

Abstract
Reactivation of latent tuberculosis infection (LTBI) is well recognized as an adverse event associated with anti-tumor necrosis factor-α (anti-TNF-α) therapy. The strengths and weaknesses of current techniques for detecting LTBI in patients with chronic inflammatory diseases such as rheumatoid arthritis (RA) and psoriasis have not been fully examined. T cell hyporesponsiveness due to immunosuppression caused by illness or drugs, referred to as anergy, may produce false-negative tuberculin skin test (TST) and interferon-γ release assay (IGRA) results. The literature suggests that anergy may influence screening performance of TST and IGRA tests in candidates for anti-TNF-α therapy. Conversely, the potential for false-positive TST and IGRA results must be considered, as treatment for LTBI may be associated with significant morbidity. This review examines the reliability issues related to LTBI diagnostic testing and provides practical direction to help prevent LTBI reactivation and facilitate successful anti-TNF-α treatment.
- TUMOR NECROSIS FACTOR-α
- LATENT TUBERCULOSIS INFECTION
- ANERGY
- TUBERCULIN TEST
- INTERFERON-γ
- DELAYED HYPERSENSITIVITY
The incidence and severity of tuberculosis (TB) in patients receiving tumor necrosis factor (TNF) antagonists is a major concern1; thus, accurate screening for and treatment of latent tuberculosis infection (LTBI) before initiating therapy is crucial to minimize risk of reactivation and resultant serious infection. Our review provides direction on LTBI testing in TNF antagonist therapy candidates and examines LTBI testing reliability prior to or during such treatment, with specific attention to anergy, or T cell hyporesponsiveness due to immunosuppression that results from illness or drugs.
TB disease in patients receiving TNF antagonists
Etanercept, adalimumab, infliximab, golimumab, and certolizumab are TNF antagonists approved in Canada. There are 2 types of TNF antagonists: soluble TNF receptor (TNFR) and monoclonal antibody. Etanercept is a soluble TNFR construct fused to the Fc portion of IgG, while adalimumab, golimumab, infliximab, and certolizumab are monoclonal antibodies. Etanercept, adalimumab, and infliximab are indicated for rheumatoid arthritis (RA), ankylosing spondylitis (AS), psoriatic arthritis (PsA), and psoriasis. Adalimumab and infliximab are also indicated for Crohn’s disease. Golimumab is indicated for RA, AS, and PsA; certolizumab is indicated for RA.
TNF antagonist treatment is associated with an increased incidence of TB. Some evidence has shown there is variation in the incidence of TB across agents. Three adequately powered studies demonstrated that infliximab and adalimumab have an increased incidence of TB compared to etanercept1,2,3. A recent analysis that combined 5 studies found that the time to onset of TB with infliximab was shorter (16.2 weeks) than that of etanercept (59.6 weeks)4.
Several structural and functional differences could explain the higher TB incidence with monoclonal versus soluble inhibitors. One difference is binding kinetics; TNF readily dissociates from etanercept but dissociation from infliximab was undetectable5. Another difference is binding stoichiometry; etanercept binds only trimeric soluble or transmembrane TNF, 1 trimer per 1 etanercept dimer. Infliximab binds both monomeric and trimeric soluble or transmembrane TNF5. Since monoclonal antibodies can bind 2 TNF molecules, cross-linking of multiple membrane-bound TNF-α by monoclonal antibody can occur, leading to large immune complex formations5,6. However, certolizumab is a monoclonal antibody fragment (Fab) and therefore cannot cross-link transmembrane TNF. This may suggest that an alternative mechanism may be responsible for the increased risk of TB using this class of therapy7. In light of this, the exact mechanism by which TNF antagonists cause TB reactivation or de novo TB is not well understood. Even though monoclonal antibodies demonstrated an increased incidence of TB, the risk of TB reactivation with etanercept therapy is not negligible1,3. Appropriate screening for LTBI is required for all TNF antagonist candidates, regardless of mechanism of action.
The estimated risk of TB in persons taking TNF antagonists relative to persons with no known risk factor is 1.5 to 41,8. In comparison, the estimated risk of TB for patients taking glucocorticoids, immunosuppressant therapy (organ transplant), and those with AIDS is 4.9, 20 to 74, and 110 to 170, respectively9,10,11,12,13,14,15.
