

Abstract
Objective. This case-control study was designed to evaluate magnetic resonance imaging (MRI) findings of knee joints in patients with psoriasis without clinical peripheral or axial joint involvement, and to correlate MRI findings with disease and demographic variables.
Methods. In total 48 patients with psoriasis and no clinical evidence of synovitis or enthesitis in any peripheral or axial joints were enrolled. A random sample of 20 healthy subjects without knee or other joint complaints and matched for age and sex served as controls. All patients and controls underwent enhanced MRI studies of both knee joints, and MRI findings were compared.
Results. Among 48 patients (96 knees), a total of 90 entheseal lesions were detected, with no enthesitis in 2 cases (6.3%). Signs of continuing inflammation bilaterally were frequently found: soft tissue edema (STE; n = 52), bone marrow edema (BME; n = 20), perientheseal BME (n = 3), cartilaginous erosions (n = 42), and bone erosions (n = 27). In controls, 2 (10%) subjects had BME and another 5 (25%) showed cartilaginous erosions. None showed evidence of enthesitis. Significant correlations were observed between the number of entheseal lesions of both knees vs STE (present vs absent; r = 0.314, p = 0.030) and STE (number of lesions; r = 0.351, p = 0.014). Enthesitis (unilateral vs bilateral) was significantly and positively correlated with STE (r = 0.304, p = 0.036), cartilaginous erosions (r = 0.304, p = 0.036), and villous projections (r = 0.347, p = 0.016).
Conclusion. Subclinical synovitis and enthesitis are frequently found in the knee joint of patients with psoriasis. These may be an early sign of psoriatic arthritis.
- KNEE ENTHESITIS
- ENHANCED MAGNETIC RESONANCE IMAGING
- PSORIASIS
- SUBCLINICAL SYNOVITIS
- SERONEGATIVE SPONDYLOARTHROPATHY
“Enthesitis,” the term used to describe inflammation at tendon, ligament, or joint capsule insertions, is included in the European Spondylarthropathy Study Group criteria for the classification of spondyloarthropathy (SpA). Evaluation of entheseal-related changes at different joints by magnetic resonance imaging (MRI) became an important topic on the research agenda in both differentiated and undifferentiated arthritis. If enthesitis is the primary event and synovitis follows, the presence of enthesitis among patients with psoriasis with no evidence of clinical arthritis could be a predictor of psoriatic arthritis (PsA)1.
The advent of MRI and better understanding of joint microanatomy including the complexity of joint entheses provide a unifying anatomical and biomechanical concept that links disease at the apparently disparate sites of involvement in PsA, including the synovium, enthesis, bone, and periosteum. These findings suggest an explanation for the localization of disease to skeletal sites that are subject to repeated mechanical stress2. There appear to be 2 patterns of inflammation: the “rheumatoid arthritis” (RA) phenotype, where synovial involvement is the primary target of inflammation, and the “SpA” pattern, where enthesitis comes first, followed by synovitis1,3,4,5.
Regarding enthesitis of the knee joint in SpA, McGonagle and colleagues3 were the first to describe characteristic MRI entheseal changes involving the knee joints in a cohort of 10 patients with SpA (3 of whom had PsA) with knee swelling of recent onset. This finding was confirmed by our group5. We compared enhanced MRI findings of the knee joints in 3 groups of patients, undifferentiated arthritis (UA; n = 25), established RA (n = 15), and SpA (n = 15), and found that enthesitis was a common feature on MRI in the SpA group, was totally absent in the group of patients with RA, and was observed in 3 patients in the UA group. We recommended that enthesitis as found on MRI could help to classify patients presenting with UA of the knee joint. Our group4 investigated enthesitis and entheseal-related changes shown on knee MRI among patients with several SpA. We found enthesitis in the knees of 56 patients including 30 with PsA, 5 with ankylosing spondylitis, 5 with reactive arthritis, 5 with ulcerative colitis, and 5 with Crohn’s disease. A provocative finding was the presence of enthesitis of the knee joint among 6 patients with psoriasis without clinical synovitis, who were not receiving any disease-modifying antirheumatic drugs (DMARD). In the psoriasis group (n = 6), 1 had bone marrow edema (BME), and enthesitis was detected in 5 patients at the patellar tendon insertion (PTI) and in 1 case in the medial patellofemoral ligament (MPFL)4.
