

Abstract
Objective. The aim of this multireader exercise was to assess the reliability and sensitivity to change of the psoriatic arthritis magnetic resonance imaging score (PsAMRIS) in PsA patients followed for 1 year.
Methods. MRI was acquired from 12 patients with PsA before initiation of treatment and after 12 months. MR images were scored according to PsAMRIS (for synovitis, tenosynovitis, periarticular inflammation, bone marrow edema, bone erosion, and bone proliferation) under standardized conditions, in unknown chronological order. Intraobserver/interobserver reliability was examined by intraclass correlation coefficients (ICC) and sensitivity to change by standardized response means (SRM).
Results. The interobserver reliability of PsAMRIS was high for synovitis, tenosynovitis, periarticular inflammation, and bone edema status and change scores (interobserver ICC 0.87–0.97). The intraobserver reliability was moderate to high (ICC 0.60–0.98) for status and change scores, except for change in periarticular inflammation (ICC 0.33). PsAMRIS sensitivity to change was moderate for synovitis, tenosynovitis, and periarticular inflammation (SRM 0.5–0.8), while poor (SRM 0.1–0.3) for bone marrow edema, erosion, and bone proliferation. Rare occurrence and minimal change contributed to poor SRM and change-score ICC for bone parameters.
Conclusion. This multireader exercise, performed under standardized conditions, confirmed PsAMRIS to have high interobserver and intraobserver reliability for hand PsA. Measures of inflammation were sensitive to change, implying that PsAMRIS may be a valuable tool for monitoring change in inflammation during PsA clinical trials.
Psoriatic arthritis (PsA) is a heterogeneous disease with diverse presentations and disease outcomes. During the last decade, new biological therapies for PsA have been introduced, with the potential to modify the disease course and suppress both joint inflammation and erosive bone damage. This has led to a need to develop reliable and responsive outcome measures, so that treatment effects can be monitored accurately. Magnetic resonance imaging (MRI) has the advantage of depicting both soft tissue inflammation, affecting articular and periarticular structures, and bone involvement (including bone marrow edema, erosion, and proliferation). In rheumatoid arthritis (RA), the MRI score (RAMRIS) developed by Outcome Measures in Rheumatology Clinical Trials (OMERACT) has been shown to be both reliable and responsive to change in multiple patient groups1,2,3,4,5. In 2004, an OMERACT MRI working party began to develop a PsA MRI scoring system (PsAMRIS)6,7. This has been shown in previous exercises to demonstrate moderate to good interreader reliability6,7,8. The aim of the current multireader exercise was to test inter- and intrareader reliability of PsAMRIS in a group of patients on anti-tumor necrosis factor-α (TNF-α) therapy or standard disease modifying antirheumatic drugs (DMARD) over a 1-year period. Both status and change scores have been recorded under standardized conditions. This allows determination of whether PsAMRIS can be used as an instrument to monitor responses to therapy in PsA.
MATERIALS AND METHODS
Patients
The exercise was performed using MRI scans acquired from 12 patients with PsA (8 from Copenhagen and 4 from Leeds) before the onset of treatment and after 12 months (Table 1). Patient characteristics were as follows: 58% were women, median age was 56.5 years (range 35.0–72.0) and disease duration 4.0 years (range 0.6–11.0). The 8 patients from Copenhagen received anti-TNF-α treatment and the 4 Leeds patients DMARD.
Patients included in the Psoriatic Arthritis Magnetic Resonance Imaging Score (PsAMRIS) workshop.
Methods
The MRI scans included images of the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints of the 2nd–5th fingers. The images were acquired using a 0.6 T Philips Panorama MRI unit (Copenhagen) and a 0.2 T Esaote C Scan MRI unit (Leeds). The acquired images from Copenhagen consisted of sagittal and axial STIR sequences, and coronal, axial, and sagittal T1-weighted before and after intravenous administration of gadolinium. From Leeds, T1-weighted axial, sagittal, and coronal images without gadolinium injection were available. For the workshop all images were anonymized and blinded for time sequence; for second reading, images were re-anonymized and re-randomized. FG, FMcQ, MØ, and P. Bøyesen read MR images of the 12 patients twice on identical PACS workstations. The images were scored according to the PsAMRIS system as described6,8. In short, for each MCP, PIP, and DIP joint-level synovitis is scored 0–3, tenosynovitis 0–3, periarticular inflammation 0–2, bone marrow edema 0–6, bone proliferation 0–1, and bone erosions 0–20.
Statistics
Baseline and 1-year change of the PsAMRIS features were analyzed as median (minimum, maximum) of the 4 readers’ median scores. Changes in PsAMRIS features within patients were tested by Wilcoxon signed-rank tests. Reliability was evaluated by 2-way mixed intraclass correlation coefficients (ICC), smallest detectable difference (SDD), and the smallest detectable change (SDC) for status and change scores, respectively. Average measure ICC (ICCa) was used for interreader reliability and single-measures ICC (ICCs) for intrareader reliability. Bland and Altman’s 95% limits of agreement method was used to estimate the SDD and SDC9,10.
