

Abstract
Leading up to the Outcome Measures in Rheumatology (OMERACT) 10 meeting, the goal of the Worker Productivity Special Interest Group (WP-SIG) was to make progress on 3 key issues that relate to the application and interpretation of worker productivity outcomes in arthritis: (1) to review existing conceptual frameworks to help consolidate our intended target and scope of measurement; (2) to examine the methodologic issues associated with our goal of combining multiple indicators of worker productivity loss (e.g., absenteeism <—> presenteeism) into a single comprehensive outcome; and (3) to examine the relevant contextual factors of work and potential implications for the interpretation of scores derived from existing outcome measures. Progress was made on all 3 issues at OMERACT 10. We identified 3 theoretical frameworks that offered unique but converging perspectives on worker productivity loss and/or work disability to provide guidance with classification, selection, and future recommendation of outcomes. Several measurement and analytic approaches to combine absenteeism and presenteeism outcomes were proposed, and the need for further validation of such approaches was also recognized. Finally, participants at the WP-SIG were engaged to brainstorm and provide preliminary endorsements to support key contextual factors of worker productivity through an anonymous “dot voting” exercise. A total of 24 specific factors were identified, with 16 receiving ≥ 1 vote among members, reflecting highly diverse views on specific factors that were considered most important. Moving forward, further progress on these issues remains a priority to help inform the best application of worker productivity outcomes in arthritis research.
At the Outcome Measures in Rheumatology Clinical Trials (OMERACT) 9 meeting we provided an update on the 21 available measures that assess the impact of health on work, and the available OMERACT filter evidence in either arthritis or other musculoskeletal disorders1. Recent studies and reviews have shown an increasing interest to assess the impact of arthritis on work from different perspectives1,2,3,4,5. For example, some measures are designed to assess impacts on worker productivity6,7,8,9, by quantifying or monetizing losses in work time or output associated with health-related work absences (absenteeism), as well as reduced performance at work in terms of both quantity and quality (presenteeism). This perspective is considered most relevant in health economics research10,11. Other measures are intended to provide a more clinical or disability-oriented perspective of the impact of health on work12,13,14,15, for example, by assessing the degree of difficulty associated with the performance of specific work-related tasks13. Recent studies have shown only weak-to-moderate associations between productivity- and disability-oriented type instruments2,16, thus differences in conceptual foci among available tools remain important to recognize.
The choice of measure(s) to be considered for recommendation is currently being guided by the availability of OMERACT filter evidence17, including head-to-head comparisons across tools2,10,16,18,19,20,21. At OMERACT 9, we had identified 6 measures7,13,14,22,23,24 as the most promising candidates to continue our work forward, and had received endorsement at the OMERACT plenary session for an updated definition of absenteeism that includes an expanded set of indicators1. Since that time, we have held 3 meetings (EULAR, 2009; Vancouver, 2009; Paris, 2010) that have served the OMERACT agenda, and as well have initiated a new collaborative group (I-CAN-WORK Alliance) in the area of arthritis and work. Leading up to OMERACT 10, the main objective of the Worker Productivity Special Interest Group (WP-SIG) was to examine issues related to the interpretation of numeric scores on our candidate outcomes, rather than the choice of instruments itself. We were challenged to make progress on 3 issues: (1) to reexamine and consolidate our intended measurement target by reviewing pertinent theoretical frameworks; (2) to examine methodologic issues associated with the goal of capturing both absenteeism and presenteeism with a single comprehensive outcome; and (3) to examine the contextual nature of work and its implications for the interpretation of scores derived from our outcomes. The purpose of this article is to describe our progress along each of these objectives.
GUIDING THEORETICAL FRAMEWORKS
Measurement must include a solid theoretical framework — one that defines the necessary domains to gather a valid picture of the target concept, and posits the theoretical relationships between factors. In recent meetings, we had identified 3 frameworks that were considered most relevant for understanding the scope of our measurement target and the different components of health-related worker productivity loss.
Adaptation of the Model by Brouwer, et al — Transitioning Between Absenteeism and Presenteeism
Theoretical relationships between work productivity loss and health-related quality of life indicators were proposed in a framework by Brouwer, et al25. We adapted this framework at OMERACT 9 to emphasize an important concept — that workers may transition between states of work absenteeism and presenteeism when there is a change in health status1 (Figure 1). This helped us recognize that both absenteeism and presenteeism must be concurrently measured to provide a complete view of the impact of arthritis on work, and that they should also ideally be represented within the same measurement continuum. We believe the lowest level of impact should be represented by a complete absence of both absenteeism and presenteeism (0% productivity loss), while the highest level of impact should be represented by a person not working at all (100% productivity loss). Evidence from recent costing studies has shown both absenteeism and presenteeism to be contributing sources of health-related worker productivity loss11,26, providing empirical support for both components to be measured as “essential” elements that make up our intended target concept. Thus, the ability to integrate workers’ experience of both absenteeism and presenteeism into a single unifying outcome score is imperative for us, as it represents the whole “truth” that we are seeking. Candidate measures should satisfy this requirement.

Adaptation of the conceptual model by Brouwer, et al25, which examines the relationship between an individual’s health state and level of worker productivity over time. The vertical axis depicts a level of functioning and health, or quality of life (“Health Status”). Two thresholds are defined by the job. The first intersection is Q1, defined as the threshold above which the loss of health does not affect functioning on the job. The second intersection, Q2, defines a threshold below which the individual is unable to work. Between Q1 and Q2 represents the range where there is at-work productivity loss (presenteeism), as the individual is at work but is unable to be as productive as the job demands. Reprinted from Beaton, et al. J Rheumatol 2009;36:2100–91.