These preliminary findings led us to look for enthesitis and entheseal-related changes in the knees among patients with only psoriasis without clinical evidence of peripheral or axial joint involvement, and to analyze a possible relation between enthesitis and other variables (such as demographic data, disease characteristics, severity and extension of psoriatic lesions) with other MRI signs suggestive of continuing inflammation in the knee joints [such as soft tissue edema (STE), BME, perientheseal BME, and cartilaginous and bone erosions].
MATERIALS AND METHODS
Study population
Consecutive outpatients with psoriasis were included with no clinical evidence of synovitis or enthesitis at clinical examination. A convenience sample of 20 healthy subjects with no knee complaints served as a control group.
Clinical evaluation and assessment
At baseline, a full history was taken and a complete clinical examination was performed. Detailed rheumatological examinations included peripheral and axial joint assessment (sacroiliac joints, axial mobility tests, and chest expansion), evaluation of extraarticular features such as nail lesions (pits and onycholysis), dactylitis, enthesitis, distal interphalangeal joint involvement, and tenosynovitis.
Skin assessment
The Psoriasis Area and Severity Index (PASI) is used to express the severity of psoriasis6. It combines the severity (erythema, induration, and desquamation) and percentage of the affected area into a single score in the range 0 (no disease) to 72 (maximal disease) as follows.
Severity
A representative area of psoriasis is selected for each body region. The intensity of redness, thickness, and scaling of the psoriasis is assessed as none (0), mild (1), moderate (2), severe (3), or very severe (4).
Area
The percentage area affected by psoriasis is evaluated in the 4 regions of the body (head and neck, upper limbs, trunk, lower limbs). In each region, the area is expressed as nil (0), 1%−9% (1), 13%−29% (2), 30%−49% (3), 50%−69% (4), 70%−89% (5), or 90%−100% (6)6.
MRI protocol and data acquisition
MRI/gadolinium-enhanced MRI was undertaken for both knees in all patients. Results are given as per-patient, to increase sensitivity. A General Electric echo speed 1.5-Tesla MR unit equipped with a dedicated cylindrical knee coil was used. Sagittal, coronal, and axial T1-weighted spin-echo MR images were obtained with the following MRI sequences: coronal T2-weighted TR: repetition time (TR)/echo time (TE) 2600−24/68, matrix size 256 × 160, section thickness 4 mm, spacing 0.5 mm, field of view (FOV) 16 × 16; coronal short-tau inversion recovery sequence (STIR) TR/TE 5250−94/68, matrix size 256 × 160, section thickness 4 mm, spacing 0.5 mm, FOV 16 × 16; sagittal T2 TR/TE 2600−24/68, matrix size 256 × 160, section thickness 4 mm, spacing 0.5 mm, FOV 16 × 16; sagittal STIR TR/TE 5250-49, matrix size 256 × 160, section thickness 4 mm, spacing 0.5 mm, FOV 16 × 16; axial T1 TR/TE 450−11.2, matrix size 320 × 192, section thickness 4 mm, spacing 0.5 mm, FOV 16 × 16; and axial T2 TR/TE 2600−23.5, matrix size 256 × 192, section thickness 4 mm, spacing 0.5 mm, FOV 16 × 16. Immediately after the acquisition of baseline images, an 0.05 mmol/kg body weight intravenous bolus of Gd-DTPA (Schering, Berlin, Germany) was given, including fat saturation.
Interpretation of MRI findings
MR images were evaluated for the following radiological signs before and after intravenous contrast injection: BME, perientheseal BME, bone erosions, cartilaginous erosions, synovial enhancement and degree of synovial thickness, Baker’s cyst, periarticular soft-tissue edema, and knee effusion.
Articular cartilage was assessed for contour (smooth vs irregular) and focal destruction (intact, superficial loss and/or thinning, or deep erosions to subchondral bone). Bone was assessed for marrow signal intensity abnormalities and focal erosions. Maximal synovium thickness was measured in the suprapatellar pouch on sagittal T1-weighted Gd-enhanced images, as in our earlier studies4,5. Special emphasis was given to the following entheseal sites and they were carefully evaluated for abnormalities: the quadriceps tendon insertion and the proximal and distal patellar tendon. The iliotibial band insertion, the medial collateral ligament (MCL) origin and insertion, the lateral collateral ligament (LCL) origin and insertion, the lateral capsular insertions, the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL) origins and insertions, PTI, biceps femoris insertion, semimembranosus insertion, MPFL, and lateral patellofemoral ligament (LPFL). Focal areas of abnormal signal adjacent to the superior and inferior attachments of the posterior capsule and related calf muscle origins were also considered as enthesitis.