In addition, TB reactivation following LTBI treatment can occur after starting TNF antagonist treatment16,17,18 and may be more likely in patients with significant apical fibronodular disease16.
Screening for LTBI in candidates for TNF antagonist therapy
Testing methods
In Canada, LTBI testing is indicated when there is an increased risk of developing TB disease19. There are 2 main methods to diagnose LTBI: the tuberculin skin test (TST) and the newer interferon-γ release assays (IGRA). The TST performed by the Mantoux method (Table 1) is used in Canada, the United States, and the UK19,20,21. It involves intradermal injection of purified protein derived (PPD) from Mycobacterium tuberculosis bacteria. Injection site induration within 48 to 72 hours caused by manifestation of a recall immunological response to TB antigens suggests past or present infection19,20,21. The 2-step TST is mainly used for persons who will have routine serial screening for LTBI, such as healthcare workers19. IGRA quantifies interferon-γ (IFN-γ) production from T cells and is based on the fact that T cells already sensitized to TB antigens produce high IFN-γ levels once reexposed19.
Summary of recommendations for identifying and managing latent tuberculosis infection (LTBI) in at-risk populations.
Screening recommendations in Canada, the US, and the UK (Table 1)
Immunosuppressed persons [e.g., those with end-stage renal disease (ESRD), diabetes, human immunodeficiency virus (HIV), corticosteroid therapy, or TNF antagonist therapy] are included in the at-risk population discussed in the 2007 Canadian Tuberculosis Standards19, the 2010 Canadian Tuberculosis Committee (CTC) updated recommendations22, the 2000 US Recommendations20, and the 2010 US updated guidelines for using IGRA23. However, the UK National Institute for Health and Clinical Excellence (NICE) Guidelines (2006)21 do not reference immunosuppressed populations. The following all provide focused recommendations for patients taking or candidates for TNF antagonists: the Canadian Tuberculosis Standards and CTC update recommendations, the 2005 British Thoracic Society Guidelines, the 2010 European TBNET Consensus Statement, the 2007 Health Protection Agency position statement on the use of IGRA (which supplements the NICE Guidelines), and the Centers for Disease Control and Prevention (CDC)19,22,24,25,26,27.
The CTC states that an IGRA test may be used if the initial TST result is negative and there is concern about LTBI in an immunocompromised person22. If 2 consecutive indeterminate IGRA results occur, clinicians should suspect anergy and are advised to rely on history, clinical features, and other laboratory results.
TNF antagonist manufacturer’s recommendations for TB/LTBI screening
Labels for TNF antagonists approved in Canada indicate all patients be evaluated for both active and latent TB before starting therapy. The etanercept label recommends evaluation according to the Canadian Tuberculosis Standards, while the labels for adalimumab, infliximab, and certolizumab indicate screening with TST. Only the adalimumab label states that a ≥ 5 mm induration size, for LTBI testing, is considered positive even for patients vaccinated with Bacille Calmette-Guérin (BCG), a consideration that is contrary to the Canadian and British TB guidelines19,24. All labels warn of possible false-negative TST in immunocompromised or severely ill patients. In addition, labels for infliximab and certolizumab recommend taking a TB medical history.
All TNF antagonist labels recommend that if LTBI is diagnosed, treatment with anti-TB drugs should be started before initiating TNF antagonist therapy. In the ideal world, completion of LTBI treatment may be the preferred option. However, in practice this could be difficult to accomplish, so some experts suggest 4 weeks of LTBI therapy before initiating TNF antagonist treatment27. All TNF antagonist labels, except for certolizumab, state that anti-TB therapy should be decided by consulting a TB expert if patients have a negative LTBI test yet still have a high risk of TB infection. All manufacturers advise that patients with active TB should not receive TNF antagonist therapy.
All TNF antagonist labels suggest appropriately monitoring for TB disease during and after TNF antagonist treatment, including patients who tested negative for LTBI. Although new infections are rare in low TB-prevalence countries such as Canada and the United States, they are of greater concern in countries with a high burden of illness28. It is important to note that it is possible that medications other than TNF antagonist therapies (including emerging therapies or new indications) may have an effect on the expression of TB.
