

To the Editor:
Giant cell arteritis (GCA) is the most common idiopathic systemic vasculitis of large vessels. It affects individuals over 50 years of age. The prevalence is approximately 200 per 100,000 persons1. Although it may be generalized, vessel inflammation most frequently involves the muscular arteries originating from the aortic arch and their branches and usually presents with new-onset or worsened headache, jaw claudication, scalp or temporal artery tenderness with decreased pulsation, or visual symptoms such as eye pain, amaurosis fugax, diplopia and visual loss. High-dose corticosteroid (CS) therapy, which may last 1 to 5 years, is the basic treatment for GCA. However, in about 60% of patients the long duration of treatment causes serious, dose-related side effects2. For patients whose disease is resistant to or dependent on CS therapy, methotrexate (MTX) or azathioprine (AZA) is used as steroid-sparing second-line treatment, with conflicting results3. While MTX seems to be effective in controlling GCA4,5, the data on AZA remain controversial6; the tumor necrosis factor-blocking agents infliximab and etanercept were not successful in inducing and maintaining disease remission7,8.
Interleukin 6 (IL-6) plays an important role in the pathogenesis of GCA. IL-6 levels are elevated in active disease, correlate with the acute-phase response (such as C-reactive protein; CRP), and remain higher in patients who have experienced more relapsing disease9.
We describe 2 patients with refractory biopsy-proven GCA who were at high risk for longlasting high-dose CS, and who were treated successfully with the humanized anti-IL-6 receptor (IL-6R) antibody tocilizumab (TCZ), given monthly at a dose of 8 mg/kg.
Our 2 female patients (aged 76 and 77 years old) had a clinical history of diabetes mellitus with oral therapy (metformin) and hypertension needing at least 2 antihypertensive drugs. Additionally, they had osteoporosis (T scores −3.1 and −2.8 on dual energy x-ray absorptiometry). Patient 1 was previously treated with high-dose steroids for 14 months (up to 75 mg/day of prednisone) and subsequently with associated MTX (20 mg weekly dose, intramuscularly). MTX failed to allow a steroid-sparing target as signs and symptoms of relapsing GCA presented when prednisone dose was reduced to less than 25 mg/day.
Apart from the noted comorbidities, a reduction of steroid dose was largely desirable in Patient 2 because in 2010 she underwent 2 orthopedic interventions for right hip replacement due to aseptic necrosis attributed to CS treatment, when she was still taking 25 mg/day of oral prednisone and 20 mg/week of intramuscular MTX.
The patients were followed at our center from August 2010 for TCZ treatment for a mean period of 7 months (6 and 8 months, respectively). The acute-phase responses (erythrocyte sedimentation rate and CRP) decreased rapidly after the first TCZ infusion, and were completely normal in both patients after 3 months of treatment (Figure 1).