The contextual nature of worker productivity was also recognized in the original framework by Brouwer, et al25. Two critical thresholds of health status were defined: Q1, above which a person was working without any limitations with a health state exceeding job demands even with mild fluctuations in disease; and Q2, below which persons could not be at work1,25. The area between the 2 (Q1–Q2) represents at-work productivity loss (presenteeism). This framework allowed for Q1 and Q2 to float, so that a job with a different set of demands relative to a health state might allow someone in a given health state to be at work with no limitations. Other contextual factors and personal characteristics that could influence the positions of the Q1 and Q2 thresholds, however, were not explicitly defined in this framework.
ICF Model. Dissociating the Impact of Arthritis on Work
The International Classification of Functioning, Disability and Health (ICF) model27 adheres to the biopsychosocial model of disease and recognizes health impacts at 3 interrelated levels: body functions and structures <—> activities <—> participation. Worker productivity loss is generally considered to be most consistent with restrictions at the participation level, reflecting challenges for a person to fulfill a worker role. All our candidate measures are primarily capturing participation restrictions28, although several are also capturing limitations at the activities level (e.g., lifting, commuting, etc.)13,14,15, or impairments at the level of body functions and structures (e.g., pain, fatigue that relates to work)14,15. The role of contextual factors is integral to the ICF framework and provides the link between arthritis (health) and the resultant impact at the 3 levels. In the ICF, contextual factors are organized as “environmental” or “personal” factors, but they can also be differentiated as fixed “scene setters” or modifiable factors that function as either “barriers” or “enablers,” according to Badley, et al29. Environmental factors may include physical, social, structural, or attitudinal factors such as physical environment at work, workplace and health policies, attitudes towards injury, and relationships and roles27,30. Personal factors refer to individual characteristics and living background such as age, gender, attitudes and beliefs, ability to cope, socioeconomic status, and also role expectations. According to the ICF, the level of disability experienced by a person is a complex interaction of health, person, and environmental factors and needs to be understood within this broader context27.
Sandqvist and Henriksson Framework — the Importance of Person-Environment “Fit”
A conceptual model developed by Sandqvist and Henriksson31 (2004) is another useful perspective on our target concept (Figure 2). This model examines 3 dimensions of work functioning in the context of occupational rehabilitation: individual capacity (physical and psychological attributes), work performance (ability to handle tasks), and work participation (ability to fulfill role of worker)31. These dimensions are proposed to have strong parallels with the 3 ICF levels of health impacts. In its core concept, this model posits that the level of work functioning at each of the 3 dimensions is a function of the degree of “fit” between relevant personal and environmental factors, and that the consequences of specific person-environmental mismatches could cross different dimensions31. A good fit might mean a worker is still experiencing some pain, fatigue, or disability, but favorable environmental factors like having a flexible work schedule, access to assistive equipment, and social support may enable a person to work to her full capacity. Problems occur in situations where there is a significant person-environment mismatch, which could lead to losses in worker productivity. Recent evidence suggests that person-job mismatches are predictive of adverse future work disability outcomes32,33, providing some support for key concepts proposed in this framework.
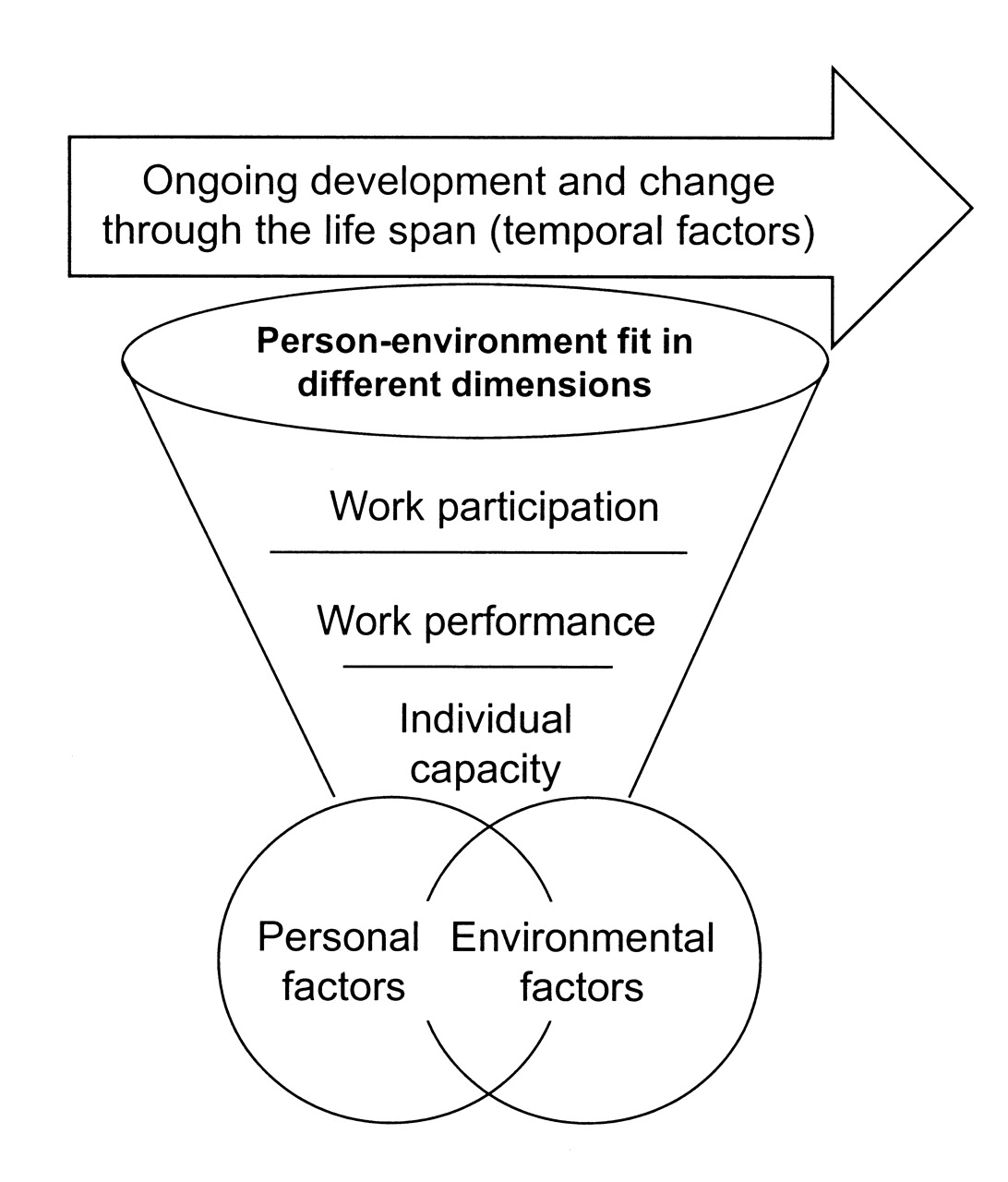
Conceptual framework proposed by Sandqvist and Henriksson31. Level of work functioning is represented as a function of the degree of person-environment fit, spanning 3 dimensions: individual capacity, work performance, and work participation. The greater the overlap between the circles representing personal and environmental factors, the better the level of functioning. Interactions between factors are also considered to be dynamic and may vary across time and throughout an individual’s life span. Reprinted from Sandqvist and Henriksson. Work 2004;23:147–57; with permission from IOS Press.
