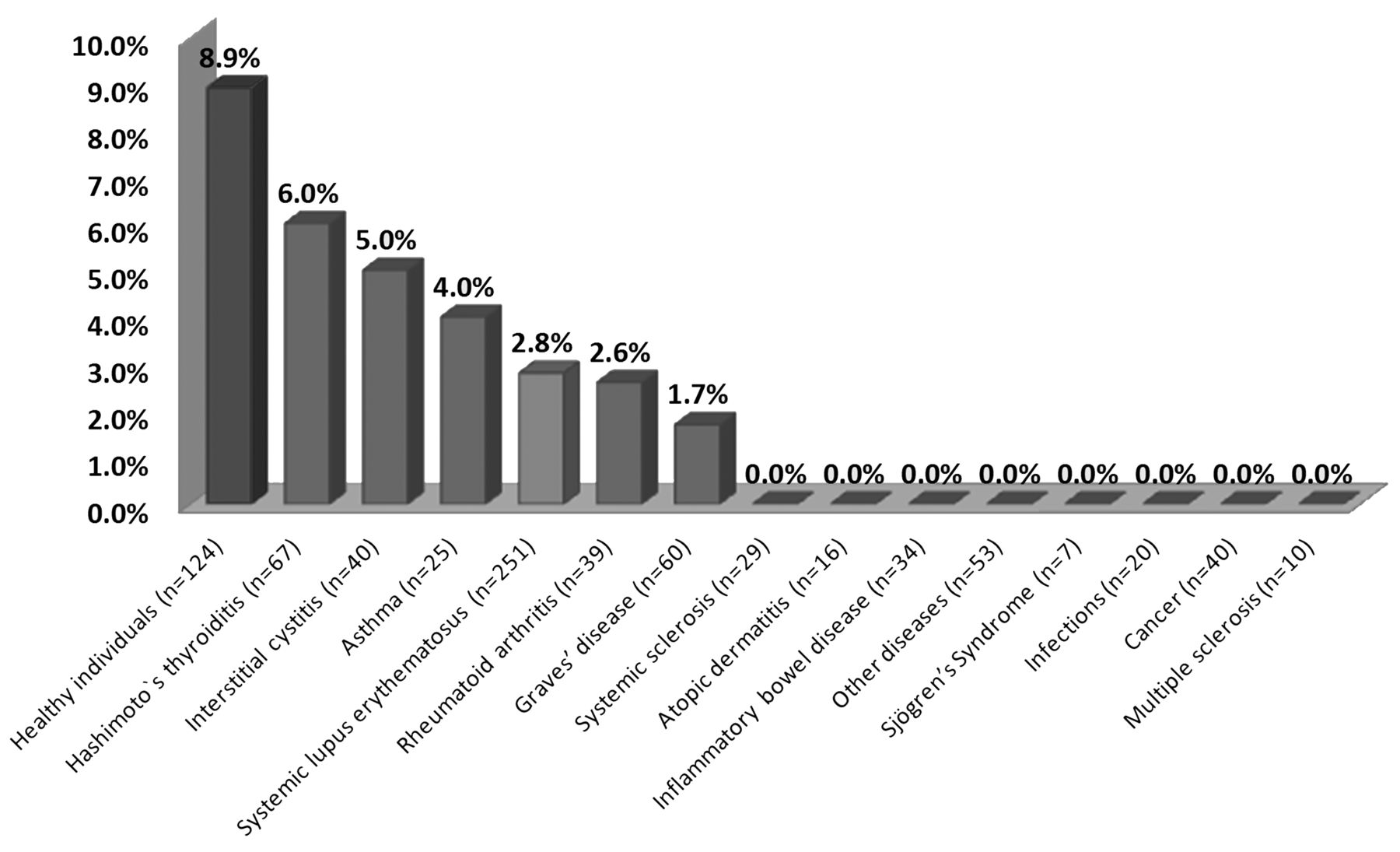
Prevalence of anti-dense fine speckled (DFS)70 antibodies in different cohorts determined by chemiluminescence immunoassay. The prevalence of anti-DFS70 antibodies found in apparently healthy individuals and in different pathologies is given in percentages. The prevalence in apparently healthy individuals was significantly higher than in all other diseases including systemic lupus erythematosus.
