

Abstract
Objective. To investigate by magnetic resonance imaging (MRI) which bones in wrists and metacarpophalangeal (MCP) joints most frequently show bone erosions, and which most frequently demonstrate erosive progression, in early and established rheumatoid arthritis (RA).
Methods. MRI datasets from 258 RA patients [126 with early RA (disease duration < 6 months)] were analyzed, of whom 223, including 126 with early RA, had 1-year followup MRI. All patients had MRI of one wrist, whereas 86 patients had additional images of 2nd–5th MCP joints, and 46 patients additional images of the contralateral wrist. MRI were evaluated blinded by one reader, according to the OMERACT RA MRI scoring system (RAMRIS) for erosions, and presence/absence of erosions was noted in each bone, as was presence/absence of erosive progression.
Results. The capitate, ulna, lunate, triquetrum, and scaphoid were the 5 bones with both most frequent baseline erosions and most frequently demonstrated erosive progression. No bones were without erosions. Patterns of erosions and progression were similar in early and established RA. No major difference between dominant and nondominant wrists was detected. In the fingers, the 2nd–3rd MCP joint most frequently displayed erosions and erosive progression.
Conclusion. The distribution and frequency of bone erosion and erosive progression as detected by MRI in RA wrists and MCP joints were identified. No pattern differences between early versus established disease and dominant versus nondominant sides were detected. No bones showed erosive progression. Thus, no self-evident simplification of the RAMRIS erosion score was identified. Bone involvement patterns may be considered, when joints are selected for MRI protocols for clinical trials and practice.
Magnetic resonance imaging (MRI) has been shown to be more sensitive for identifying early bone damage than conventional radiography1,2,3,4, and is increasingly used as an outcome measure of structural joint damage in rheumatoid arthritis (RA) clinical trials5,6,7,8. MRI of unilateral wrist and 2nd–5th metacarpophalangeal (MCP) joints is more sensitive to change for erosive progression than radiography of both hands, wrists and forefeet9. However, data on the exact distribution of bone erosions, i.e., the pattern of bone involvement, are minimal.
The aim of this study was to investigate which bones in wrists and MCP joints most frequently show bone erosions and which most frequently demonstrate erosive progression in early and established RA.
MATERIALS AND METHODS
MRI datasets from 258 RA patients [126 with early RA (disease duration < 6 months)] were analyzed. One-year followup MRI were available in 223 patients (126 with early RA). All patients had MRI of one wrist, whereas 86 had additional MCP joint MR images and 46 additional images of the contralateral wrist. The MRI data originated from 5 investigator-initiated clinical studies9,10,11,12,13,14, in which details on population characteristics and MRI techniques are described.
MRI (including T1-weighted images in coronal and axial planes) were evaluated for bone erosions according to the OMERACT RA MRI scoring system (RAMRIS), i.e., an erosion was defined as a sharply marginated bone lesion, with correct juxtaarticular localization and typical signal characteristics, visible in 2 planes, with a cortical break seen in at least one plane5.
Presence/absence of erosions at baseline was noted in each bone, as was presence/absence of erosive progression. All images were read blinded by the same reader (BE), who has extensive experience in reading MRI of RA patients and has demonstrated high levels of intra- and interobserver reproducibility6,9.
