

Abstract
Objective. To investigate sex differences in response to anti-tumor necrosis factor-α (TNF-α) therapy over time in early versus established rheumatoid arthritis (RA).
Methods. Patients with RA who initiated anti-TNF therapy between January 2003 and June 2008 in Denmark were selected from the DANBIO Registry. Sex differences in baseline disease features were examined using chi-square, Mann-Whitney U tests, and t tests. Using a generalized estimating equations (GEE) model for repeated measures, we examined European League Against Rheumatism (EULAR) responses in men and women over 48 months of followup, adjusting for baseline values of age, 28-joint Disease Activity Score (DAS28), disease duration, and anti-TNF, methotrexate, and prednisolone use.
Results. At initiation of anti-TNF therapy (baseline), 328 women and 148 men had early RA (≤ 2 yrs), and 1245 women and 408 men had established RA (> 2 yrs). In both early and established RA, men and women had active disease with similar DAS28 scores (mean ± SD 5.2 ± 1.1), physician global scores, swollen joint counts, and radiographic changes. In early RA, men were significantly more likely to achieve a EULAR good/moderate response over 48 months compared to women (GEE; p = 0.003), and a significant interaction between sex and followup time (GEE; p < 0.0005) suggested that men achieved this response sooner than women.
Conclusion. Better responses to anti-TNF therapy among men compared to women in early but not established RA suggest that disease duration at initiation of therapy may be an important factor to consider when investigating sex differences in treatment responses.
It is well established that there is a strong sex bias in the occurrence of rheumatoid arthritis (RA), women being affected at least 3 times more often than men1. Sex differences in RA outcomes, including disease activity and functional capacity in early2,3 as well as longstanding disease4,5,6, have been described, although not yet established. Over the last few years, a uniform trend appears to be emerging from studies that examined sex as a potential predictor of remission in RA — increased remission rates in response to conventional as well as biologic disease-modifying antirheumatic drugs (DMARD) have been consistently observed among men compared to women2,7,8,9,10,11,12,13.
There seems to be a consensus among recent studies of early RA that in the early stages of the disease, disease activity measures are similar between men and women, and over time, women have a worse disease course than men despite similar treatment2,3,14,15,16; hence, men are more likely to achieve better responses. Thus, in early RA, sex differences in treatment outcomes only become apparent as the disease evolves. It has not yet been investigated whether the sex differences in treatment responses observed in early RA are also present when treatment is initiated 2 or more years after diagnosis, i.e., in patients with established RA. Studies of patients with RA of variable disease durations that examined the influence of sex on treatment responses have yielded conflicting findings13,17, and did not address the possible role of RA duration at the start of treatment.
In our study, we specifically investigated whether the duration of RA when anti-tumor necrosis factor-α (TNF-α) therapy was started, i.e., early RA (≤ 2 years since diagnosis) versus established RA (> 2 years since diagnosis), influenced treatment responses differently among men compared to women. To address this question, we examined sex differences in European League Against Rheumatism (EULAR) responses over 48 months of followup in a large prospective cohort of patients with RA from the national DANBIO Registry in Denmark18 from the time the patients started anti-TNF therapy.
MATERIALS AND METHODS
Patients
Patients with RA throughout Denmark are enrolled in the observational DANBIO Registry when they are first prescribed biologic treatment18. For our study, patients with RA who initiated anti-TNF therapy (adalimumab, etanercept, or infliximab) for the first time, from January 1, 2003, to June 30, 2008, were selected from the DANBIO Registry. All patients satisfied the 1987 American College of Rheumatology (ACR) criteria for RA19. As mandated by Danish law, DANBIO was approved by the Danish Data Registry, and by the National Board of Health, and written informed consent was not required.
Data collected
All patients were examined by rheumatologists when biologic therapy was first prescribed (study baseline), and about every 6 months thereafter. Clinical and demographic data from each of these timepoints, as well as data for prescriptions and outcomes for anti-TNF and other therapies used, were stored in the DANBIO Registry. For our study, data available at each 6-month interval were used for the analyses, for a total followup time of 48 months. These included 28-joint counts for tender (TJC28) and swollen joints (SJC28), as well as self-reported measures such as patient global health. Blood samples drawn at baseline and at each followup were used to evaluate levels of C-reactive protein (CRP). It should be noted that since DANBIO is a national registry mandated by Danish law, all subjects enrolled should remain in the database for as long as they continue to obtain treatment in hospital rheumatology departments in Denmark. Therefore, in principle, there is no loss to followup until a subject stops treatment, dies, or moves out of the country. However, for our study, although nearly complete data were available from patients and rheumatologists at enrollment into the registry, data for random variables were missing at various timepoints in different patients. Further, for patients enrolled in DANBIO after May 2005, followup time was < 48 months, as the study observation time ended in May 2009.