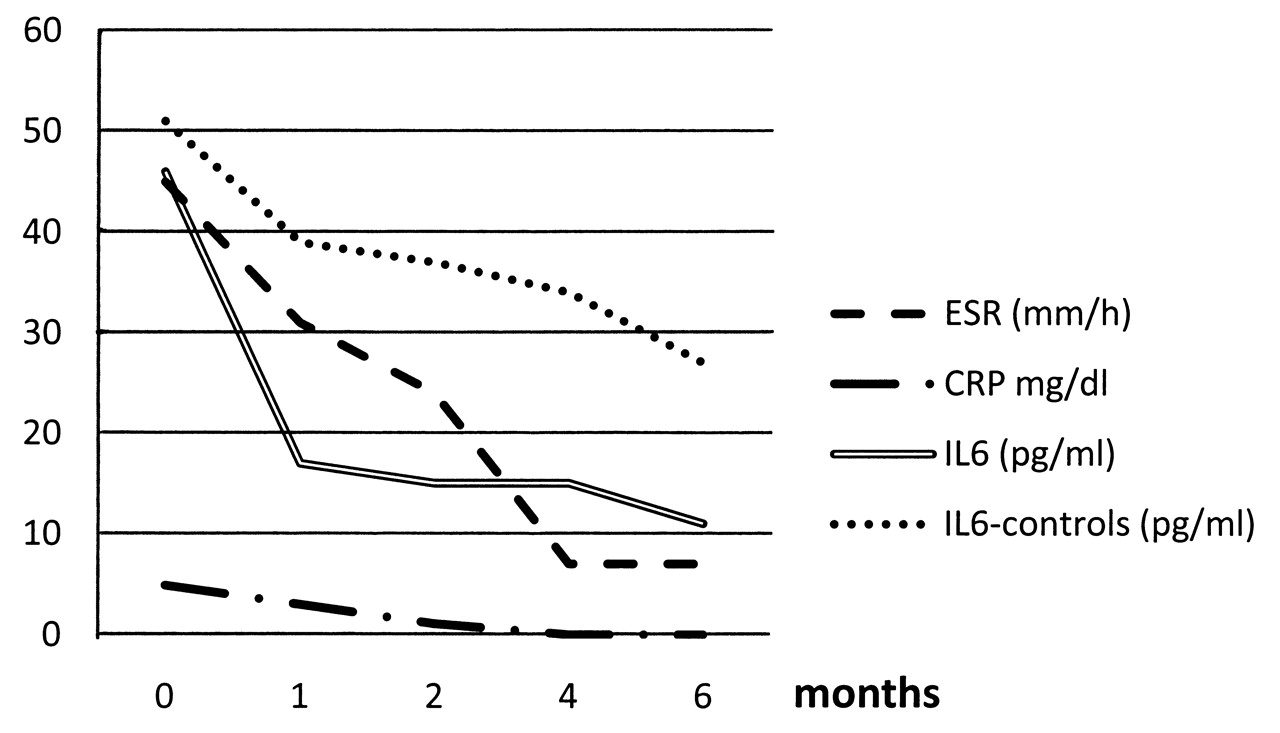
Serologic assessment of the 2 patients treated with TCZ during the followup.
Circulating levels of IL-6 were measured by immunoassay using Quantikine kits (R&D Systems), according to the manufacturer’s instructions. Four patients with recently diagnosed GCA (duration not more than 2 months), treated with CS according to the current guidelines10, were enrolled as a control group to compare serum levels of IL-6. The serum level of IL-6 decreased more rapidly in the 2 GCA patients treated with TCZ compared to the controls. Mean baseline values were 46 pg/ml and 51 pg/ml, respectively; then 17 pg/ml and 39 pg/ml after 2 months; and 11 pg/ml and 27 pg/ml after 6 months (p = 0.04; Figure 1). Of note, after 2 months the starting dose of prednisone was halved, and then reduced to the maintenance dose of 5 mg/day. We based our definition of disease activity on clinical and serologic indicators. At a mean followup of 7 months both the patients were in remission and inflammation markers were within the normal range.
TCZ has been proposed as a safe and effective treatment for cases of large-vessel vasculitis, that is, for Takayasu arteritis11 and GCA12. In our experience the additional clinical benefit of treatment with TCZ was its CS- and immunosuppressant-sparing effect without disease flare. Indeed, the rapid remission with TCZ treatment allowed early reduction of daily CS even in patients who were CS-dependent. Current data derived from randomized controlled clinical trials in rheumatoid arthritis suggest an acceptable tolerability profile for TCZ, and longterm exposure to TCZ during open-label extension studies did not reveal any new safety signals or increased risks of serious adverse events13.
TCZ may be considered a steroid-sparing agent in patients with GCA, but before results of controlled trials become available, it may be considered as a therapeutic option for patients who do not improve or stabilize with conventional therapy or in subjects in whom a reduction of steroid dose is largely desirable.








{kind=link}