MRI findings and data interpretation
Two observers, blinded to the diagnosis, interpreted the MRI findings in all patients and controls. Before interpretation of MR images standards were established to look for all potential sites of enthesitis and entheseal-related changes in both groups in the following anatomical sites — ACL, PCL, LCL, MCL, MPFL, LPFL, and PTI.
To avoid overreading or misinterpretation, potential entheseal sites were evaluated by T2 fat saturation and STIR sequences for the assessment of the tendon fibers, together with proton-density fat saturation for assessment of perientheseal soft-tissue edema, and perientheseal BME with evident high signal intensity in case of enthesitis. To avoid misinterpretation due to the “magic angle” effect, we relied on long TE pulse sequence for the assessment of tendon or ligament fibers. In case of disagreements, the findings were discussed according to the previous standards until agreement was reached7.
Statistical analysis
Quantitative variables were described using mean ± SD and categorical data by frequency and percentage. The Pearson chi-square test was used to test differences among categorical variables among the groups of patients, and Student’s t test was used to compare quantitative variables; in all tests, p value < 0.05 was considered to be statistically significant.
The study was approved by the local ethics committee of the Dr. Erfan and Bagedo General Hospital and followed the principles of the Declaration of Helsinki; all patients and controls gave written informed consent before participation.
RESULTS
A total of 48 consecutive outpatients [26 women (54.2%) and 22 men (45.8%)] were included with psoriasis only and with no clinical evidence of synovitis or enthesitis at clinical examination. There were no refusals. Twenty healthy subjects [12 women (60%) and 8 men (40%)] matched for age and sex with no knee complaints served as controls. The mean age of the patient group was 42.2 ± 7.5 years, and in controls 40.65 ± 7.278 years. There were no significant differences between the 2 groups regarding age and sex (p = 0.421, p = 0.659, respectively).