Disease activity
RA disease activity was assessed by the Disease Activity Score (DAS) calculated on 4 variables including 28-joint counts and CRP (DAS28CRP4 scores)20:
RA treatment outcomes
Changes in RA symptoms from baseline were assessed using EULAR criteria for treatment response22,23. Trends in DAS28 scores were also evaluated over time to assess responses to treatment. Patients who were already in remission at baseline (DAS28 < 2.6)21 were excluded from the analyses (n = 82).
Statistical analyses
Patients were separated into 2 groups based on RA duration at baseline: early RA (duration ≤ 2 years) and established RA (duration > 2 years). All analyses were performed in each of these 2 patient groups separately.
Cross-sectional differences between sexes at baseline
Summary statistics for men and for women were calculated as means and SD for symmetrically distributed continuous variables, and medians with 25th and 75th percentiles, for non-normally distributed continuous variables. For categorical variables, proportions of patients within each patient group were computed. Sex differences in disease features at baseline were examined using chi-square tests to compare distributions of categorical variables between men and women, and the Mann-Whitney U test and t test for continuous variables.
Longitudinal analyses of treatment outcomes in men and women (0–48 months)
Generalized estimating equations (GEE) models, with an independent correlation structure, were used to model differences in EULAR responses (categorized as a binary variable, i.e., no response vs moderate/good response) between men and women over time (0–48 months), taking into account within-subject correlations in repeated measurements during the followup. In the GEE models, followup time and sex (male sex as the referent group) were included as the main explanatory variables, adjusting for baseline values of age, disease activity (DAS28), disease duration, anti-TNF therapy, and use of methotrexate (yes/no) and prednisolone (yes/no). An interaction term (sex*followup time) was included to assess whether the time taken to achieve a moderate/good response was modified by sex. The mean values of the DAS28 scores were also plotted against followup time for men and women, to visually assess any differences in trends in the raw data over time within each sex. In order to illustrate how the results of the GEE model translate into probabilities of a EULAR response, we computed probabilities of achieving a moderate/good EULAR response in men and women over time in early RA and in established RA, using the regression coefficients from the model, and the mean baseline values of age, DAS28 scores, and RA duration. We also repeated the GEE analyses, using each DAS28 component as the outcome variable in the model separately, to determine which of these components may account for any observed association between EULAR response and gender.
Sensitivity analyses
Since data were missing at different timepoints on a large proportion of subjects during the 48 months of study observation time, at each timepoint we compared the mean DAS28 scores of the men and women who had data available at the next timepoint to those who did not, to assess whether there was any sex bias. Further, we repeated the longitudinal analyses in the subset of patients for whom data were available at 48 months. We also investigated whether the probability of a significant Health Assessment Questionnaire (HAQ) response from baseline (i.e., Δ ≤ −0.22) differed between men and women.
All statistical analyses were performed using the Stata software package (Release 11; StataCorp, College Station, TX, USA).
RESULTS
Baseline characteristics of the patient population
A total of 2129 patients with RA were available from the DANBIO Registry for our study. Among these patients, 476 (328 women and 148 men) had early RA and 1653 (1245 women and 408 men) had established RA. Overall, as shown in Table 1, the early RA group had later disease onset compared to the group with longstanding RA and, as expected, were less likely to have developed radiographic erosions. Otherwise, the 2 groups had relatively similar disease features, and similar mean disease activity (DAS28, mean ± SD: 5.2 ± 1.1 in both groups), with the majority of patients having moderate to severe RA disease activity, i.e., DAS28 > 3.2 (early RA: 96.2%, longstanding RA: 94.9%).
Summary of disease characteristics and medications at baseline by rheumatoid arthritis (RA) duration and sex. Results are mean ± SD or medians (interquartile range), unless otherwise indicated.