Specifically, we used the random-effects average of the mean residual error of repeated-measures analysis of variance by √2 of the number of readers (√k). A SDD%max and SDC%max were expressed as the SDD/SDC divided by the maximum observed scores10. The PsAMRIS’s sensitivity to change was estimated by the standardized response mean (SRM). The SRM was calculated as the mean change divided by the standard deviation of the change score.
RESULTS
The median (range) PsAMRIS results at baseline and 1-year followup are summarized in Table 2. Synovitis, tenosynovitis, and periarticular inflammation were frequently detected in this group of patients with PsA, whereas bone marrow edema and erosions were infrequent. At 1-year followup, tenosynovitis (p = 0.05) statistically significantly improved, and there was a numerical, but not statistically significant, improvement in PsAMRIS synovitis and periarticular inflammation. PsAMRIS bone marrow edema, erosions, and bone proliferation did not change during the 1-year followup period.
Median (minimum, maximum) baseline and 1-year change in PsAMRIS features for overall scores and subjoint regions. All values are given as median (minimum to maximum) of the 4 scorers’ median scores.
The inter- and intrareader reliability of PsAMRIS status and change scores is summarized in Table 3⇓. Overall, the PsAMRIS reliability was good to very good, with some exceptions. The 1-year change in PsAMRIS bone proliferation and bone erosions had poor to trivial reliability (ICCa 0.10 and 0.44, respectively). All readers, however, consistently found minimal or no change in these parameters.
Inter- and intrareader reliability for PsAMRIS status and change scores. Intraclass correlation coefficients. Key to SRM values: Very good, ICC ≥ 0.80; good, 0.50 ≤ ICC < 0.80; poor, 0.20 ≤ ICC < 0.50; trivial, ICC < 0.20.
Inter- and intrareader reliability for PsAMRIS status and change scores. Smallest detectable difference and change.
The PsAMRIS’s sensitivity to change assessed by SRM is summarized in Table 4. Overall, there was moderate responsiveness of synovitis, flexor tenosynovitis, and periarticluar inflammation measured by PsAMRIS (SRM 0.5–0.8). However, bone marrow edema, erosion, and bone proliferation showed poor sensitivity to change in this exercise (SRM 0.1–0.3). PsAMRIS’s sensitivity to change during anti-TNF-α therapy is illustrated in Figure 1.
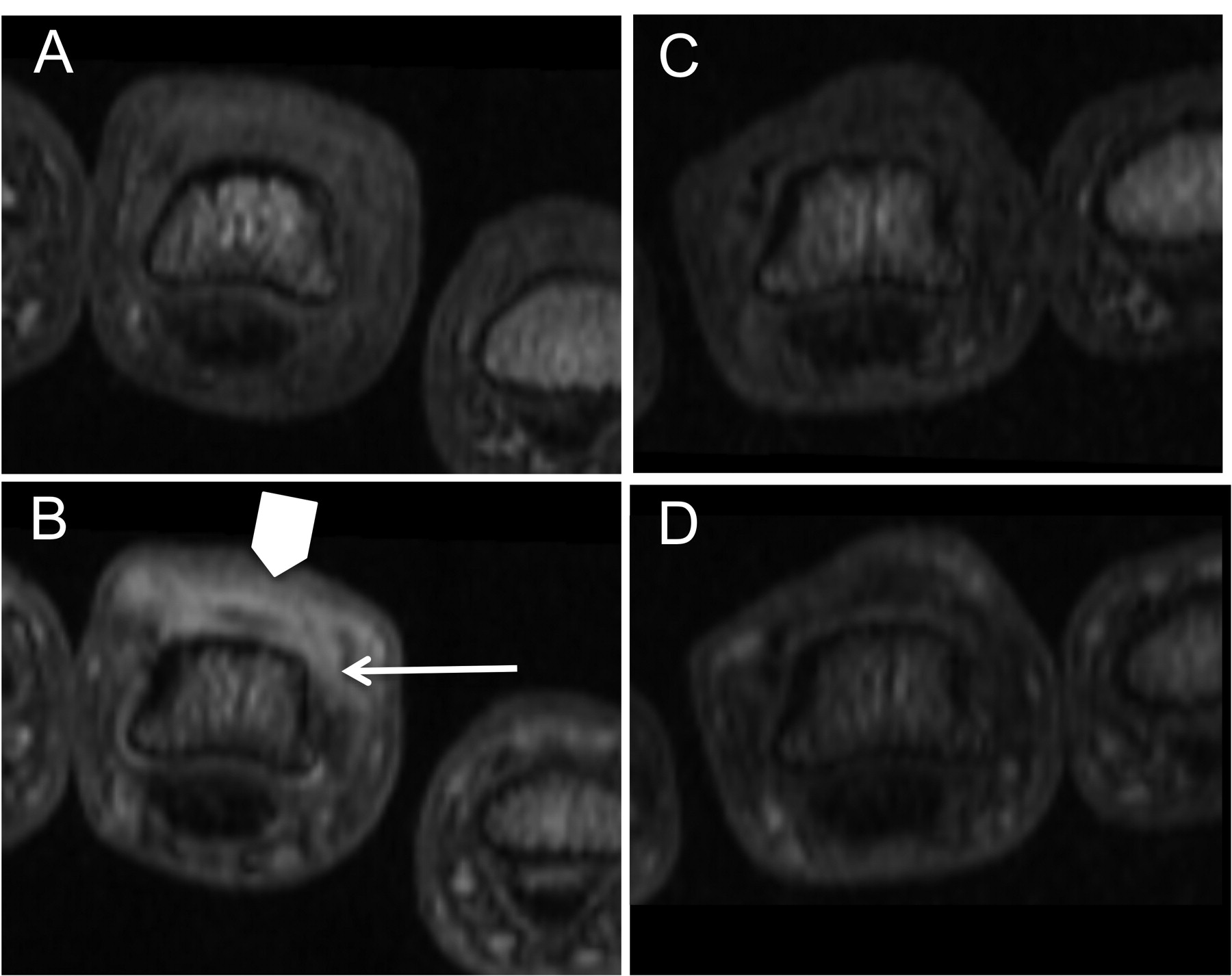
Magnetic resonance imaging examples of PsAMRIS’s sensitivity to change during anti-TNF-α treatment. The T1-weighted images show before (A and B) and after (C and D) gadolinium injection. Baseline MR images of PIP-3 (A and B) show periarticular inflammation (broad arrow, B) and synovitis (narrow arrow, B). After 12 months with anti-TNF-α treatment (C and D) the periarticular inflammation and synovitis of the PIP-3 resolved.