Demographic and disease characteristics, PASI, and laboratory findings among the study group are described in Table 1. MRI scans identified unilateral knee enthesitis in 22 (45.8%) and bilateral in 23 (47.9%) cases.
Demographic and clinical characteristics and laboratory findings among the patients with psoriasis (n = 48). Data are mean ± SD or no. (%).
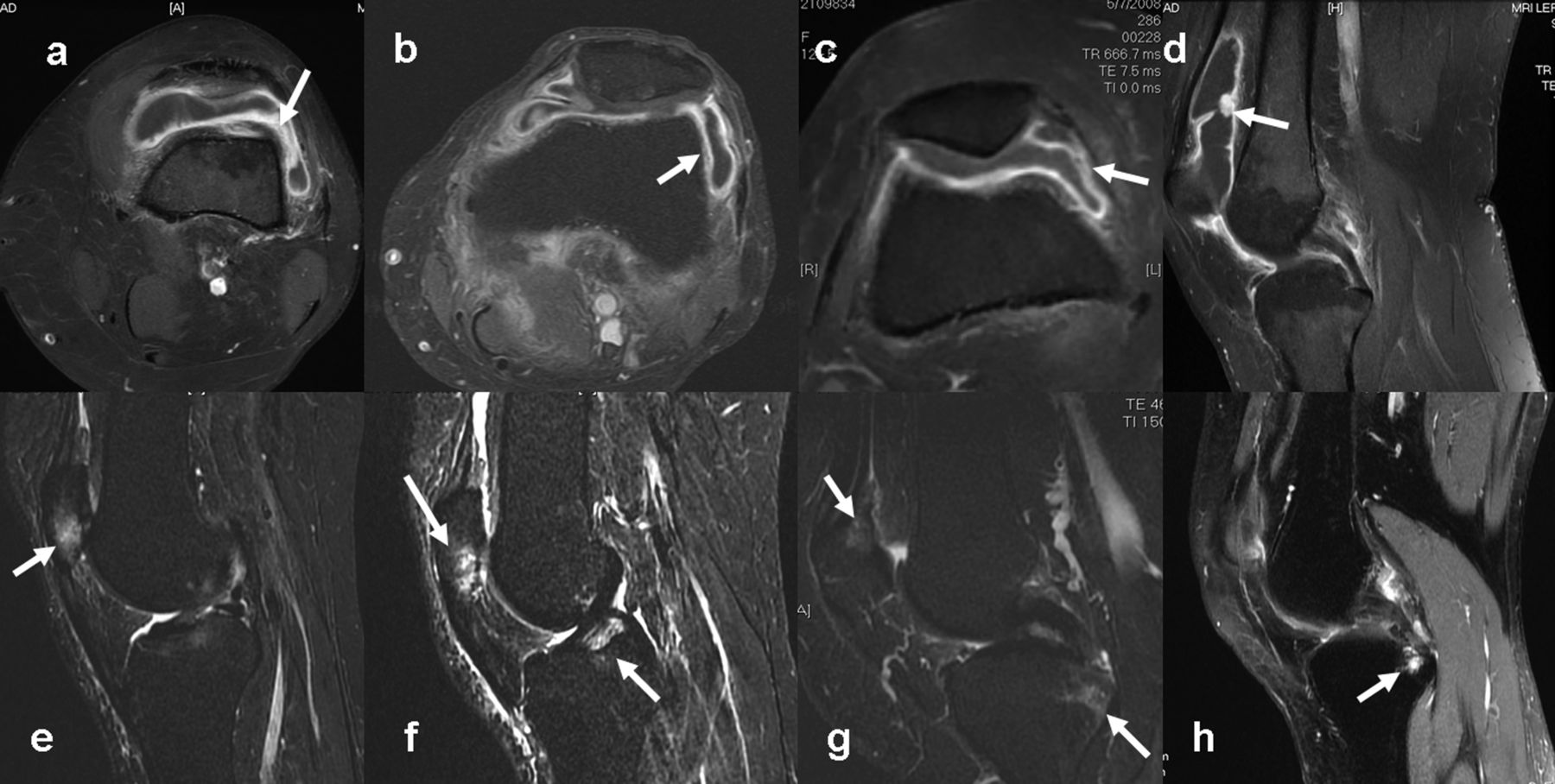
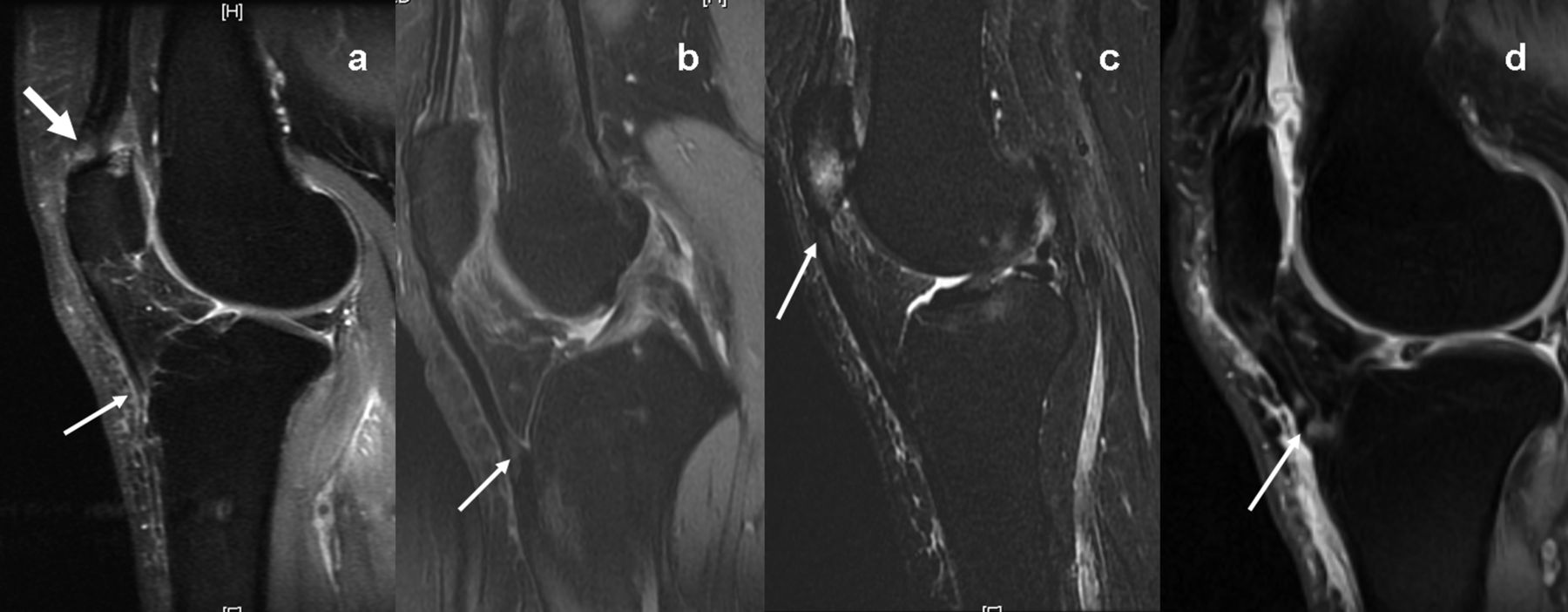
Detailed MRI findings among patients are described in Table 2, including synovial thickness (Figure 1A–1D), villous projections (Figure 1D), knee effusion grading, STE, BME (Figure 2A, 2B), perientheseal BME (Figure 3E), and cartilaginous and bone erosions (Figure 1E–1H). Knee enthesitis was absent in 3 cases (6.3%) and 90 lesions were identified by MRI of the knees (Figures 3 and 4). No significant statistical differences between the right and left knees were observed by any of these MRI findings (p > 0.05). In the right knee, MCL enthesitis was identified in 4 (8.3%; Figure 3C, 3D), LCL in 5 (10.4%; Figure 3E), ACL in 3 (6.3%; Figure 3H), PCL in 2 (4.2%), PTI in 21 (43.8%; Figure 1B, 1D), MPFL in 5 (10.4%; Figure 1C), and LPFL in 3 cases (6.3%); the total number of entheseal lesions in the right knee was 43. In the left knee, MCL enthesitis was observed in 9 (18.8%), LCL in 8 (16.7%), ACL in 2 (4.2%), PCL in 3 (6.25%), biceps femoris insertion (intracapsular and extrasynovial) in 1 (2.1%), PTI in 12 (25%; Figure 4), MPFL in 9 (18.8%; Figure 3G), and LPFL in 3 cases (6.3%); the total number of entheseal lesions in the left knee was 47. No significant differences were observed between right and left knees regarding the different entheseal lesions (p > 0.05).