Cross-sectional differences between sexes at baseline
In both early and established RA, there were no significant sex differences in DAS28 scores, physician global scores, swollen joint counts, and in the proportions of men and women with rheumatoid factor (RF) seropositivity and radiographic changes at baseline, when anti-TNF therapy was initiated (Table 1). Men had significantly higher levels of CRP early in the disease course and were more likely to be current smokers or to have ever smoked, although these were statistically significant only in longstanding RA. Women had worse disability (HAQ-Disability Index), pain visual analog scale (VAS) scores, patient global scores, and fatigue VAS scores, and more tender joints; these differences appeared to be more pronounced in early RA, although they were not statistically significant. At baseline, about two-thirds of the patients received concomitant methotrexate, and between one-third and one-half of the patients were taking concomitant prednisolone. No important sex differences were observed at baseline in treatment patterns in early RA, whereas in longstanding RA, significantly more men were administered prednisolone compared to women. Similar proportions of men and women were prescribed each of the different biologic anti-TNF therapies (infliximab, adalimumab, and etanercept) at baseline.
Longitudinal analyses
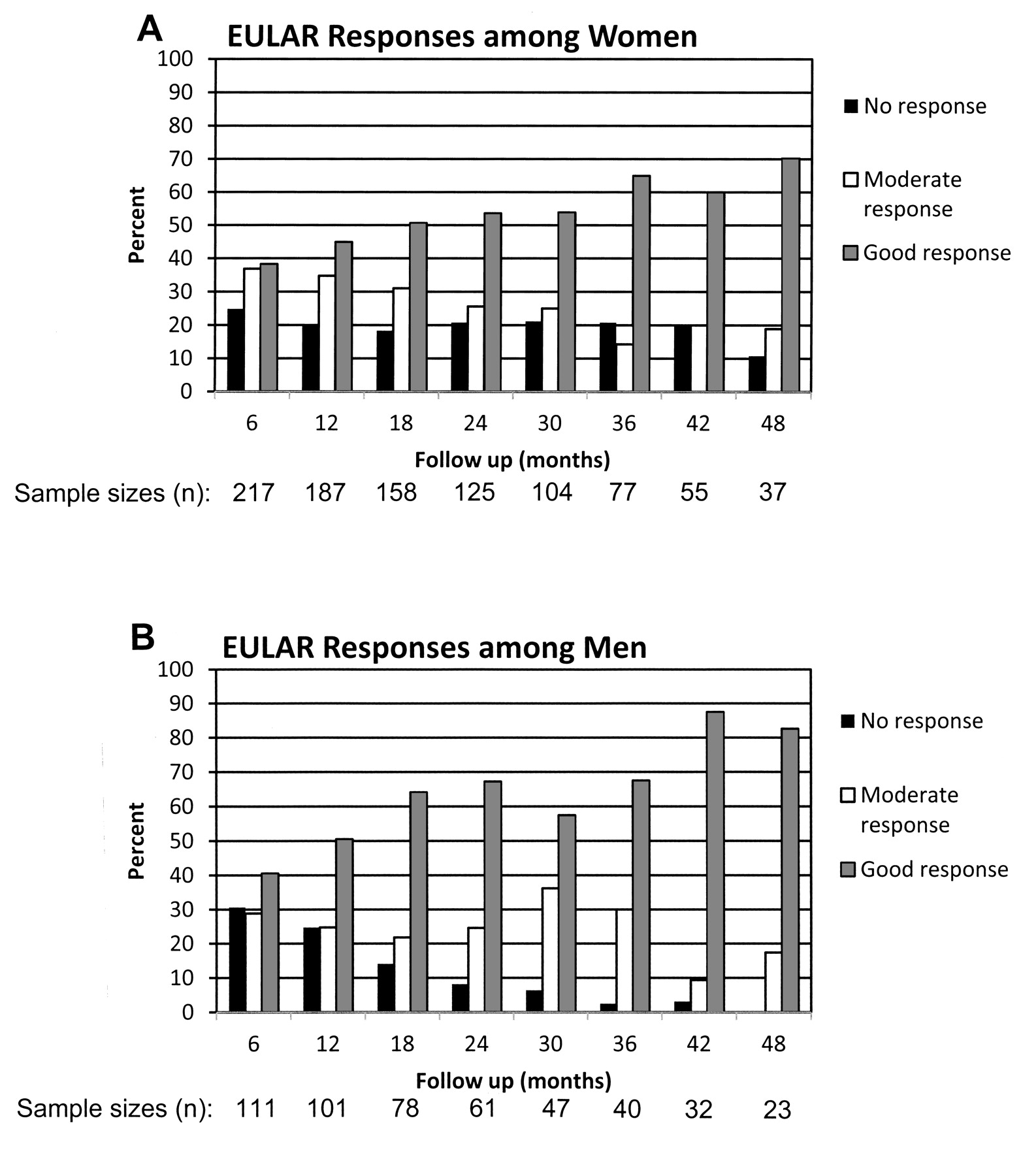
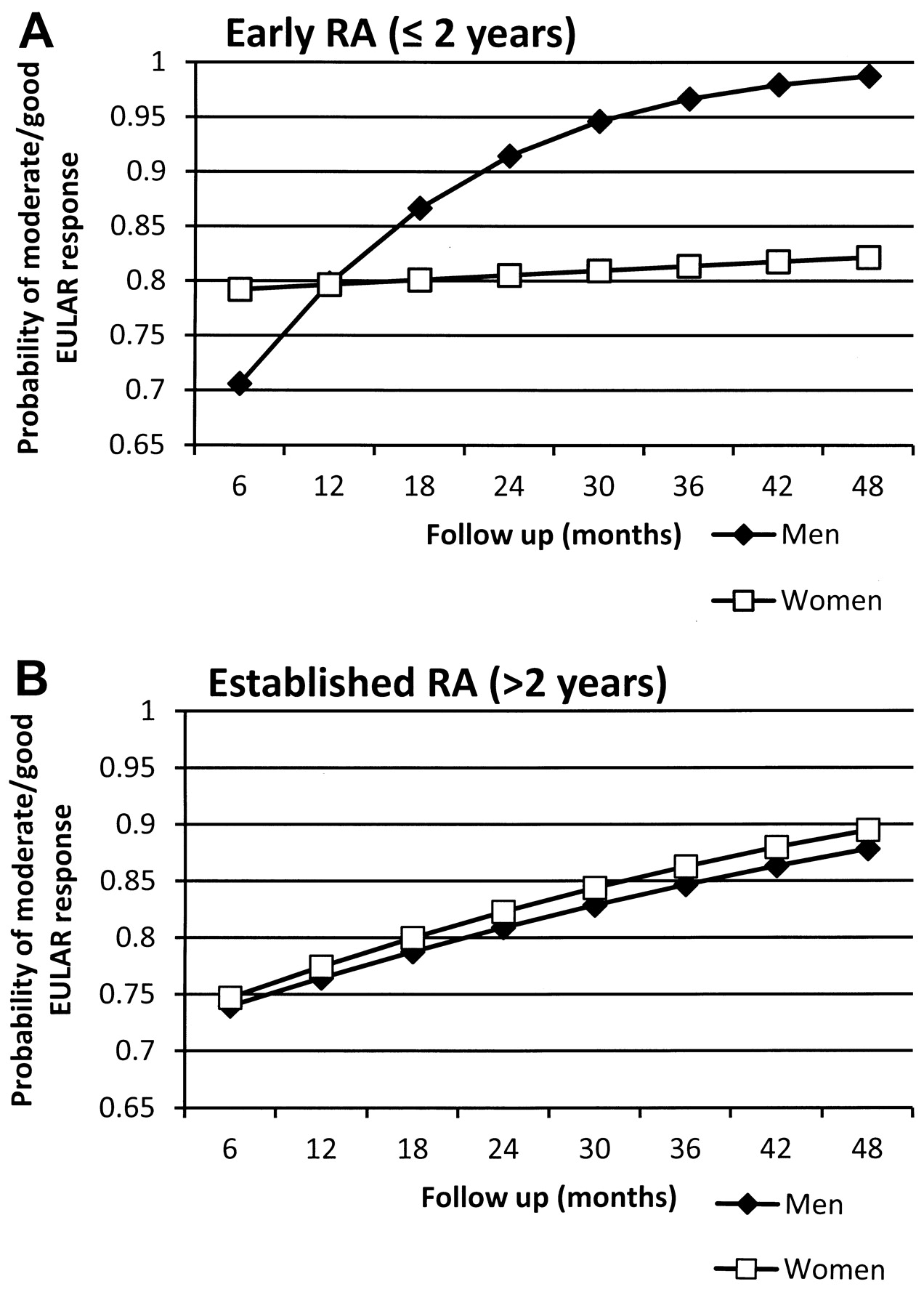
In early RA, the observed proportions of men and women with good, moderate, or no EULAR responses at each followup (Figure 1) suggest that men were more likely to achieve better responses than women. In the GEE model, with moderate/good EULAR response as the outcome (no response as the reference), the EULAR response differed significantly between men and women (Table 2). In early RA, men were significantly more likely to have better responses over time compared to women (p = 0.003). Further, being male was associated with a shorter time taken to achieve a good/moderate response, as shown by the interaction term (sex*followup time) in the model (p < 0.0005). In Figure 2A, the results from this model are further illustrated as probabilities of achieving a moderate/good response, with men expected to achieve a better response over time compared to women with similar baseline characteristics, irrespective of whether the patients were also taking methotrexate and/or prednisolone. These sex differences were also reflected in the observed