Association of anti-DFS70/LEDGF and other autoantibodies in a large SLE cohort
Seven of 251 samples (2.8%) from patients with SLE were positive for anti-DFS70 antibodies by CIA, of which 1 was also positive for anti-Sm, 2 for anti-dsDNA, 3 for anti-U1RNP, 3 for anti-SSB/La, 3 for anti-C1q, 4 for anti-chromatin, and 4 for anti-SSA (Ro60/Ro52 mixture). None of the samples was positive for anti-ribosome P. Only 1 of the SLE serum samples had isolated anti-DFS70 reactivity. No statistically relevant clinical or laboratory differences were found between anti-DFS70-positive and -negative patients with SLE (Table 1). Of the 11 ACR classification criteria for SLE17, 2 anti-DFS70-positive patients fulfilled 4, 2 patients 5, 1 patient 6, and 2 patients 8. The patient with isolated anti-DFS70 antibodies fulfilled 5 criteria irrespective of the positive DFS ANA (Table 2). The mean age (43.0 vs 48.1 yrs), the disease duration (6.4 vs 8.3 yrs), and the female/male ratio of the anti-DFS70-positive patients with SLE were not significantly different from those of the anti-DFS70-negative patients. The most common clinical feature of the anti-DFS70-positive patients with SLE was arthritis (n = 7, 100%) followed by photosensitivity (n = 5, 71.4%). Although it did not reach statistical significance (p = 0.064), a remarkable difference between anti-DFS70-positive and -negative patients was the presence of hemolytic anemia, which was higher in the anti-DFS70-positive group. The average SLEDAI score (4.0 vs 3.7, respectively) and the number of active patients (SLEDAI > 6; 18.9% vs 14.3%) was higher in anti-DFS70-nega tive compared to anti-DFS70-positive patients, but the differences were not statistically significant. These results are summarized in Table 1.
Associations of anti-DFS70/LEDGF with clinical features and other autoantibodies in SLE. Data are number (%).
Clinical and serological features of anti-DFS70-positive patients with SLE.
IIF patterns and immunoblot reactivity of anti-DFS70/LEDGF-positive samples
Ten of the 11 (90.9%) anti-DFS70/LEDGF-positive samples (by DFS70 CIA) from healthy individuals (n = 124) showed the typical DFS staining pattern by IIF on HEp-2 cells. The only sample (1/11) that did not demonstrate the typical DFS pattern lacked the typical staining of metaphase chromatin. In contrast, the IIF pattern of 6/7 SLE was different from the typical DFS staining pattern previously described (Figure 3B). All anti-DFS70 antibody-positive samples identified by CIA were also positive by immunoblot using the recombinant protein (data not shown).

Affinity purification of anti-dense fine speckled (DFS)70 antibodies from human serum. Anti-DFS70 antibodies were affinity-purified from human serum using recombinant DFS70 immobilized on a Sepharose column. Eluted fractions were characterized using the DFS70 chemiluminescence assay and 4 reactive fractions were pooled (panel a.). Indirect immunofluorescence results using the affinity-purified antibodies show typical staining pattern of anti-DFS70 antibodies (panels b. to d.). RLU: relative light units.
To compare the staining pattern of anti-DFS70/LEDGF antibody-positive samples, a prototype serum was tested on slides from 4 different manufacturers (Euroimmun, Inova, The Binding Site, Kallestad/Bio-Rad). Although minor differences were observed in the degree of discrete speckles in interphase nuclei, the DFS IIF pattern on interphase nuclei accompanied by staining of metaphase chromatin was similar on slides from all manufacturers.
DISCUSSION
Although anti-DFS antibodies have been historically associated with interstitial cystitis3 and atopic dermatitis5,12, they have also been described in various other diseases4. Although a distinctive clinical association is unreported, anti-DFS70 antibodies have been proposed as a useful biomarker for the exclusion of SARD9,14,15. This suggestion has mainly been based on the observation that anti-DFS antibodies are more prevalent in healthy individuals than in patients with SARD and that anti-DFS-positive individuals did not develop SARD after clinical followup of 4 years13. Anti-DFS70 antibodies have been reported in about 3% of patients with SLE14, but usually accompanied by other SLE-associated antibodies such as anti-dsDNA, anti-SSA/ Ro, or anti-Sm. We confirmed the reported prevalence of anti-DFS70 antibodies in healthy individuals and patients with SLE and in particular noted the low prevalence of isolated anti-DFS70 reactivity in SARD14.
In one early study, Daniels, et al reported that 46 of 206 (22.3%) sera samples from patients with prostate cancer had anti-DFS70 reactivity by ELISA or immunoblot7. Later, anti-DFS70 reactivity was found in only 6/334 cancer patients (1.8%)27 as determined by IIF (details about the cell substrate were not provided). The authors concluded that the low prevalence of anti-DFS70 antibodies might be attributed to the limited sensitivity of IIF for the identification of anti-DFS70-positive samples. In our study, all patients with colon (n = 20) and breast cancer (n = 20) were negative for anti-DFS70 antibodies when tested by CIA.
Because previous studies did not include samples from patients with inflammatory bowel disease (IBD), multiple sclerosis, and individuals with infectious diseases; we included those cohorts in our study. Interestingly, the prevalence of anti-DFS70 was significantly higher in healthy individuals than in patients with IBD or in individuals with infectious diseases. The higher prevalence of anti-DFS70 antibodies in healthy individuals compared to patients with SARD might support the hypothesis that these autoantibodies serve a protective function28. Further longitudinal studies are required to address this.
One study has thoroughly analyzed the epitope distribution on DFS70/LEDGF using recombinant protein fragments and synthetic peptides spanning the entire DFS70/LEDGF sequence; it was found that the major reactivity is restricted to a presumably conformational epitope localized to the C-terminal alpha-helical domain25. However, no difference between patients with SARD and healthy individuals in the recognition of the various epitopes was observed25.