A–D. Postcontrast T1 fat saturation magnetic resonance imaging (MRI) scan showing moderate knee effusion with synovial enhancement and villous projection in panel D. E–H. Sagittal T2 fat saturation MRI scan showing examples of bony and cartilaginous erosions close to the entheseal insertion of quadriceps (E–G) and posterior cruciate ligament (H).

A. Sagittal T2 fat saturation magnetic resonance imaging (MRI) scan showing bone marrow edema (BME) of the posterior aspect of the medial femoral condyle. B. Coronal T2 fat saturation MRI scan showing BME of femoral condyle. C. Sagittal T2 fat saturation MRI scan showing focal bone erosions of the upper patellar pole. D. Sagittal T1 scan showing patellar cartilaginous erosions (arrow).

A, B. Sagittal T2 fat saturation magnetic resonance imaging (MRI) showing enthesitis of quadriceps tendon (arrows). C, D. Coronal proton density (PD) and T2 fat saturation MRI scans showing enthesitis of the medial collateral ligament (MCL; arrows). E, F. Axial PD fat saturation MRI scan showing enthesitis of the lateral collateral ligaments with associated perientheseal bone marrow edema (arrows). G. Axial T2 fat saturation MRI showing combined enthesitis of the medial patellofemoral ligament and MCL insertions (arrow). H. Sagittal PD fat saturation MRI showing enthesitis at the foot plate of the anterior cruciate ligament (arrow).

A. Sagittal postcontrast T1 fat saturation magnetic resonance imaging (MRI) showing focal enhancement at the patellar insertion (thin arrow) and quadriceps tendon attachment to the upper patellar pole (thick arrow). B. Sagittal T2 fat saturation MRI scan showing hyperintensity at the patellar tendon (arrow). C. Sagittal STIR image showing hyperintensity and marrow edema at the upper patellar tendon attachment (arrow). D. Sagittal T2 fat saturation MRI scan showing hyperintensities at the patellar tendon insertion (arrow).