trends of the mean DAS28 scores over the 48 months of followup among men and women (Figure 3). There was a comparable and significant improvement in DAS28 scores in both men and women during the first 6 months after initiation of anti-TNF therapy irrespective of RA duration; after 6 months, the rate of improvement slowed down in both sexes, but was significantly better among men in the early RA group.

The observed proportions of (A) women and (B) men with good, moderate, or no EULAR responses, as well as sample sizes, are shown for each followup. A EULAR response could not be assessed for some patients who were missing DAS28 data at baseline; thus sample sizes are smaller than those shown in Figure 3.

Expected probabilities achieving a moderate/good EULAR response over time are shown, as an example, in men versus women in (A) early RA and (B) established RA, using mean baseline values of age, 28-joint Disease Activity Score (DAS28), and RA duration computed for early and established disease — based on the GEE model in Table 2.
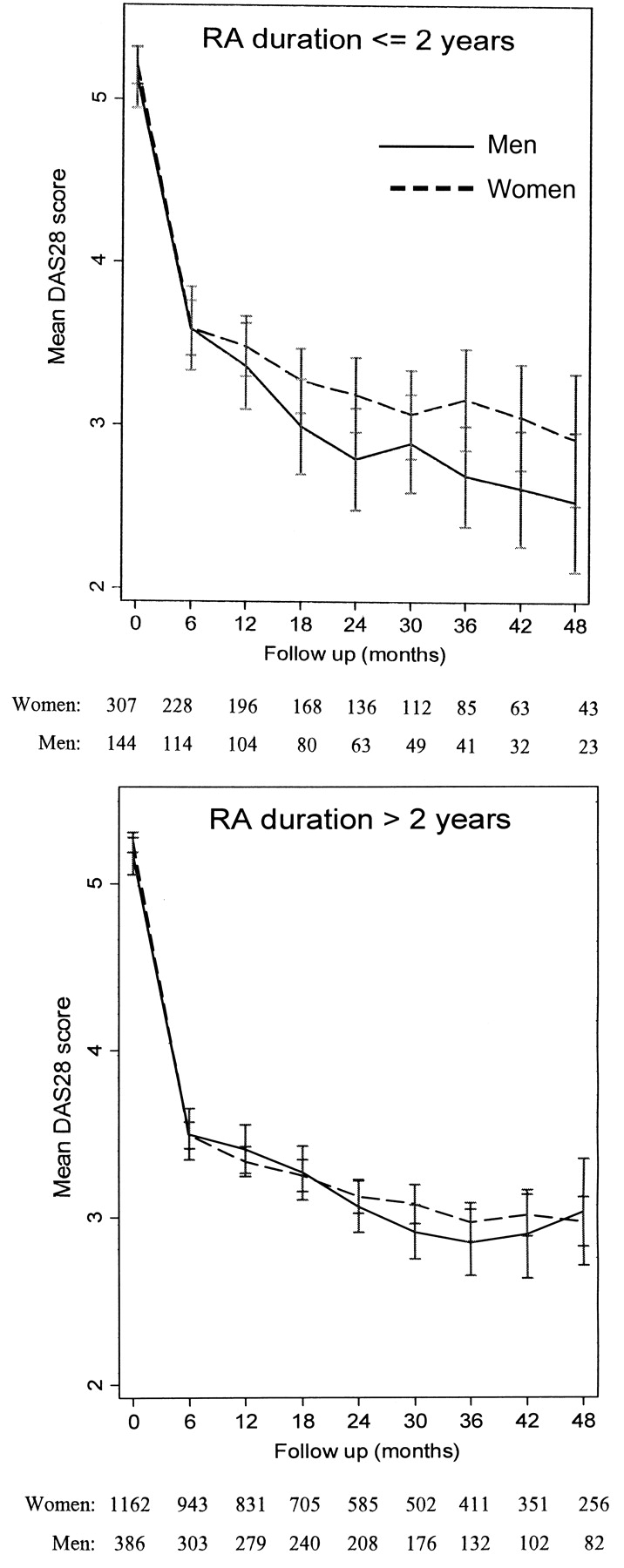
The observed mean values of the 28-joint Disease Activity Score (DAS28) among men and women in early versus established RA and sample sizes at each followup are shown.