Detection of LTBI using TST
Practical strengths and weaknesses
Advantages include low cost, simplicity, and validation in large cohorts19. Testing, administration, and reading techniques can lead to variability in test results; thus, testing should be performed by trained health professionals19.
Measures of screening performance
TST can deliver false-positive and false-negative results. Because of the potential for serious isoniazid (INH) hepatotoxicity reported with treatment of LTBI in patients with RA receiving methotrexate or sulfasalazine and TNF antagonists29, LTBI tests should maintain sufficient specificity to minimize false-positives and potential adverse effects of unnecessary LTBI treatment. False-positive TST can be caused by previous BCG vaccination, sensitization to environmental nontuberculous mycobacteria (NTM), or inappropriate induration cutoff thresholds30. In a recent metaanalysis, BCG taken by 12,728 subjects after 1 year of age yielded 41.8 false-positive TST reactions per 100 vaccinees31. BCG vaccination was discontinued in Canada as TB incidence rates began to fall. Children in Quebec, Newfoundland and Labrador, and Prince Edward Island were routinely BCG-vaccinated from the 1940s to the 1970s. Vaccination of healthcare workers was discontinued in the 1970s in Alberta, British Columbia, Manitoba, New Brunswick, Nova Scotia, Ontario, and Prince Edward Island. Many First Nations and Inuit populations continue to be vaccinated19. Worldwide, BCG continues to be widely used (BCG World Atlas; McGill University, Public Health Agency of Canada; http://bcgatlas.org).
False-negative TST can result from immune suppression caused by immunosuppressive therapies, coexisting illness (HIV, cancer, chronic renal failure, recent viral illness such as mononucleosis, mumps, and measles), or inappropriate induration cutoff thresholds19,31.
Effect of anergy on screening performance
A consistent definition of anergy is absent from the literature; however, one possible clinically relevant definition is T cell hyporesponsiveness to previously exposed antigens due to immunosuppression caused by illness or drugs that may produce false-negative TST and IGRA results.
Anergy testing was developed to more accurately identify anergy in immunocompromised populations in order to better interpret negative TST results. It involves skin testing with a panel of control antigens, for example, Candida albicans and mumps. The CDC defines anergy as no reaction to these control antigens32. Anergy testing limitations include no standard convention for classifying positive response, the fact that validity in diagnosing TB has not been demonstrated, and the lack of reproducibility and standardized protocol33. Thus anergy testing is not recommended by Canadian and US TB guidelines19,20,33.
To maximize TST sensitivity, Canadian and US TB guidelines indicate a reduced induration threshold that defines a positive TST for the immunosuppressed population versus the general population. In most clinical situations in Canada, the criteria is 10 mm induration size19. However, ≥ 5 mm defines a positive reaction for immunosuppressed patients (e.g., HIV infection, organ transplant, corticosteroid therapy, TNF antagonist therapy). In the US, the threshold for persons with no TB risk factors is ≥ 15 mm, but for immunosuppressed persons, the cutoff is ≥ 5 mm20,26. Contrary to the North American standards19,20,26, the 2010 European TBNET Consensus Statement27 recommends a TST cutoff of ≥ 10 mm for immunocompromised conditions.
Some studies show that a blunted or reduced recall response, often called anergy, can produce false-negative TST results in patients with RA not on immunosuppressive therapy34,35,36,37. Sezer and colleagues observed that untreated patients with early-stage RA had statistically significant smaller induration diameter compared to treated patients with RA and AS, and healthy subjects34. This less robust response to PPD may be due to the T cell’s active role in developing RA, thus a blunted response to PPD34. In addition, data confirm that RA monocytes have lower PPD-antigen presentation capacity37. Patients with RA receiving immunosuppressive therapy may exhibit attenuated delayed-type hypersensitivity (DTH)38,39,40,41,42. A higher dose of methotrexate is associated with PPD anergy and a higher steroid dose was a predictor of negative PPD42. It has been reported that high doses of prednisone (≥ 15 mg/day) can cause false-negative TST reactions43. A decrease in memory T4 cells was found in anergic patients, which may contribute to the decrease in antigen reactivity41. In contrast, there is weak evidence that supports the absence of anergy in patients with RA44,45. However, the evidence supporting anergy in patients with RA is confounded by concomitant immunosuppressive medications and disease severity.