RESULTS
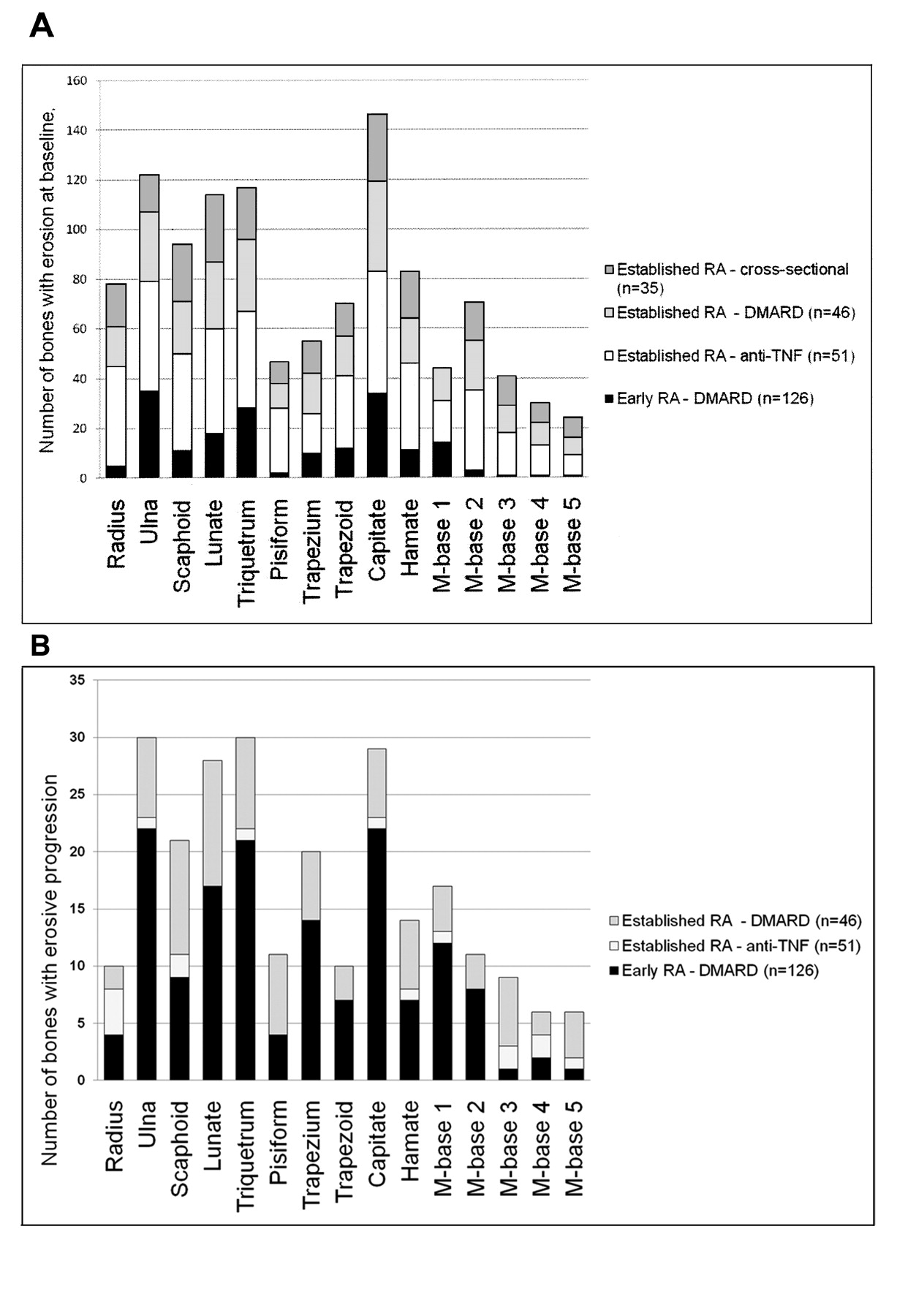
The distribution of baseline erosions per wrist bone is shown in Figure 1A, whereas the distribution of bones with progression at Year 1 is seen in Figure 1B. The capitate, ulna, lunate, triquetrum, and scaphoid were the 5 bones most frequently demonstrating both baseline erosions and erosive progression. Patterns were similar in early and in established RA. No bones were without erosions. In patients with available bilateral wrist MRI, no major differences between dominant and nondominant hands were found (269 vs 277 bones with baseline erosions; 73 vs 85 bones with erosive progression).
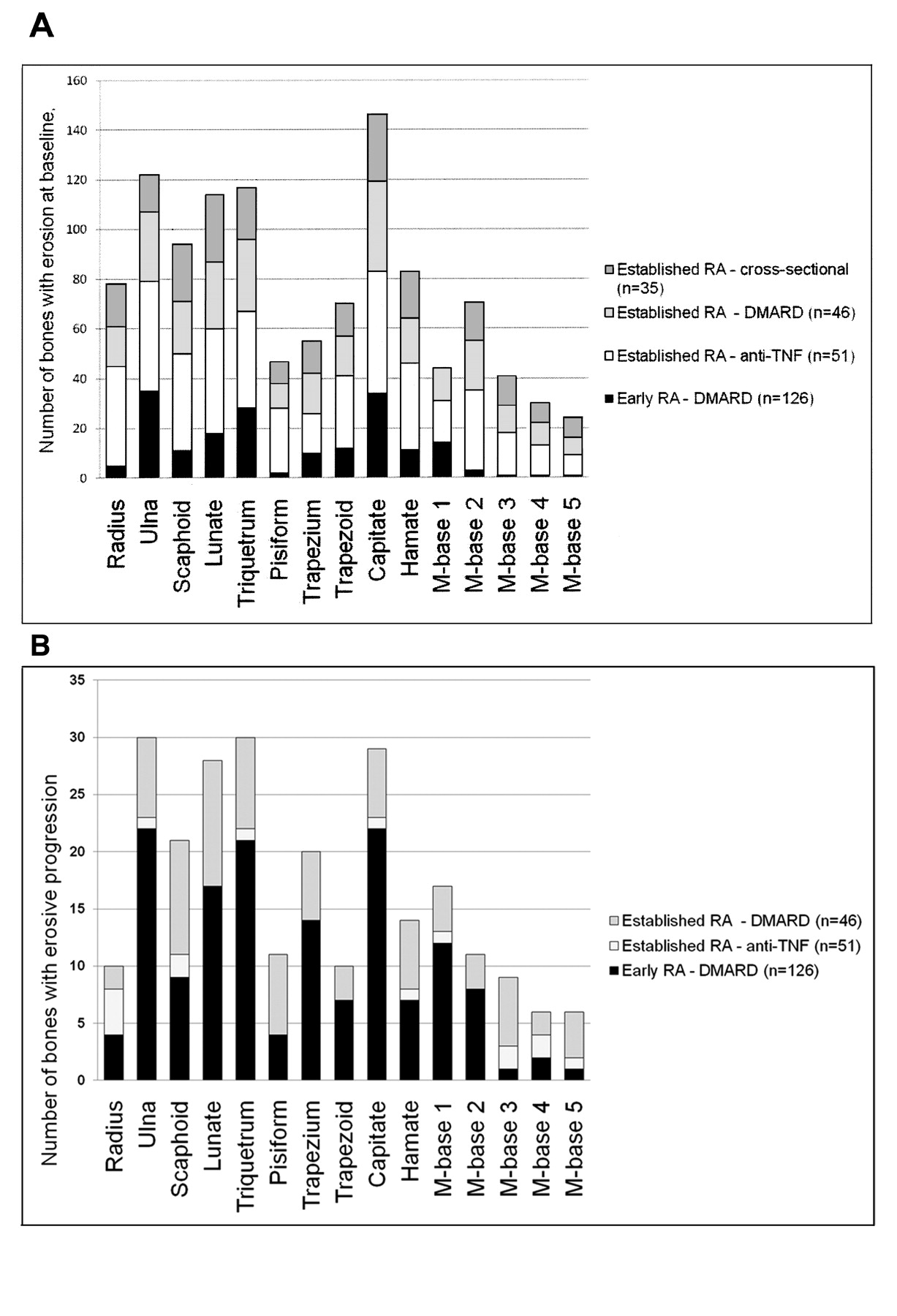
A. Number of bones with bone erosion, per bone (n = 258). B. Number of bones with erosive progression, per bone (n = 233).
In the patients in whom both wrist and MCP joint images were available, baseline erosions were still most frequently found in the 5 previously mentioned wrist bones, whereas the head of the 2nd metacarpal bone was the most frequently involved MCP joint bone. Second and 3rd MCP joints most frequently showed erosive progression.
DISCUSSION
Our study documents the frequency and distribution of the presence and progression of MRI bone erosions in a large number of RA patients from different populations. Based on data from 258 RA patients, patterns of MRI bone erosion in wrists and MCP joints could be identified. The capitate, ulna, lunate, triquetrum, and scaphoid were most frequently involved and showed, together with the 2nd and 3rd MCP joints, the most change over time. No obvious differences in erosive patterns between early and established RA, or between dominant and nondominant wrists, were identified.
