

To the Editor:
Ehlers-Danlos syndrome (EDS) type IV is an autosomal dominant disorder caused by mutations in the gene for type III procollagen (COL3A1). The phenotype is characterized by thin translucent skin with visible veins, spontaneous rupture of arteries, uterus or intestines, characteristic facial features, and easy bruising1. Median survival is 48 years, with spontaneous arterial rupture the commonest cause of death2. We describe a case of renal infarction due to spontaneous renal artery dissection in EDS, highlighting the clinical presentation and management difficulties.
A 25-year-old man presented to an outlying facility in our hospital network with a 6-h history of acute severe right flank pain associated with 2 episodes of vomiting. Medical history was notable for a diagnosis of EDS type IV, diagnosed by dermal fibroblast culture at the age of 20 years. He dislocated his left shoulder at the age of 21 years and had a pneumothorax at age 22 years. His mother and brother had also been diagnosed with EDS type IV. He was a nonsmoker and denied cocaine use. Examination revealed the characteristic facies of his condition: translucent skin with visible veins, multiple intradermal pressure-point bruising, and mild hypermobility. Abdominal examination revealed tenderness in the right iliac fossa without guarding or rebound tenderness. Laboratory tests showed an elevated white blood cell count at 13.1 × 109/l, with neutrophilia 11.2 × 109/l. C-reactive protein was 8.5 mg/l. Hematology and biochemistry were otherwise normal. Autoantibody and thrombophilia screens were normal, as were chest radiograph, electrocardiogram, transthoracic echocardiogram, and urinalysis. Computed tomography of the abdomen demonstrated multiple areas of renal infarction in the right kidney, predominantly in the lower pole but also involving the upper pole. Cortical involvement was estimated at 30%. Dimercaptosuccinic acid scan demonstrated minimal if any uptake in the lower pole of the right kidney, with faint uptake in the upper pole. Relative uptake was estimated at 23% for the right kidney and 77% for the left kidney. Magnetic resonance angiogram confirmed the renal infarctions (Figure 1A) and demonstrated right renal artery dissection (Figure 1B, Figure 2). Initial treatment consisted of analgesia, intravenous antibiotics, and unfractionated heparin. Following transfer to our center, anticoagulation was stopped. His pain decreased somewhat and he had no further vomiting. He was subsequently transferred back to his local hospital.