In addition to the RA population, evidence supports the existence of anergy in patients with ESRD on hemodialysis, HIV, or lupus46,47,48. A significantly higher proportion of patients with ESRD had no TST induration versus controls47. Similarly, HIV-positive patients were significantly less likely to be TST-positive compared to HIV-negative patients46. Patients with active systemic lupus erythematosus had lower skin response to PPD than inactive or control patients48.
Detection of LTBI using IGRA
Scientific basis of IGRA
Currently, 2 IGRA types, QuantiFERON®-TB Gold In-Tube (QFT-GIT) and T-SPOT®.TB [a simplified variant of the enzyme-linked immunospot (ELISPOT)], are approved in many countries. QFT-GIT is the latest generation test; its predecessors include QuantiFERON®-TB (QFT) and QuantiFERON®-TB Gold (QFT-G), approved in 2001 and 2005, respectively. QFT-GIT involves collecting whole blood and incubating it with proteins specific to M. tuberculosis but absent from BCG (unlike the TST) and most NTM. Lymphocytes from TB-infected patients will recognize M. tuberculosis-specific proteins and respond by releasing IFN-γ, which is quantified. T-SPOT.TB is similar to QFT-GIT, except that quantified peripheral blood mononuclear cells are incubated and enumerated.
Practical strengths and weaknesses
Although initial material and ancillary costs are greater than TST, IGRA can improve LTBI detection specificity in a BCG-vaccinated population. IGRA testing for the most part requires 1 appointment, while TST requires a second appointment 48 to 72 hours later. Additionally, IGRA uses a negative control and a positive mitogen-based control, minimizing additional visits due to inconclusive results19. However, a repeat test is required if an inclusive IGRA result occurs. The labels for QFT-GIT and T-SPOT.TB state that if the response to TB antigens is negative but the response to the mitogen is low, the result is considered indeterminate. A study by Greenberg and colleagues demonstrated an increase in indeterminate results due to low mitogen responses in patients with RA using the earlier generation IGRA (GFT)44. Such a result can provide additional information because it could be due to poor specimen preparation, insufficient lymphocytes (for QFT), reduced lymphocyte activity due to improper specimen handling, incorrect filling/mixing of the mitogen tube, or inability of the patient’s lymphocytes to generate IFN-γ (one facet of anergy).
Measures of screening performance
A recent metaanalysis identified 38 studies published prior to March 31, 2008, that examined sensitivity and specificity of QFT-G, QFT-GIT, and T-SPOT.TB49. Eight studies were excluded because they included noncommercial assays, leaving 30 studies for analysis. Studies assessing sensitivity had patients with microbiologically confirmed active TB but who were not immunocompromised. Studies assessing specificity had healthy patients with a low risk of TB and no known exposure to TB. The IGRA type used in the 30 studies was 11 QFT-G only, 5 QFT-G and T-SPOT.TB, 2 QFT-GIT and T-SPOT.TB, 4 QFT-GIT only, and 6 T-SPOT.TB only. Pooled sensitivity of the 22 QFT-G/QFT-GIT and 13 T-SPOT.TB studies was 76% (95% CI 72% to 80%) and 90% (95% CI 86% to 93%), respectively. Pooled specificity was 98% (95% CI 96% to 99%) for all QFT-G/QFT-GIT studies and 93% (95% CI 86% to 100%) for T-SPOT.TB. Sensitivity estimates for TST were heterogeneous, with a pooled estimate of 77% (95% CI 71% to 82%). Specificity estimates for TST in non-BCG-vaccinated populations were consistently high, with a pooled estimate of 97% (95% CI 95% to 99%). Specificity was low in BCG-vaccinated populations, 59% (95% CI 46% to 72%) and highly heterogeneous49. Overall, the pooled T-SPOT.TB sensitivity was higher than that of the QFT-G and QFT-GIT assay49. This has also been shown in rheumatic patients scheduled for TNF antagonist treatment and in immunocompromised patients50,51. It is important to note that the lack of a gold standard for LTBI diagnosis is a limitation in the studies that assessed TST and IGRA specificity and sensitivity. In the absence of a gold standard, populations with active TB and low risk of TB were used by Pai and colleagues as surrogate standards to estimate accuracy49.