Collectively, these converging theoretical frameworks have guided our conceptualization of worker productivity, and our understanding of the components that need to be measured in order to comprehensively capture the intended target. Appreciating the way these conceptual frameworks complement each other is important, but differences in scope and focus should also be recognized. For example, the adapted Brouwer, et al model25 emphasizes impacts from only the productivity perspective, while the other 2 frameworks were designed to consider impacts at 3 interrelated domains. Also, health/disease state is considered as a “personal” factor in the Sandqvist and Henriksson model31, but is a distinct component in the ICF. Nonetheless, moving forward, these frameworks will provide the foundation from which to evaluate the performance of candidate measures, and ultimately, to inform the recommendation of outcomes through the OMERACT process.
Learning points:
Conceptual model by Brouwer, et al1,25:
-
Level of worker productivity — a function of health status vs level of job demands
-
Workers may transition between absenteeism <—> presenteeism states
-
Two defined thresholds: below Q1 — able to work but with at-work productivity loss (presenteeism); below Q2: unable to work (absenteeism)
ICF framework27:
-
Worker productivity loss — considered an outcome at the participation level
-
Interactions between health and contextual factors (environmental and personal factors)
Conceptual Model by Sandqvist and Henriksson31:
-
Application of the ICF framework examining domains and factors specific to work
-
Importance of person-environment “fit” and its dynamic nature over time
COMBINING ABSENTEEISM AND PRESENTEEISM
Meeting Our Vision of “One Target Concept, One Outcome.”
Einstein said, “science needs to be as simple as possible but not simpler.” Our vision has always been an ambitious one — to be able to comprehensively capture the impact of arthritis on worker productivity with a single outcome; that is, a single value on a metric that ideally can be applied for clinical evaluative or costing purposes. The Brouwer model helped us recognize that absenteeism and presenteeism may best be represented as different states along a single continuum. However, the best way to apply measurement tools to operationalize this interrelationship remains unclear. At OMERACT 9, we identified 9 productivity-oriented measures7,8,9,22,24,34,35,36,37 that are designed to assess and combine absenteeism and presenteeism, thus the option to use a single outcome to represent the full spectrum of our target concept is available. All such tools similarly emphasize a time-oriented metric to quantify both absenteeism and presenteeism (by estimating or converting scores into equivalent days/hours lost), enabling both components to be summed into a single value. Specific approaches to estimate productivity losses, however, differ widely across instruments, particularly the presenteeism component38. In the simplest example, the Health and Labor Questionnaire8 simply asks respondents to estimate the number of additional hours they would have worked to compensate for production losses due to illness on working days. Other measures, like the Work and Health Interview7, rely on multiple items (n = 5) to quantify reduced work performance, which are translated into a proportion of time impacted. Nonetheless, the general approach to combine absenteeism and presenteeism through a common unit of time-loss or cost appears to have reasonable face validity.
Challenges with Using Presenteeism Measures
Twelve measures that assess only presenteeism were identified from our recent review1. How should we combine these presenteeism scales with absenteeism indicators into a single score? This is a perplexing question that requires continued research and debate. For the purpose of combining scores, it could be argued that multi-item presenteeism scales (that rely on summative scoring) lack compatibility with traditional absenteeism indicators since the latter are often quantified in a more objective manner (e.g., proportion/number of work time missed). Incompatibility of recall periods between absenteeism and presenteeism measures is also a potential issue. The ability to convert presenteeism summative scores into equivalent time-loss/cost values could be one way to combine with absenteeism, although we are aware of this type of conversion for only one of our candidate presenteeism measures. Research by Lerner and colleagues had proposed a regression formula to convert raw Work Limitations Questionnaire-25 score into equivalent percentage productivity loss39, although the generalizability of these conversion rates to different types of work and to arthritis populations is unclear. Some considerations for continued research to enable this method of combining absenteeism and presenteeism may be worthwhile, particularly with candidate presenteeism measures that have received some endorsement from past OMERACT meetings.