Predictors of a moderate or good European League Against Rheumatism (EULAR) response in early and established rheumatoid arthritis (RA); generalized estimating equations (GEE) model.
Among patients with established RA, no association was found in the GEE models between sex and EULAR response or the time to achieve EULAR good/moderate response (Table 2), as also shown in Figure 3B.
DAS28 components
Among the components of the DAS28 score, only CRP showed a pattern that resembled the EULAR responses when used as the outcome variable in the GEE model (data not shown). In early RA, men initially had higher observed CRP levels (Table 1); after 12 months of followup, the levels among women increased to levels higher than in men; this difference was nevertheless not clinically significant. In established RA, on the other hand, the CRP levels were similar between men and women throughout the study period. Tender joint counts and patient global scores tended to be consistently lower among men in early RA, although the differences did not reach statistical significance. No sex differences were observed for these measures in established RA. Swollen joint counts were similar in men and women in both early and established RA.
Sensitivity analyses
At each timepoint, the men and women who had data available at the next visit had similar mean DAS28 scores as those who had missing data at the next visit (data not shown). A GEE analysis restricted to those who had data at 48 months provided results similar to those presented for the entire dataset. The probability of a significant HAQ improvement was also higher among men, especially in the early RA group (data not shown).
DISCUSSION
Our study of treatment responses to anti-TNF therapy among men and women in a large observational cohort provides novel evidence that sex differences are present in early but not in established RA. Within the DANBIO cohort, among patients who initiated therapy within 2 years of diagnosis, men achieved better and faster EULAR responses than women. This sex difference in treatment response was not seen in patients who initiated anti-TNF therapy > 2 years after diagnosis. Thus, our results indicate that duration of the disease prior to treatment being administered is important. Previous studies that investigated sex differences in treatment response have not addressed in detail the possible role of RA duration on sex modification of treatment responses, and a direct comparison of treatment responses by sex between early and established RA as we present here has not previously been reported, to our knowledge. Studies of early RA cohorts performed by us14 and by others2,7,16 suggested that maleness is a predictor of better treatment responses and/or remission in early stages of the disease, which supports our findings of better responses among men with early RA in the DANBIO cohort. It was not known, however, whether these sex differences were specific to early RA or whether similar differences could be found among patients who have established RA when treatment is initiated. It has also not been investigated whether sex differences to treatment responses are influenced by the type of treatment administered — i.e., traditional DMARD versus biologic DMARD. Nonetheless, although our knowledge about sex differences in treatment responses in RA is currently limited and based almost entirely on these studies, there is increasing evidence that men respond significantly better than women to both traditional DMARD and anti-TNF therapy in early RA. In established RA, however, there were no sex differences in responses to anti-TNF therapy in the DANBIO cohort. Additional studies of established RA are warranted to replicate these findings.