Some studies suggest that IGRA, when compared to TST, may improve specificity and sensitivity in diagnosing LTBI prior to or during TNF antagonist treatment in patients with rheumatic disease30,38,52,53,54,55,56,57,58,59. Some data propose that IGRA reduces false-positive TST results associated with BCG and NTM and may minimize the number of false-negative TST results due to immunosuppression30,38,52,54,55,57,58,60. It should be noted that IGRA tests may also generate false-positive results, which may limit the utility of these tests for detecting LTBI without the use of other complementary tests53. Accordingly, some studies58,59 suggest IGRA should replace TST, while others30,38,44,52,53,54,57,60,61 suggest concomitant tuberculin skin and IGRA testing is more effective in diagnosing LTBI in all patients. Inanc and colleagues propose retesting patients with QFT-G after starting TNF antagonist therapy if QFT-G results before starting TNF antagonists were negative or indeterminate55. However, there are conflicting data on whether IGRA improve specificity and sensitivity and the role of these new methodologies remains under study.
Few data exist on patients with psoriasis regarding LTBI detection and use of IGRA. However, a study by Laffitte and colleagues screened for LTBI in patients with psoriasis before TNF antagonist treatment by comparing T-SPOT.TB versus TST, and found a positive T-SPOT.TB strongly associated with risk factors for LTBI62. This study represents the first report of the frequency of LTBI (20%) in patients with psoriasis prior to TNF antagonist therapy. The incidence reported here is considerably higher, and it is possible that this overestimation could be due to the small number of patients in the study; to the fact that 20% of patients came from or previously lived in a country with a high incidence of TB62; or to false-positive results that may have occurred with the use of IGRA53.
The effect of anergy on screening performance for patients treated with TNF antagonists
Clinical studies in patients receiving TNF antagonist therapy for inflammatory diseases, including RA, demonstrated a decrease in IFN-γ-releasing CD4+ T lymphocytes or a decrease in IFN-γ production63,64. This decrease in IFN-γ due to TNF antagonist treatment could cause an indeterminate or false-negative IGRA result, thus Hamdi and colleagues recommend against using the ELISPOT assay to diagnose LTBI in patients receiving such treatment63. Currently, there are not enough consistent data to evaluate the effect of TNF antagonists on TST.
Discordance between TST and IGRA results
Multiple studies demonstrate discordant TST and IGRA results30,38,44,52,53,54,58,61,62,65. Discordant results in an RA population that includes candidates for TNF antagonist therapy or those currently receiving it can be explained by several factors: differences between study populations; a false-negative TST or IGRA caused by anergy; a false-positive TST due to BCG vaccination or NTM infection; an indeterminate IGRA that results from immunocompromised status and/or TNF antagonist treatment, further suppressing the immune response; poor sample preparation; or inconsistent laboratory technique19,30,38,44,52,54,57,61,65,66. BCG vaccination also causes discordant results between TST and T-SPOT.TB in patients with psoriasis prior to TNF antagonist therapy62. Although evidence suggests that IGRA with TST, used as screening tools for LTBI, improve specificity and sensitivity in populations with prior BCG vaccination and possibly other select populations, anergy can cause indeterminate or false-negative IGRA and TST results. Thus, clinicians should refer to guidelines that recommend relying on patient history, clinical features, and other laboratory results to diagnose LTBI in immunocompromised patients19.
Individualizing assessment of LTBI in candidates for TNF antagonist therapy
It is important that LTBI diagnostic tests maintain sufficient specificity and sensitivity, to minimize unnecessary LTBI therapy with isoniazid and activation of TB in patients with LTBI who receive TNF antagonist treatment. Whether a TB specialist, rheumatologist, or dermatologist is responsible for LTBI screening depends on what is appropriate in the physician’s region and the resources that are available.
