

To the Editor:
Rheumatoid arthritis (RA) is a chronic disease of unspecified etiology that is manifested by persistent inflammation of the synovium. Proinflammatory cytokines such as tumor necrosis factor (TNF), interleukin 6 (IL-6), and B cells are involved in the pathogenesis and chronicity of the inflammatory process in RA, and lead to development of antagonists to treat the disease1.
Although the use of anticytokine and B cell therapy benefits a substantial number of patients, in some these therapies tend to lose response after the initial benefit2. We describe a patient for whom all available biologic therapies, with different mechanisms of action, failed to inhibit progress of the disease throughout a decade. The patient underwent several orthopedic procedures in small and large joints during that period.
Symptoms in our patient started in 1998, when she was 35 years old. She was positive for rheumatoid factor. When anticyclic citrullinated peptide measures became available, she had titers above 200 U on several occasions. In 2002, after she underwent a partial synovectomy of the wrist, she was started on 2 anti-TNF inhibitors sequentially, followed by rituximab, abatacept, and lastly tocilizumab, in 2009. A series of surgical procedures was also performed in the same period, the last in mid-2010 for a total knee replacement (Table 1; Figure 1). At that time a synovial biopsy showed the inflamed synovium with hypertrophy of the lining layer (3−4 layers thick). Cell expression was also increased in the subsynovial lining and large follicle-like aggregates were visible in the tissue. Immunochemical staining (Figure 2) showed the presence of CD3 (T cells), CD20 (B cells), CD68 (macrophages), and CD138 (plasma cells). In one of the germinal center-like structures one can see paracortical T cells surrounding B and plasma cells (CD3, CD68).

Computed tomography whole-body scan reveals surgical procedures of the shoulder, elbows, wrists, hands, knees, and ankles during a decade.
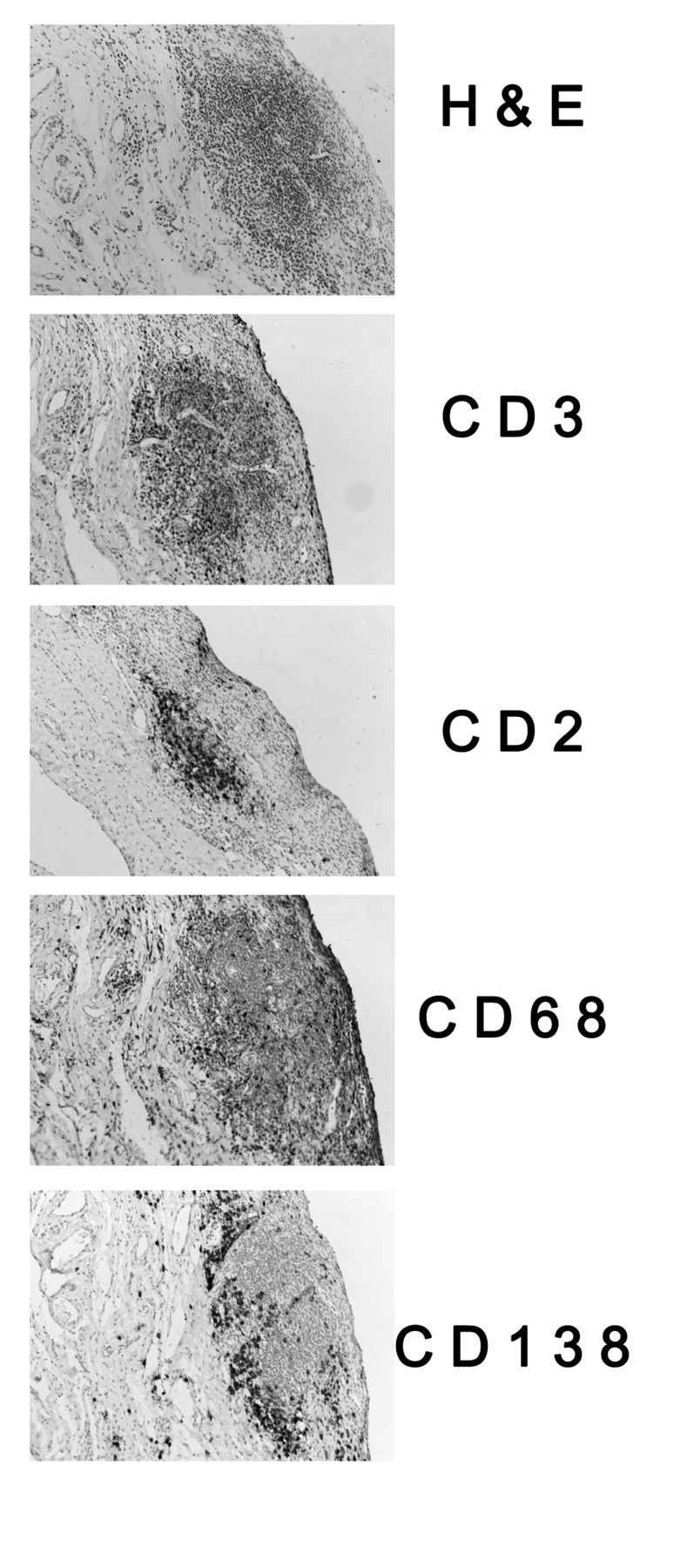
Results from immunohistochemistry analysis with all 4 conjugates that show significant staining; one shows germinal center-like follicles stained for CD20 and “paracortical” T cells, and infiltration of macrophages and plasma cells (CD3, CD138).
Orthopedic surgical procedures in our patient.
Efforts have been undertaken to evaluate the cellular components of the inflamed synovium, in an attempt to determine the precise etiologies of RA. Examination of serial synovial biopsies is now being done for screening purposes and also to establish patterns of drug resistance3. In our case, we were able to show that the synovial biopsy obtained during the last surgical procedure was associated with the presence of abundant CD68-positive macrophages and large follicle-like aggregates in the subsynovial lining. Increased numbers of CD68-positive macrophages and the presence of ectopic florid lymphoid neogenesis in the synovium have been reported to be associated with resistance to therapy; this was apparent in our case, after 10 years of biologic treatment4,5,6. Similarly, the presence of subtypes of B cells such as CD79a-positive B cells has recently been shown to be increased in the synovial membrane; the investigators suggest that may be a helpful biomarker for disease activity in RA7.
Current findings support the notion that synovial cellular markers may be used in the future to identify patients who are at risk of having destructive disease. The gradual introduction of new biologics as targeted therapies in the early phase of disease is needed to prevent disease progression and irreversible joint damage. The lack of such early targeted therapy is clearly demonstrated in our patient, who had active disease in spite of a decade of biologic therapy with compounds with different mechanisms of action8.








{kind=link}
{kind=link}