Among the components of the DAS28 score, sex differences similar to those observed for EULAR responses were also found for CRP, although minor differences in tender joint counts and patient global scores may also have contributed to the observed differences in DAS28 and EULAR responses. The mechanism responsible for the observed sex differences, and why these differences occur in early versus established RA, remains obscure. We speculate that there are intrinsic physiological sex differences that have a differential effect on the way men and women respond to treatment. For example, it has been demonstrated that men and women respond differently to low-dose aspirin, which is protective against heart attack in men but not women, and protective against stroke in women but not men24. We previously observed that in early RA, women had worse progression of the disease over a 2-year period compared to men despite having similar treatment14, and similar findings have been reported by other groups2,6,16. As to why men achieve better responses compared to women in early RA and not in established disease, we do not know. Interestingly, the observed trends in mean DAS28 scores in early and established RA suggest that women may experience similar responses to therapy irrespective of RA duration, and that the sex differences observed in early RA may be due to men responding better when treated in early rather than subsequent stages of the disease. We cannot, however, exclude the possibility that men may have a form of the disease that remits more often in the early course compared with women. Another interpretation of our findings may be that since DAS28 scores are highly dependent on pain perception, men may have a higher threshold for reporting joint tenderness and global health in early stages of the disease, but as disease duration increases, adaptive mechanisms relating to pain perception may be in operation, leading to a more similar reporting of symptoms between men and women. Nonetheless, given the current international effort to provide treatment in the early stages of RA25, this difference between men and women is worth noting, and it is possible that eventually, sex-related response thresholds may need to be established to more effectively manage the disease in men and women.
In the NorDMARD8 and GISEA9 cohorts, which were also observational, a significantly higher proportion of men had already achieved a good EULAR response or DAS28 remission by 6 months after initiation of anti-TNF therapy. In contrast to these studies, we found men and women to have a similar improvement in both early and established RA during the first 6 months. We have made similar observations in an independent early RA observational cohort (the Western Consortium of Practicing Rheumatologists cohort), as reported14, although the patients in that study were treated with traditional and not biologic DMARD.
Our study has a number of limitations related to its observational design and incomplete followup. First, the patients were selected because they had initiated anti-TNF therapy and thus they represented patients with more severe RA. However, we are not aware of any selection bias in terms of sex, as both men and women had similar disease activity and treatment at study baseline. Further, the DANBIO Registry reflects routine practice of biological treatment, in real-life settings in Denmark, with > 90% national coverage. Since anti-TNF therapy can only be prescribed and administered by hospital departments of rheumatology in Denmark, and the expenses are covered by the public health system, we expect minimal confounding by indication. Second, the number of patients in the early RA group, especially the number of men, was small and the results should be interpreted with caution. Third, by the end of the 4-year followup period, about 80% of patients had missing datapoints at one or more followup visits. However, there was no apparent sex bias in disease activity among the men and women with missing data, and the missing data appeared with similar frequencies among men and women.
Our results corroborate previous findings that men respond better to treatment than women in early RA, and provide novel evidence that such sex differences are observed in early but not established RA. Thus, if sex differences in treatment responses become apparent only when treatment is administered in early stages of the disease, then perhaps all studies comparing responses to treatment over time between men and women should take into consideration the duration of the disease at the time that treatment is initiated. Our results further demonstrate that when a cohort of patients with established RA is adjusted for confounders and for accumulated sex differences in various disease features present at the start of followup, no sex difference is expected to remain during followup. Hence, using cohorts of patients with varying RA durations at initiation of therapy is not recommended when the aim is to study sex differences in treatment responses.
Acknowledgment
We thank our collaborators from the rheumatology departments in the following hospitals in Denmark for contributing data from their patients with RA to the DANBIO Registry: Ålborg, Århus, Esbjerg, Frederiksberg, Gentofte, Glostrup, Gråsten, Hjørring, Holbæk, Holstebro, Horsens, Hørsholm, Kolding, Næstved/Nykøbing Falster, Odense, Randers, Rigshospitalet, Roskilde/Køge, Silkeborg, Slagelse, Svendborg/Fåborg, Vejle, and Viborg. We thank Niels Steen Krogh for assistance with extracting DANBIO data. We also thank Dr. Ginny Gildengorin at the Children’s Hospital Oakland Research Institute for statistical advice.
Footnotes
-
Dr. Jawaheer is supported by a Career Development Award (K01AR053496) from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. The DANBIO Registry is supported by the hospital owners and by grants from Abbott, Bristol-Meyers Squibb, Roche, Schering-Plough/MSD, UCB-Nordic, and Wyeth/Pfizer.
- Accepted for publication August 12, 2011.








{kind=link}
{kind=link}
{kind=link}