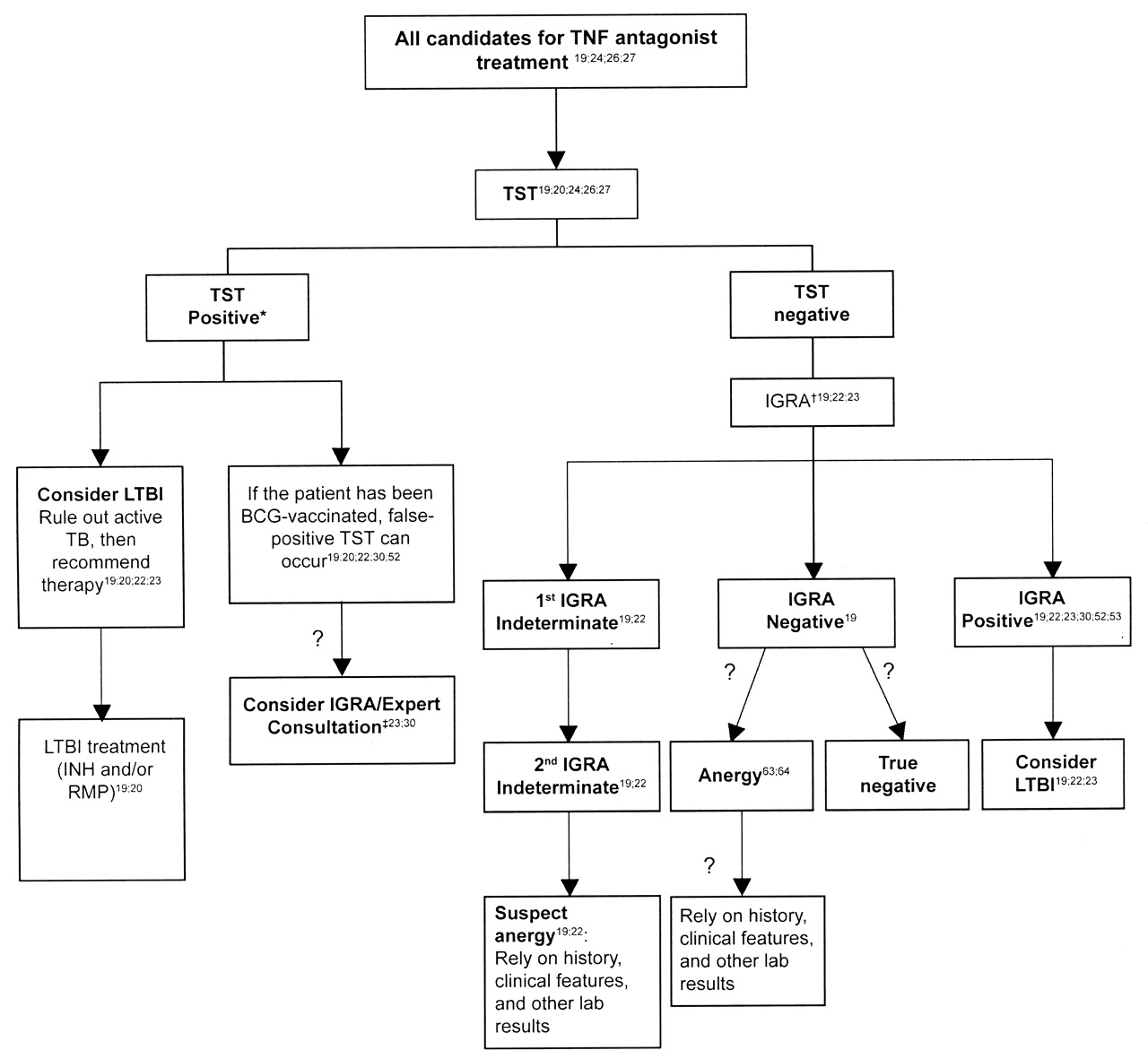
LTBI screening is discouraged in healthy persons where TB risk is low19. However, the Canadian TB Standards and TNF antagonist product labels mandate screening for LTBI and active TB in all immunocompromised patients19 and candidates for TNF antagonist therapy, respectively (Table 1, Figure 1). In such cases, the first test should be a TST. If the patient is immunosuppressed and was not BCG-vaccinated and the induration is ≥ 5 mm, then the TST is interpreted as positive. The patient should be considered to have LTBI after active TB is ruled out by chest radiograph and medical examination. If the patient has been BCG-vaccinated, a false-positive TST can occur and an IGRA may be of benefit23,30, however, it is not recommended by the CTC22 and further evidence is needed. It is increasingly recognized that a TST may overestimate true LTBI67. This has resulted in the recommendation to use IGRA to clarify a positive TST result in adults at low risk22,23. Whether this applies to persons being considered for TNF antagonists is unknown but is under study68. When clinical suspicion suggests a possible false-negative TST in an immunocompromised person (e.g., someone with HIV, organ transplant, ESRD, or TNF antagonist therapy), an IGRA may be used, with the T-SPOT.TB being the preferred test19,22. If 2 indeterminate results occur, anergy is suspected and the clinician must rely on history, clinical features, and other laboratory results to make a decision. For the general nonimmunocompromised Canadian population with no TB risk, the TST induration cutoff is 10 mm19.