Methodologic Issues
The ability to combine absenteeism and presenteeism into a single outcome is also important from a methodologic perspective. Experience has shown that analyzing absenteeism and presenteeism as separate but interrelated outcomes can contribute to a number of practical and computational issues. For example, how should conclusions on the “overall” impact at work be made when differential effects or even conflicting effects are found between absenteeism and presenteeism outcomes? Should we then value changes in one outcome more than the other? When using presenteeism multi-item measures, scoring is problematic when a worker is off-work, since presenteeism becomes an irrelevant concept and can no longer be properly assessed. Should score imputation be performed (e.g., assume maximum score) in these situations? In longitudinal studies, missing-not-at-random data-points40 could be generated when workers are transitioning between working and not working over time. This can be difficult to resolve statistically41, and contributes to an undesirable burden in certain types of analyses. With absenteeism and presenteeism represented as separate outcomes, another challenge is the interpretability of clinical parameters such as minimal clinical important differences for presenteeism scales. Will these parameters be meaningful at all levels of absenteeism? To put it another way, would a defined level of improvement in presenteeism be similarly meaningful to someone working full-time (low absenteeism) versus someone who is only able to work one day a week due to arthritis (high absenteeism)? Perhaps not. For these reasons, it is important to recognize that using multiple outcomes to represent our intended target concept could complicate data analysis and interpretation, and may represent a methodologic disadvantage.
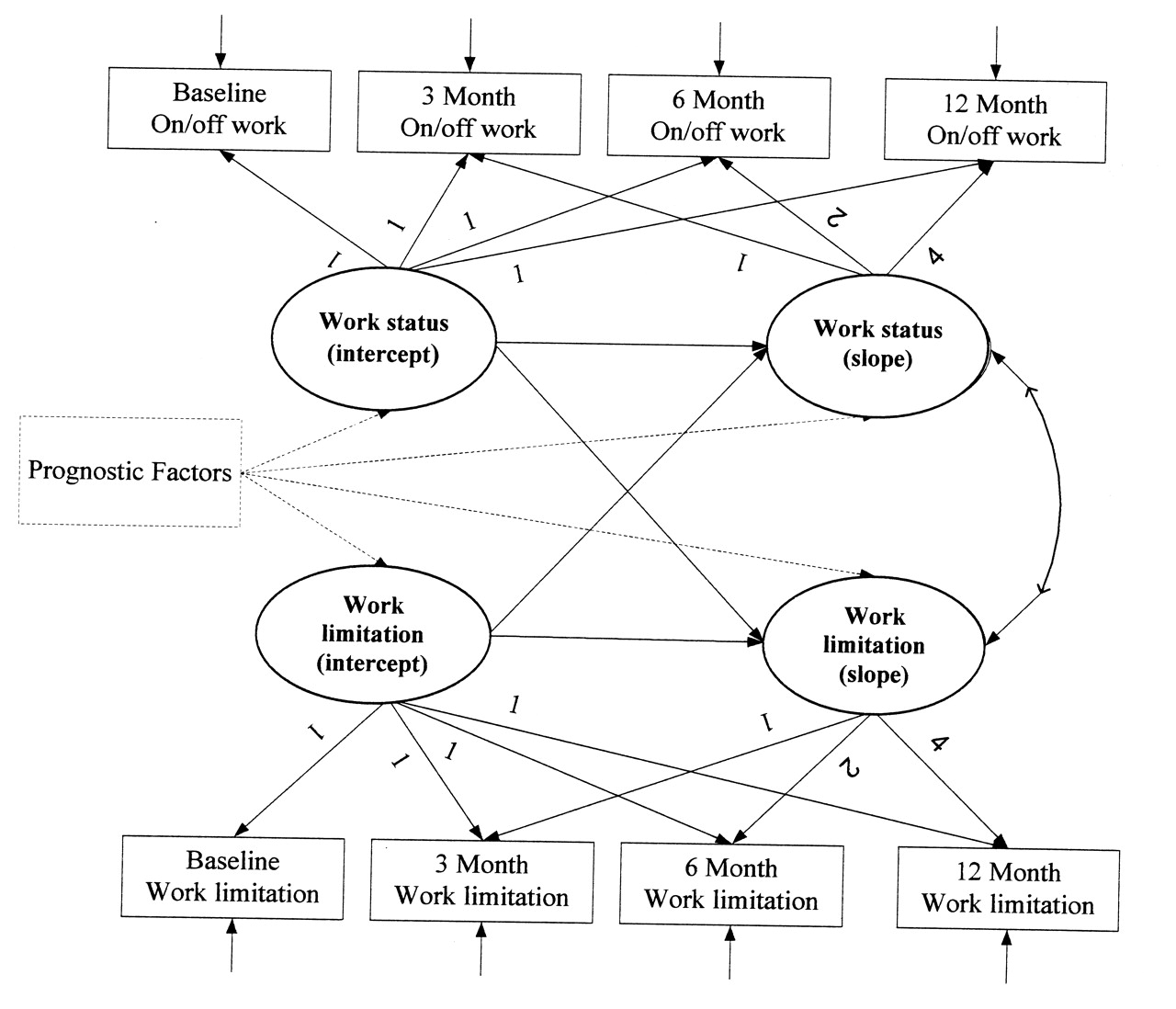
In spite of our vision of “one concept, one outcome” and the associated methodologic issues, it should be acknowledged that in some instances, keeping absenteeism and presenteeism outcomes separate has proven to be useful and informative. First, there is the obvious advantage of being able to disentangle work impacts into more defined conceptual elements to allow unique changes for each component to be more clearly revealed. Second, separate scales may allow more advanced statistical approaches [e.g., structural equation modeling (SEM)] to assess and better understand the interrelationships between absenteeism and presenteeism and other indicators. In Figure 3, we present a potential application of the 2-part growth modeling approach42 in an SEM framework to examine the prognostic factors for both absenteeism and presenteeism over time, while assessing (and controlling for) potential interrelationships between these 2 outcome components, within a single analytical step.