Sensitivity to change of the PsAMRIS measured by standardized response means (SRM). Key to SRM values: large, SRM ≥ 0.80; moderate, 0.50 ≤ SRM < 0.80; small, 0.20 ≤ SRM < 0.50; trivial, SRM < 0.20.
DISCUSSION
In this multireader exercise, the PsAMRIS was tested under standardized conditions with identical radiological workstations and image setup, in addition to the stringent methodology with blinded chronology of scans applied in previous exercises8. The previously demonstrated good to very good reliability was reproduced8. Further, PsAMRIS was sensitive to improvement in inflammation scores of synovitis, flexor tenosynovitis, and periarticular inflammation during anti-TNF-α therapy.
In this multireader exercise all PsAMRIS features could be scored in 8 of 12 included patients, all of whom received anti-TNF-α therapy (Copenhagen). PsAMRIS bone erosions and bone proliferation were the only features that could be scored in the remaining 4 DMARD-treated patients (Leeds). As a consequence, all results concerning PsAMRIS synovitis, flexor tenosynovitis, periarticular inflammation, and bone marrow edema are derived from patients treated with anti-TNF-α therapy.
Intrareader reliability for PsAMRIS was examined for the first time in this exercise and was overall “good” to “very good” (0.5 to 1.0). The reliability of PsAMRIS synovitis, bone marrow edema, and erosion scores was comparable with the high reliability for the same components of the RAMRIS when tested in patients with RA1. However, the results for the PsA-specific features of periarticular inflammation and bone proliferation were more variable. This may reflect difficulty in readers recognizing and scoring these features, which could be addressed by further training. The intrareader reliability for PsAMRIS change scores was also generally “good” to “very good.” Interreader reliability for PsAMRIS status scores was “good” to “very good” and was better than in previous PsAMRIS exercises8. This was also true for the reliability of change scores, with the exception of PsAMRIS bone erosion and bone proliferation, where the ICC were reduced due to the lack of change during the 1-year followup, and not to any major disagreements between readers11. Other studies in larger and more heterogeneous PsA populations, where more change in bone parameters occurred, would be needed to investigate the responsiveness of these features.
During the 1-year followup tenosynovitis improved and we found a numerical but not statistically significant improvement in PsAMRIS synovitis and periarticular inflammation. The SRM was used to measure responsiveness, as done previously in similar settings2. PsAMRIS synovitis, flexor tenosynovitis, and periarticular inflammation were moderately (0.5 to 0.8) sensitive to change, but for bone edema, sensitivity to change was lower (SRM −0.34). A possible explanation of this result was that the bone edema score was high in only one patient, whereas the remaining patients had either mild (score 1) or no bone edema, making it difficult for an improvement to be observed. PsAMRIS bone erosion and bone proliferation were not responsive to change. This was caused by the minimal change that occurred in accordance with the potent influence of anti-TNF-α therapy on bone, not by major disagreements between readers.
A limitation of the study was the small sample size. Further, the external validity of the results could be questioned. The PsA patients studied here all had involvement of the fingers but in patients with, for example, oligoarticular large-joint disease, PsAMRIS may not capture relevant pathology or its change in the setting of a randomized controlled trial. Therefore, the applicability of this scoring system to a more heterogeneous group of PsA patients remains to be examined.
In summary, this multireader exercise performed under standardized conditions has confirmed PsAMRIS to have high interobserver and intraobserver reliability for hand PsA. The MRI measures of inflammation were sensitive to change, implying that PsAMRIS may be a valuable tool for monitoring change in inflammation during PsA clinical trials.








{kind=link}