Association with other autoantibodies
Thirty-three percent to 50% of ANA-positive sera derived from healthy individuals have been reported to demonstrate anti-DFS70 antibodies13,25. The prevalence in patients with SARD is significantly lower. In the SLE group studied by Muro, et al14, 4/7 anti-DFS70-positive patients with SLE were positive for anti-SSA/Ro antibodies, 6/7 were also positive for dsDNA, and 2/7 for anti-Sm. In our SLE cohort the coexistence of other autoantibodies was similar: 2/7 anti-DFS70-positive patients with SLE were positive for anti-dsDNA and 1 for anti-Sm antibodies. Only 1/7 SLE patients with anti-DFS70/LEDGF antibodies had no additional autoantibodies (Table 2). These data confirm that anti-DFS70/LEDGF antibodies in SARD are rarely observed, and when they are, they are usually accompanied by additional SARD-related autoantibodies.
Association between anti-DFS70/LEDGF antibodies and demographic and clinical features
The prevalence of anti-DFS70/LEDGF positivity has been reported to decrease with increasing age9,13, a finding that we did not confirm in our present study. This might be explained by the difference in the composition of the 2 cohorts of healthy individuals. Because SARD are more prevalent in females than in males1,29, autoantibodies to nuclear antigens are consequently also more prevalent in females1,29,30. In the study published by Watanabe9, et al, 55/453 females (12.1%) had anti-DFS70 antibodies compared to 9/144 males (6.3%; not significant, p = 0.06). However, in our study anti-DFS70 antibodies were not significantly more prevalent in female healthy individuals.
In our SLE cohort, there were no obvious clinical differences between anti-DFS70 antibody-positive and anti-DFS70 antibody-negative patients (Table 2). However, additional clinical-serologic studies in large cohorts of patients with well characterized SLE are required to determine whether the presence of the antibody is associated with demographic factors or specific clinical phenotypes such as particular organ involvement, disease activity, cumulative damage, or the effect of therapeutic interventions.
Importance of anti-DFS70/LEDGF antibodies in routine ANA testing
One study reported that 172/21,512 samples (0.8%) showed the typical DFS pattern by IIF27, while another investigation showed that anti-DFS antibodies were present in only 12.3% of consecutive samples tested for ANA10. In our investigation, 1.62% of samples had a DFS pattern. Virtually all were then confirmed by CIA and/or ELISA. In addition to methodological variability that may reflect differences in interlaboratory variation of techniques, referral patterns or other demographic variables such as ethnicity may be involved. Nevertheless, it is important to note that the frequency of anti-DFS70 antibodies is within the range of other important SARD autoantibodies such as anti-dsDNA antibodies31,32. Because significant differences have been described between the staining patterns on HEp-2 cells from different manufacturers31,33, we used a prototype serum derived from an apparently healthy individual on slides from 4 different manufacturers. Although the DFS pattern was slightly different, the differences were less pronounced than for other autoantibodies such as anti-ribosome P31. Such minor variation might be attributed to the fixation method used for manufacturing the cell substrates. Although our data indicate that the DFS pattern can be identified on slides from a number of ANA kit manufacturers, more samples need to be analyzed to draw a conclusion, especially because controversial results have been published33.
Because a positive ANA test result is an important component in the triage and diagnosis of patients with possible SARD, ANA–HEp-2 testing outside a proper clinical framework may yield a sizable portion of ANA-positive apparently healthy individuals, causing concern and anxiety in patients and physicians13. This result also may lead to prescribing inappropriate and potentially toxic therapeutics18. This becomes more crucial with the perception that autoantibodies may precede the clinical onset of SARD by many years19,20,21. Hence, samples with DFS staining pattern identified by IIF should be tested for anti-DFS70/LEDGF antibodies by a specific assay (i.e., ELISA or CIA) and the result should be included in the laboratory report. Clinicians should not overestimate positive ANA results in patients with isolated anti-DFS70/LEDGF antibodies and focus on the patients’ clinical symptoms, complemented by the detection of other disease-specific autoantibodies.
Our data confirm previous observations that anti-DFS70 antibodies are significantly more prevalent in healthy individuals compared to patients with SARD and other conditions. Therefore, anti-DFS70 antibodies represent a promising diagnostic biomarker, because in isolation (without any other SARD-associated autoantibodies) it is associated with a decreased likelihood of SARD in individuals with a positive DFS ANA compared with other patterns.
Acknowledgment
We thank Andrea Seaman, Wilson Yang, Kristen Buckmelter, Chelsea Bentow, Sima Patel, Jason Wu, Aaron Lanes (Inova Diagnostics), Meifeng Zhang, and Haiyan Hou (both University of Calgary) for technical assistance and Cassandra Bryant (Inova Diagnostics) for performing indirect immunofluorescence.
Footnotes
-
M. Mahler, C.L. Peebles, and T. Parker are employees of Inova Diagnostics Inc. M.J. Fritzler is a paid consultant of Inova Diagnostics Inc. and ImmunoConcepts and is the director of Mitogen Advanced Diagnostics Laboratory.
- Accepted for publication July 3, 2012.








{kind=link}
{kind=link}
{kind=link}