A proposed structural equation modeling approach to evaluate the prognostic factors of worker productivity loss over a one-year period, with both absenteeism (working: on/off) and presenteeism (Work Limitations Questionnaire score)23 outcomes represented in a 2-part growth model42. This analytic approach specifically permits the interrelationship between absenteeism and presenteeism outcomes (as covariates for each other) to be assessed. Intercepts and slopes for absenteeism assessed at 4 study timepoints are represented by the 2 top circles, while intercepts and slopes for the presenteeism over the 4 timepoints are represented by the 2 bottom circles. Paths (potential relationships) between absenteeism and presenteeism to be evaluated are illustrated by the solid arrows among the 4 circles.
A Potential Strategy to Combine Absenteeism with Presenteeism Multi-item Scales
Currently, there are no established approaches to combine absenteeism and presenteeism when the latter is assessed with a multi-item scale that is not intended to be directly translated into an equivalent time/productivity-loss value. An example of this is the 25-item Endicott Work Productivity Scale (EWPS, range 0–100, where 100 = highest presenteeism)43. Numerically speaking, a number of arithmetic strategies to combine this with an absenteeism score are possible, but the most sensible or valid approach to do so remains unclear. The simplest approach may be to simply perform a multiplication between the level of absenteeism (percentage proportion of time missed) and the level of presenteeism (summative score), but with both indicators in reverse orientation to avoid numeric operational issues associated with having zero values represent maximum productivity (Figure 4). This would operationalize total worker productivity as a product of the “proportion of expected time at work” (score range 0–1) and the level of “at-work performance” (score range 0–1, expressed as a proportion of the total presenteeism scale score). For example, a worker working 80% of his normal work hours at a EWPS reversed score of 90/100 (90%) would have a total score of 72% (0.8 x 0.9 = 0.72; i.e., 28% productivity loss) to represent the overall impact of arthritis, factoring in both absenteeism and presenteeism elements. A key issue to consider here is whether the constructs representing the 2 components are sufficiently compatible for combination. Further discussion and testing of the validity of such a strategy is anticipated leading up to future meetings.
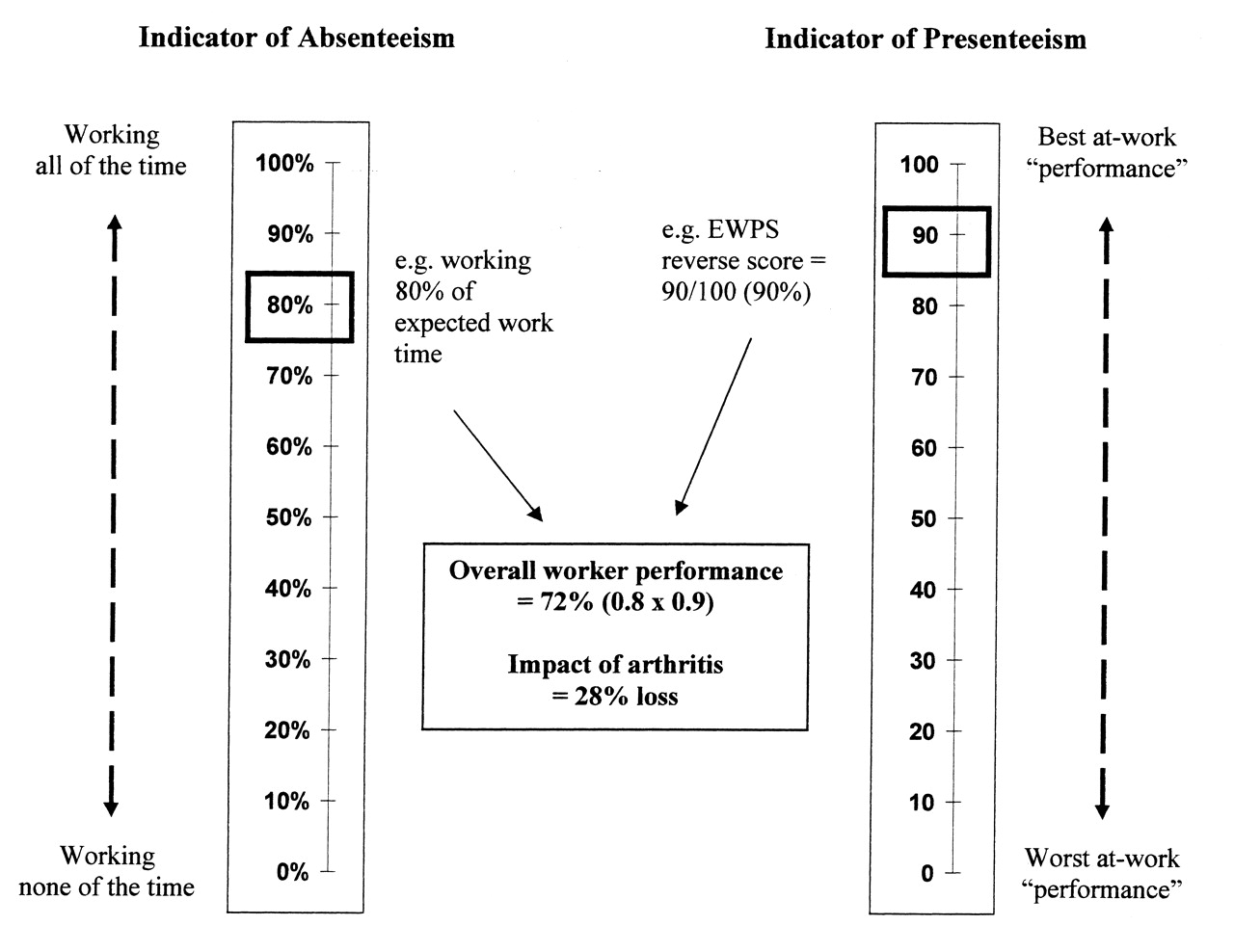
A proposed strategy to combine level of absenteeism with presenteeism psychometric (summative) scores into a single outcome score. An overall worker productivity score is derived by multiplying scores derived from the 2 components (assumes equal weighting for both). An illustrative example using the reversed score from the Endicott Work Productivity Scale43 (EWPS; range 0–100, 100 = lowest presenteeism) is shown.