MRI findings among the study patients. Data are mean ± SD or no. (%).
In Table 3, detailed correlations are summarized between the numbers of entheseal lesions detected in right and left knees and enthesitis (unilateral vs bilateral) versus demographic and disease characteristics and other MRI findings.
Comparison of body mass index (BMI) and MRI findings among patient and control groups.
No significant difference was observed between patients and control groups regarding body mass index (p = 0.11), while significant differences were observed between groups regarding BME (p = 0.011) and cartilaginous erosions (p < 0.001; Table 3). In the controls, 2 subjects (10%) had BME and another 5 (25%) showed cartilaginous erosions; none showed evidence of enthesitis.
Significant correlations were observed between the number of entheseal lesions of right and left knees versus STE (present vs absent; r = 0.314, p = 0.030), and number of STE lesions observed (r = 0.351, p = 0.014). Enthesitis (unilateral vs bilateral) was positively correlated with STE (r = 0.304, p = 0.036), cartilaginous erosions (present vs absent; r = 0.304, p = 0.036), and villous projections (r = 0.347, p = 0.016; Table 4). Neither age nor disease duration showed any correlation with the total number of entheseal lesions (r = 0.042, p = 0.776 and r = −0.030, p = 0.841, respectively; Table 4).
Correlations between number of entheseal lesions of both right and left knees and enthesitis (unilateral vs bilateral), versus demographic and clinical characteristics and MRI findings.
DISCUSSION
Our case-control study was designed to investigate enthesitis and subclinical synovitis of the knee joint in a cohort of patients with psoriasis without clinical evidence of axial or peripheral joint involvement.
Many factors appear to play a role in the development of PsA in patients with psoriasis. It was found that lifting heavy loads and infections that required antibiotics were associated with the occurrence of arthritis in patients with psoriasis. There was an inverse association between smoking and PsA8. In a followup study of 313 patients with psoriasis over 4 years by the same group, the annual incidence rate of PsA was found to be 1.87 cases per 100 patients with psoriasis, particularly among patients with moderate to severe psoriasis9.
Historically, “enthesitis” has been considered a disorder of a focal attachment site; however, another concept considers that entheses together with adjacent tissues may form mini-organs, dubbed “enthesis organs” by Benjamin and colleagues10. On an anatomical basis, the normal “enthesis organs” can be broadly classified as joint-related (here called “articular”) or extraarticular, according to whether the enthesis lies internally or externally to the capsule of a synovial joint11. At many locations there is a whole group of tissue modifications in the immediate vicinity that collectively constitute an enthesis organ. Each component plays a role in the overall task of stress dissipation12.
Since the 1970s, it has been recognized that inflammatory lesions can develop without symptoms or signs that are recognizable by the patient and the physician. Such patients can be considered to have subclinical or “occult” PsA. The concept of occult involvement in PsA could also be extended to patients already diagnosed with PsA in whom instrumental methods allow identification of more extensive disease, such as axial involvement in patients who have only clinical peripheral arthritis/enthesitis, or polyarticular/entheseal involvement in patients with clinical oligoarthritis/enthesitis. Further research regarding the recognition and progression of these occult forms could permit successful early management of PsA13. MRI opened a new avenue of research to explore hidden signs that can contribute to the understanding of early disease changes in disorders of the SpA group.
With respect to psoriasis, evidence of subclinical synovitis was previously supported and addressed a few times in the literature using different techniques and in different joints. In the earliest report, Namey and Rosenthall14 described markedly abnormal bone scintigraphy with symmetrically increased periarticular uptake about the imaged joints in patients with psoriasis. Regarding hand joints, Offidani, et al15 reported signs of occult synovitis by MRI that were found in 68% of patients including joint or tendon sheath effusions, bone erosions, and BME. In established cases of PsA, Jevtic and coworkers16 using MRI described inflamed tissue in the hand joints extending far beyond the joint capsule, thickened collateral ligaments, and surrounding periarticular soft tissue, a pattern that is quite different from that observed in patients with RA. In another report, Tan, et al17 showed, using MRI, prominent inflammatory changes in ligament, tendon, enthesis, and adjacent bone in the distal interphalangeal (DIP) joints of patients with PsA, and similar findings were observed in DIP joints among patients with osteoarthritis (OA) but to a lesser extent.