The images were obtained and scored in agreement with the OMERACT RAMRIS. This method has been extensively validated and is now the standard MRI method in RA clinical trials5,6,7,8. Comparisons with computed tomography as a “gold standard” reference for bony destruction have demonstrated a very high level of agreement and, consequently, confirmed that MRI bone erosions are true erosions15,16,17. MRI has been documented to be more sensitive to change in erosive joint damage than radiography of both hands, wrists, and forefeet, as evaluated by the Sharp-van der Heijde method8,9. The present study did not include assessment of interobserver reliability, but all images were read by the same experienced reader (BE).
This MRI study of 258 RA patients demonstrated the distribution of erosions and erosive progression in wrist and MCP joints. No pattern differences between early versus established disease and dominant versus nondominant sides were detected. No bones ever showed erosive progression. Thus, no evident reductions in the number of bones to be assessed for erosions could be identified. Future studies should test whether the RAMRIS erosion score can be simplfied to include only the most frequently involved areas (capitate, ulna, lunate, triquetrum, and scaphoid and the 2nd–3rd MCP joint) without losing sensitivity to change. Bone involvement patterns may be considered when joints are selected for MRI protocols for clinical trials and practice.
Acknowledgment
Physicians, study nurses, and patients who took part in the RA cohorts are acknowledged for their contributions.








{kind=link}