More Research on Global Indices?
An approach that has been widely used but somewhat underexplored in the measurement of worker productivity is applying a single global index to simultaneously capture information for both absenteeism and presenteeism. This might help mitigate the complexities of having to combine multiple outcomes into a single value. The key to this approach will be to provide the precise scale anchors and instructions so that respondents are primed to concurrently consider experiences related to both absenteeism and presenteeism when using such a tool. In addition to feasibility, a clear advantage is that patients will be allowed to individually determine the relative and perceived impact of their absenteeism and presenteeism experiences, from which to provide a single overall score, as opposed to having this decided a priori by a predetermined scoring algorithm (e.g. addition/multiplication of absenteeism and presenteeism scores, which assumes equal weighting). Certainly, multi-item psychometric scales can provide a detailed view of workers’ experiences, but the performance of these scales could also suffer if specific items are not relevant to the individual worker, especially when the outcome concept is highly contextual. While there are a few global indices available for assessing presenteeism22,24,36, the potential of using global indices to concurrently capture both absenteeism and presenteeism may deserve further research.
From an economics perspective, the challenge to represent absenteeism and presenteeism with a single outcome has been met by converting both components into a metric appropriate for summing (e.g., equivalent time loss, dollar cost). Challenges remain, however, for presenteeism multi-item scales that are not compatible with such conversions, many of which are of high interest for use, especially for clinicians. We have described a number of potential means to accomplish this that could be considered for further research. These approaches include performing a simple arithmetic computation with an appropriate absenteeism score, adopting a global index, or combining outcomes at the analysis stage using more complex 2-part statistical modeling.
CONTEXTUAL NATURE OF WORK
Contextual factors play an important role in shaping the nature and extent of arthritis-related impacts44,45,46, and it is important to be mindful of this when interpreting changes in worker productivity outcomes. In the pre-OMERACT 9 survey, respondents supported the importance of context in assessing work impacts, despite some unfamiliarity with outcomes related to work. Specifically, 62% of respondents believed that persons with arthritis found ways to work around their disease to allow them to function better at work, 54% believed work accommodations could help persons with arthritis stay at work, and 52% agreed that a worker’s productivity could not be measured without some understanding of the contextual factors. Recent studies have shown that workplace culture and support, level of job demands, availability of job modifications or accommodations, and co-worker support are important factors for allowing individuals with arthritis to successfully remain at work29,47,48,49,50. Adaptations made by the individual worker in order to stay at work are also important13,47,51,52,53. Potential societal-level factors, or “macroeconomic conditions”54, are also important to recognize. For example, labor market climate55, public health policies, and social regulations56 (e.g., sick leave and work disability policies, availability of funding for medications and other health benefits) could indirectly impact whether a person with arthritis is able to find suitable employment and be productive at work. Assessments of productivity losses at the “workplace” level may also consider additional factors such as the ability of the company to compensate for absent workers with replacement workers. At OMERACT 10, our main objective was to examine what participants felt were the most relevant contextual factors to consider when using work productivity outcomes, to build on the general opinion from previous survey results.
Contextual Factors of Worker Productivity Identified
At the WP-SIG, we presented a brief case scenario to engage participants to brainstorm factors that might help a person with arthritis to “make return to work successful, productive, and sustainable.” After writing each identified factor on separate cards, we then performed a “dot voting” exercise, where participants were able to anonymously vote for specific factors that they felt were most important to consider (12 votes allowed per participant, multiple votes on same factor permitted). Table 1 summarizes the 24 contextual factors (in their original description) identified during this exercise and the number of votes received from participants. Sixteen of the 24 factors received at least 1 vote, and the 2 top factors were “support at home” and “flexibility of work scheduling” although each received only a modest proportion (13%) of all votes. This indicates strong diversity of viewpoints in terms of which specific factors were considered most important.
Contextual factors identified at the OMERACT 10 Worker Productivity Special Interest Group and number of votes received for each factor during a “dot voting” exercise (12 votes available per participant, multiple votes on same factor permitted).