Coronal magnetic resonance renal angiogram demonstrating nonenhancing renal parenchymal infarcts (A, arrows) and right renal artery dissection (B, arrow).
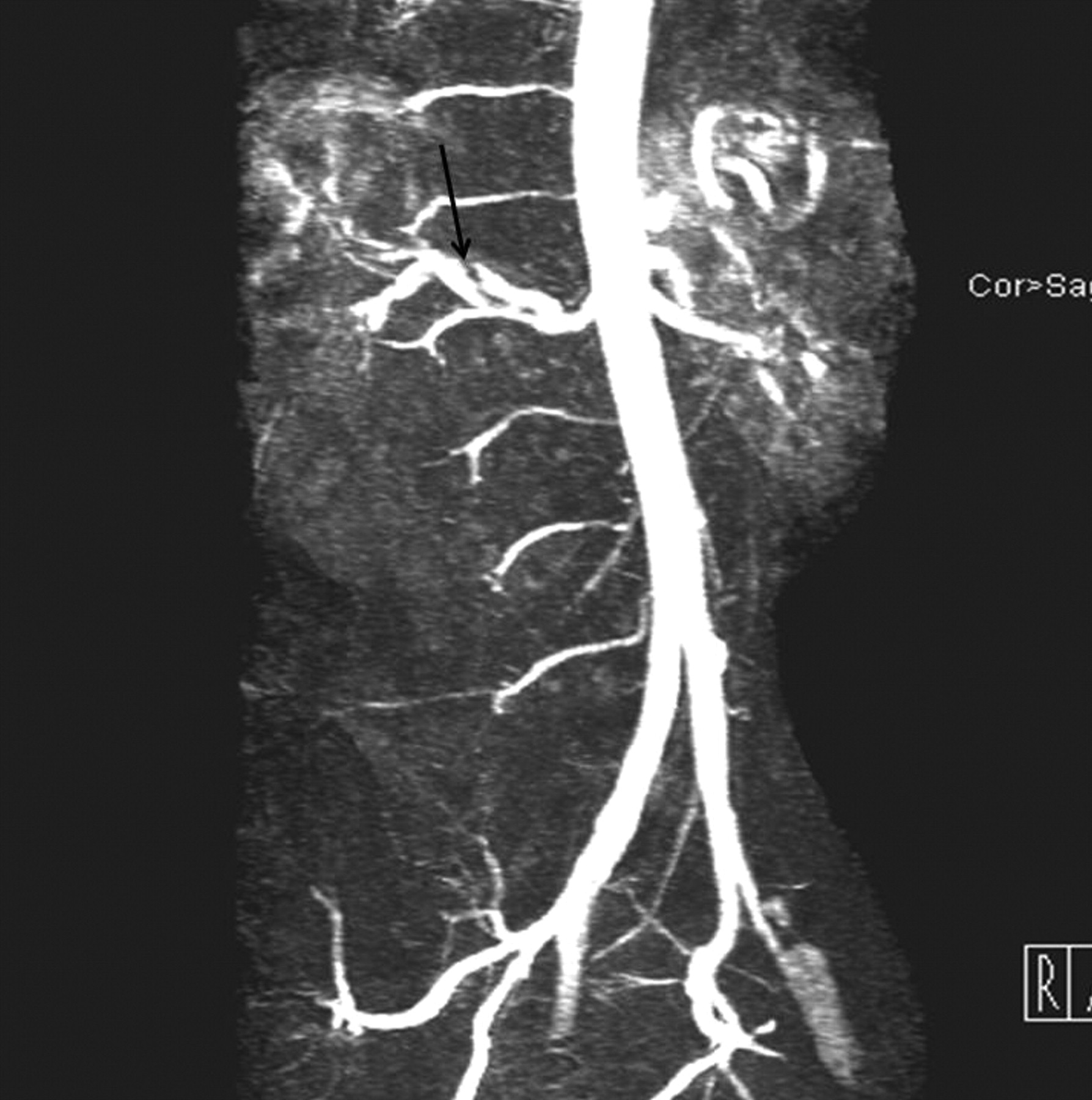
Magnetic resonance imaging abdominal aortic angiogram showing right renal artery dissection (arrow).
EDS is an inherited disorder of connective tissue caused by defective collagen production. Several subtypes are recognized today, including type IV. The friability of the vasculature in type IV EDS commonly results in arterial dissection or spontaneous arterial rupture. Infarction is a rare complication. Two previous cases of EDS associated with renal infarction have been reported. Yigal, et al, described a patient who presented with right thromboembolic renal infarctions due to a right renal artery aneurysm that was managed conservatively3. Gelbmann, et al described the case of a young woman who presented with renal infarction associated with spontaneous rupture of the liver and pneumothorax4. An additional case in the French language literature described a woman who had renal artery dissection in pregnancy5. The management of renal infarction is dependent on the etiology. Anticoagulation is indicated in cases resulting from cardioembolic sources6. Management of renal artery dissection resulting in renal infarction is controversial, with conservative management, anticoagulation, and surgical and endovascular revascularization, as described7. The use of both unfractionated and low molecular weight heparins is associated with an increased risk of hemorrhagic complications8,9. The use of anticoagulation in EDS type IV may increase the risk of fatal hemorrhage unrelated to the thrombotic presentation. In the absence of randomized controlled trial data in this rare complication of a rare disease, we advocate treatment decisions on a case by case basis. In cases of non-life-threatening thromboembolic disease, the risks may outweigh the benefits of anticoagulation in both the short and long terms.
Our case demonstrates a rare cause of renal infarction, which should be added to the differential diagnosis. To our knowledge this is the first report of a case of renal artery dissection presenting with renal infarction in EDS. The optimum management of renal infarction in Ehlers-Danlos syndrome type IV remains to be determined.
Footnotes
-
Dr. Conway reports receiving research funding from Roche Ireland Limited and UCB (Pharma) Ireland Ltd, and honoraria from Merck.








{kind=link}
{kind=link}