Entheseal abnormalities have been documented by ultrasonography (US) in clinically asymptomatic patients with psoriasis. These findings could relate to a subclinical entheseal psoriatic inflammation18. Naredo, et al19 reported in 162 patients with plaque psoriasis without musculoskeletal disease that patients with psoriasis had a significant prevalence of asymptomatic US synovitis and enthesopathy, which may indicate a subclinical musculoskeletal involvement. Additionally, 49 (36%) patients showed both synovitis and enthesopathy. As in our study, Naredo, et al19 observed with US no significant differences between psoriatic patients with and those without joint synovitis in terms of demographic data and PASI scores.
In our study a total of 90 entheseal lesions were identified by MRI in both right and left knees and in only 3 cases (6.3%) was enthesitis absent. This large number of entheseal lesions may be explained by the sensitivity of MRI compared to US from the technical point of view. Further, an important sign on MRI is BME, which cannot be detected except with the use of MRI. In our study 20 cases showed evidence of BME signs in both knees.
We have confirmed in a large series of patients with psoriasis the findings of knee enthesitis in almost all cases and other signs of synovitis as well. Importantly, we ensured the presence of MRI enthesitis at different anatomical sites by combined interpretation of STIR sequences as a sensitive measure for detection of perientheseal BME, while T2 fat saturation was better for anatomical delineation of the entheseal organ. In our study, no controls showed evidence of enthesitis on MRI and only 2 subjects (10%) had BME, and another 5 (25%) showed cartilaginous erosions, which can be explained as early osteoarthritic age-related changes. However, the later findings were significantly higher in the patient group compared to the controls (p = 0.01, p < 0.001, respectively), and this again may be indicative of a subclinical form of synovitis among patients with psoriasis. The other important finding is the presence of villous projections, which is in our opinion an early phase for pannus formation, reflecting the early inflammatory process. In recent work Gibson and coworkers20 observed no increase in the prevalence of hand enthesophytes among patients with knee BME on MRI scans. This in turn provides evidence against a systemic enthesopathic disorder in association with knee OA.
Prospective studies in patients with early SpA will be necessary to determine whether enthesitis and synovitis coexist at all stages of synovitis, or if in fact synovitis eventually becomes autonomous21. Moreover, in PsA, subclinical enthesopathy including osteitis is common in subjects with psoriasis but without arthritis22.
In our study it was notable that the total number of entheseal lesions in right and left knees was positively correlated with STE (present vs absent; p = 0.03) and with number of STE of both right and left knees (p = 0.014). On the other hand, enthesitis (unilateral vs bilateral) was positively correlated with STE (present vs absent; p = 0.036), cartilaginous erosions (present vs absent; p = 0.036), number of STE lesions of both knees (p = 0.031), and villous projections (whether taken as present vs absent or number of lesions of both knees; p = 0.019, p = 0.016, respectively). Such clear correlations indicate a close link of enthesitis with other important MRI signs previously mentioned, which definitely indicate continuing inflammation that remains subclinical and cannot be observed except with the use of a sensitive technique such as MRI. None of our patients received methotrexate (MTX) therapy to control their skin disease at the time of the study. Low-dose MTX is an effective treatment for psoriasis and PsA23.
A drawback in our study is that we did not have 2 observers presenting 2 separate scores, which would have made it possible to estimate interobserver reliability. We chose the agreement method7, which is less robust. We followed a “gold standard” interpretation of all MRI findings and all findings were individually discussed until agreement was reached.
In the knee joints of patients with psoriasis, MRI showed evidence of subclinical synovitis and enthesitis that were more frequent with extracapsular enthesitis compared to intracapsular involvement. Enthesitis was positively and significantly correlated with other important MRI signs, such as villous projections, STE, and cartilaginous erosions, that were indicative of continuing subclinical synovitis. These findings indicate that enthesitis may be an early sign (perhaps the earliest) of subclinical psoriatic arthritis.
- Accepted for publication June 20, 2012.








{kind=link}
{kind=link}
{kind=link}
{kind=link}