Post-OMERACT 10, these contextual factors were compiled with additional personal and environmental factors that have been discussed conceptually in the literature6,28,31,44,57, or have had supporting evidence in arthritis (Table 2). This full list of 70 factors was organized into a proposed 2-tiered classification: (1) as either a personal or environmental factor, and then (2) into one of 15 broad domains: health, demographic attributes, economic need, personal appraisal, related skills/abilities, work-life balance, accessibility, economic climate/labor regulations, nature of work, workplace support, non-workplace support, organizational policies and practices, physical environment, work accommodations, and others. Of further interest was how well these factors could be mapped onto the associated categories of the ICF classification. Based on agreement between 3 coders (KT, RE, AB), we found 35 (50%) of our identified factors had compatibility with existing ICF categories, including a few that were coded outside the sections on contextual factors. This suggests that while all factors are broadly considered in the ICF framework, not all factors demonstrate a precise fit with its classification structure (either too specific or too broad). Also, personal factors remain unspecified in the ICF, and therefore cannot be coded at present.
Contextual (environmental or personal) factors of worker productivity loss or work disability that have supporting evidence in arthritis, have been discussed conceptually in the literature, or were identified at the OMERACT 10 Work Productivity Special Interest Group. Factors are mapped onto the International Classification of Functioning, Disability and Health (ICF) coding system to access degree of compatibility in terms of classification. For the purpose of brevity, titles of the ICF categories were abbreviated (refer to the ICF handbook for full titles27).
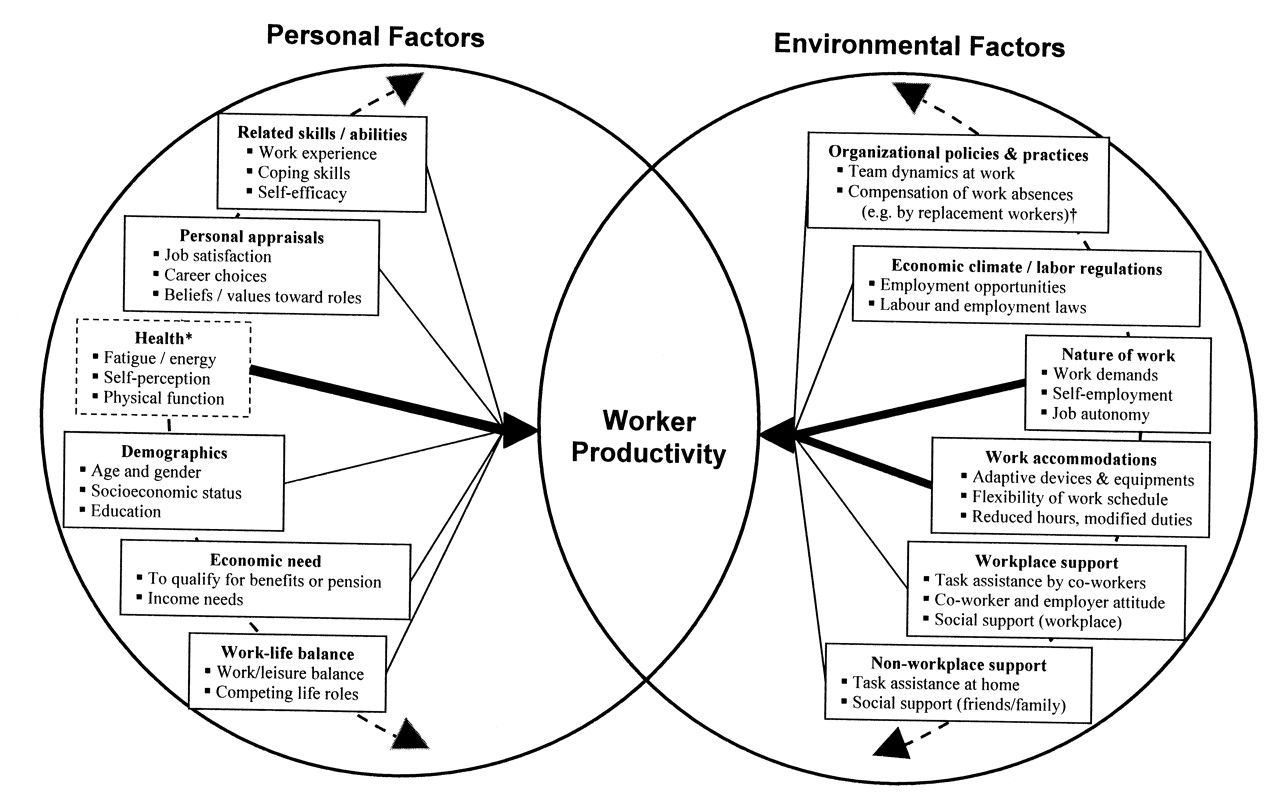
The current examination of the relevant contextual factors allowed us to elaborate on the conceptual model by Sandqvist and Henriksson31. Figure 5 illustrates the range of specific factors that may contribute to the person-environment intersection. Degree of relevance of individual factors (represented by thickness of arrows) is expected to vary between individuals, and may also evolve over time within the individual if there are changes to one’s circumstances (e.g., health, work, life events). It is also important to consider that factors may interact not only across but also within the personal and environmental divisions (represented by semicircular arrows linking the factors). For example, the importance of receiving job accommodations may be diminished if a worker has a job with highly flexible work schedule and receives strong support from co-workers. Social support from family/friends may have added importance for a self-employed worker than someone working within a supportive team environment in a larger organization. On the personal side, if economic need is modest for an individual, considerations of job satisfaction and achieving work-life balance may come to the forefront.