Evaluation of latent tuberculosis infection (LTBI) in candidates for tumor necrosis factor (TNF) antagonist therapy. *Tuberculin skin test (TST) positivity varies according to the population under study. For a normal population, a TST > 10 mm should be considered positive19. For a population at risk (including HIV infection; close contact of active contagious case; children suspected of having TB disease; abnormal chest radiograph with fibronodular disease; other immune suppression such as TNF antagonist therapy, chemotherapy), ≥ 5 mm should be considered positive19. †Consider based on background risk. Interferon-γ release assay (IGRA) positivity varies according to the population under study. How different populations affect IGRA results is still unclear. ‡May be beneficial, but further evidence is required. ?: Areas with few data, which will continue to evolve. BCG: Bacille Calmette-Guérin; INH: isoniazid; RMP: rifampicin.
Even if the baseline evaluation suggests no LTBI, TB may still develop while taking TNF antagonist therapy38,61. Thus careful evaluation of new symptoms suggestive of active disease must be performed while patients receive TNF antagonist therapy19.
The risk of progressing to active TB in patients with RA is elevated, likely the result of both the underlying disease and more importantly, nonbiologic medications, particularly corticosteroids9,69. According to the Canadian TB Standards, ≥ 5 mm is the TST cutoff for immunosuppressed patients19. Patients with moderate to severe RA may have reduced response to TST and potentially IGRA as a result of concomitant medications and in some instances as a result of their underlying disease process34,37,38,40,42,63,64,70. Consideration should be given to the risk and benefit of the 5 mm cutoff, as the number of false-positives may be high in patients who are not immunosuppressed or anergic. However, according to the American College of Rheumatology, a TST is considered positive if the reaction is ≥ 5 mm for immunosuppressed patients with RA71.
For the patient with psoriasis, currently there is no evidence of anergy; however, the absence of data does not exclude the phenomenon in psoriasis and other diseases. Relatively speaking, patients with psoriasis are healthy, therefore a 5 mm TST cutoff is not reasonable. Although there is a lack of evidence from national guidelines, the standard of care followed in Canada for LTBI screening in patients with psoriasis who are candidates for TNF antagonist therapy follows the screening standard for the general population; a TST reaction is considered positive if the induration is > 10 mm and the patient should receive LTBI treatment19.
All TNF antagonist candidates should undergo LTBI screening since an increased TB risk exists with TNF antagonist therapy. Adherence to the TB guidelines and awareness of the reasons for false-positive or negative TST results and false-negative or indeterminate IGRA results are important for more accurate LTBI diagnosis and the appropriate LTBI therapy.
Acknowledgment
The concept and outline for this article was proposed by Drs. Keystone and Papp. We thank Rose Pirone, MSc, from The Synapse Group, who provided medical writing assistance in the form of drafting and revising as per author(s) directions and in accordance with the standards of the International Committee of Medical Journal Editors.
Footnotes
-
Supported by Amgen Canada Inc. and Pfizer Canada.
- Accepted for publication February 8, 2011.








{kind=link}