Conceptual representation of the interaction between contextual factors that contribute to the person-environment “fit,” to elaborate on the framework on work functioning proposed by Sandqvist and Henriksson31. We have depicted level of worker productivity as our measurement target of interest (represented as the area of overlap between the 2 circles). Specific factors and degree of relevance (indicated by thickness of arrows) to the overall construct is expected to vary between individuals, and may also evolve over time within the individual if there are changes in circumstances (e.g., health, work, life events). Factors are also believed to interact with each other within the personal and environmental divisions (semicircular arrows behind the factors). *Some health-related factors may not be represented as “personal” factors in the ICF framework. †Some factors associated with organization policies and practices may affect work productivity primarily at the “workplace” level, rather than at the “individual” level. From Sandqvist and Henriksson. Work 2004;23:147–57. Adapted with permission.
Implications for Interpreting Work Productivity Outcomes
Since level of worker productivity could be viewed as a function of the level of person-environment fit, some care is needed when comparing outcome scores between as well as within the individual. Will the level of worker productivity have the same meaning if the job has changed for the same individual over time? How can we compare between people with different levels of job demand? When there is a change in productivity, how can we know if it is attributable to a change in the worker’s health or a change in the level of job demands placed on the individual (by job accommodations, changing jobs, etc.), or both? How could we differentiate a brief episodic versus a more sustained change with these outcomes? With these issues in mind, it is important not to simply presume that an increase in the level of worker productivity automatically represents an “improvement,” or that a decrease in score is synonymous with “deterioration,” without some understanding of any concurrent changes to contextual factors. When designing a clinical trial, it may be prudent to measure key contextual factors when using worker productivity outcomes, recognizing the potential for these factors to contribute to confounding bias. For example, data could be collected on whether job accommodations were received by workers, and whether this factor differed between comparison groups over time in a randomized controlled trial. We may also collect data on whether patients had changed jobs over time, and whether this influenced the level of job demands placed on the individual worker. For multicenter trials, we may also examine whether patients from different geographical regions are evenly distributed after randomization such that societal-level contextual factors (that could dictate the availability of sick leave or suitable jobs) would not have biased comparisons across regions. Moving forward, we assert that it will be important to collect data on key contextual factors in future studies to help facilitate a more accurate interpretation of changes in worker productivity. One of our objectives over the next 2 years will be to determine which contextual factors should be considered “essential” to assess in conjunction with worker productivity outcomes, and whether score adjustment strategies based on such factors are appropriate.
LOOKING FORWARD TO OMERACT 11
The goal of establishing valid outcomes to quantify the impact of arthritis on work has provided us with many challenges from a measurement perspective. The intrinsic broadness of our target concept, the different measurement perspectives and intended applications, the complex interrelationships between components that collectively make up our measurement target (e.g., absenteeism <—> presenteeism), and the highly contextual nature of work were among the key issues examined leading up to OMERACT 10. Importantly, these challenges also have given rise to additional questions to be addressed. In our outcome selection process, should we continue to consider measures that represent different perspectives (e.g., productivity loss vs disability)? Do candidate measures need to be able to provide outcome scores that are compatible for different research purposes (e.g., clinical vs costing studies)? Should the continued consideration of presenteeism-only measures in the OMERACT process be contingent on their ability to be combined with absenteeism indicators to provide a single outcome score in a sensible manner? We will continue to focus our efforts towards resolving the issues and questions raised in this article, to help set the stage for the recommendation of candidate worker productivity measures at future OMERACT meetings.
Summary of Progress at OMERACT 10
-
Identified 3 complementary theoretical frameworks to guide our conceptualization of worker productivity: basis for continued evaluation of candidate measures.
-
Proposed a number of potential methodologic approaches to combine absenteeism with presenteeism multi-item measures.
-
Brainstormed and reviewed contextual factors of work productivity, and expanded on the person-environment interaction proposed in the Sandqvist and Henriksson framework31.
Future Objectives
-
To reach consensus on specific domain(s) to be measured in order to capture the full scope of worker productivity.
-
Perform further research to examine the merit (strengths and limitations) of different approaches to combine absenteeism and presenteeism indicators.
-
Define essential contextual factors to be assessed when applying worker productivity outcomes in clinical trials or longitudinal observational studies.
Acknowledgment
The authors acknowledge all participants of the OMERACT 10 Worker Productivity Special Interest Group for their contributions. We also thank other members of the I-CAN-WORK Alliance for contributions to this work and encouragements to explore contextual factors in this field: Mieke Hazes, Axel Finckh, Catherine Hoffstetter, Marc Koopmanschap, Nick Bansback, Claire McGrath, and Annemarie Braakman-Jansen. We also acknowledge Depeng Jiang for providing consultations on statistical approaches to model absenteeism and presenteeism outcomes.
Footnotes
-
Supported by the Canadian Arthritis Network (part of the Networks of Centres of Excellence) in partnership with The Arthritis Society and the Research Advisory Council of the Workplace Safety and Insurance Board of Ontario; by an unrestricted grant from Abbott; and funding provided by OMERACT. K. Tang is supported by a PhD Fellowship from the Canadian Institutes of Health Research, a Canadian Arthritis Network Graduate Award, a Syme Fellowship from the Institute for Work and Health, and an OMERACT Fellow Travel Bursary from the American College of Rheumatology. R. Escorpizo is supported by a grant at Swiss Paraplegic Research and a EULAR travel grant. D.E. Beaton is supported by a Canadian Institutes of Health Research New Investigators Award. C. Bombardier holds a Canada Research Chair in Knowledge Transfer for Musculoskeletal Care. D. Lacaille is supported by an Investigator Award from The Arthritis Society of Canada and is the Nancy and Peter Paul Saunders Scholar. W. Zhang is supported by a Canadian Institutes of Health Research Doctoral Research Award in the Area of Public Health Research and a Canadian Arthritis Network Graduate Award. R.H. Osborne is supported in part by a National Health and Medical Research Council Population Health Career Development Fellowship.
REFERENCES
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}