

Abstract
Objective. To determine the prevalence and specificity of anticyclic citrullinated peptide antibodies (anti-CCP) and rheumatoid factor (RF) for rheumatoid arthritis (RA) in human immunodeficiency virus (HIV) infection and to evaluate the effect of immune reconstitution on these markers.
Methods. Patients with advanced HIV infection without arthritis were enrolled. CD4+ T lymphocyte counts (CD4), anti-CCP, and RF were determined before initiating antiretroviral therapy (ART) and repeated after 6 months. Results were compared to those of healthy controls. Patients were followed for the development of RA for 1 year.
Results. Sixty patients and 26 controls were studied. Six-month followup results were available on 49 patients. Mean (SD) levels of anti-CCP were higher in patients with HIV compared to controls: respectively, 9.50 (11.41) versus 0.80 (1.32) units (p < 0.001). Mean (SD) levels decreased to 4.85 (8.12) units (p = 0.006) after 6 months of ART (HIV-infected group). Fifteen percent of patients initially tested positive for anti-CCP, 4% after 6 months versus no controls (p = 0.031). Forty-seven percent of patients initially tested positive for RF, 18% after 6 months versus 8% of controls (p < 0.001). Decreases in RF and anti-CCP after ART were accompanied by increased mean (SD) CD4: from 129 (56) to 278 (140) cells/mm3 (p < 0.001). Anti-CCP and RF positivity was not associated with the development of RA.
Conclusion. Increased titers of anti-CCP and RF occur in advanced HIV infection. Although more specific than RF, before immune reconstitution, anti-CCP is an unreliable diagnostic marker for RA and does not necessarily predict future RA. After immune reconstitution, the specificity of anti-CCP approaches that of a control group.
- ANTICYCLIC CITRULLINATED PEPTIDE ANTIBODIES
- RHEUMATOID FACTOR
- HUMAN IMMUNODEFICIENCY VIRUS
- RHEUMATOID ARTHRITIS
Human immunodeficiency virus (HIV) infection is associated with a variety of rheumatic manifestations, occurring in up to 40% of infected patients1. Although these manifestations can develop at any time during the clinical course of HIV infection, they tend to appear preferentially in the later stages of the disease2.
While some manifestations are unique to HIV (diffuse infiltrative lymphocytosis syndrome, HIV-associated arthropathy, and painful articular syndrome), others include common rheumatological diseases such as rheumatoid arthritis (RA) and psoriatic arthritis that are either augmented or ameliorated by the immunosuppression1,3,4.
A frequent association with HIV infection is the presence of autoantibodies such as rheumatoid factor (RF), antinuclear antibodies (ANA), and anticardiolipin antibodies5. These autoantibodies have been documented in up to 45% of patients, usually against the background of advanced immunosuppression6,7. Although the presence of the antibodies is associated with lower CD4+ T lymphocyte cell counts (CD4) as well as an increased mortality, it does not appear to relate to the occurrence of rheumatic manifestations5,6.
The second-generation and third-generation ELISA anti-cyclic citrullinated peptide tests (anti-CCP2 and anti-CCP3) have been advocated as superior serological tests for the diagnosis of RA8. These combine an at least equal sensitivity (80%) with a superior specificity (94%–99%) compared to those of RF (80%–90%)9,10,11. The specificity has been confirmed in healthy control groups as well as in rheumatological and some nonrheumatological disease controls, but not yet in the setting of HIV infection9,12,13,14,15,16,17,18.
Considering the frequency of rheumatic manifestations in patients infected with HIV, as well as the high prevalence of autoantibodies in this population, we aimed to determine the prevalence and subsequent specificity for RA of anti-CCP in comparison to RF in patients infected with HIV as well as in a healthy control group. We also aimed to evaluate the effect of immune reconstitution on this prevalence and specificity.
MATERIALS AND METHODS
Patients and controls
The study population consisted of adult patients infected with HIV attending the Infectious Diseases Clinic at Tygerberg Academic Hospital. Our institution is a 1200-bed academic hospital in Cape Town, South Africa. It is one of 2 academic referral centers in the city and renders a tertiary service to the Western Cape population of about 1.5 million. In 2008 the HIV prevalence among antenatal women in the Western Cape was estimated at 16.1%19.
Sixty patients were studied according to the following inclusion criteria: (1) patients infected with HIV who are highly active antiretroviral therapy (HAART)-naive; (2) advanced immunosuppression (CD4 < 200 cells/mm3; World Health Organization stage 4)20; and (3) patients accepted for antiretroviral therapy (ART) according to the South African National Antiretroviral Treatment Guidelines, with inclusion into the study before commencing HAART21.
Exclusion criteria were (1) previous exposure to ART; (2) < 6 months after receiving ART for prevention of mother-to-child transmission (to exclude the possibility of immune reconstitution also described after receiving antiretroviral monotherapy)22; (3) existing rheumatological manifestations (as assessed by the attending clinician): arthralgia with early morning stiffness ≥ 30 minutes, or arthritis with any tender/swollen joints; and (4) confirmed active pulmonary or extrapulmonary tuberculosis (TB) or current use of antituberculous therapy as a possible cause of a false-positive anti-CCP23.
Patients were reviewed 3–4 times over a 1-year period for the development of RA (according to the American College of Rheumatology criteria of 1987) or any other rheumatological manifestations such as arthralgia or arthritis24. Further demographic and clinical data, such as development of active TB or other HIV-associated complications, were retrieved from patients’ hospital folders.
A control group consisted of 26 blood donors of whom sera were routinely screened to exclude HIV, syphilis, and hepatitis B virus and C virus, according to the Western Province Blood Transfusion Service Protocols. Donors were also asked to complete a questionnaire prior to inclusion, screening them for any rheumatological symptoms, chronic diseases, or the use of chronic medication that could contribute to false-positive results. Only healthy donors were included as part of the control group.
Ethical approval for the study was obtained from The Committee for Human Research of the University of Stellenbosch. Written informed consent was obtained from all subjects as well as from the controls on enrollment. The study was conducted in accordance to the Declaration of Helsinki.
Laboratory methods
In the patient group, an initial blood sample was analyzed for anti-CCP3, RF, and C-reactive protein (CRP) prior to commencing HAART, with a second analysis done after 6 months on HAART. The control group had only a single analysis. Further laboratory data, including CD4 and hepatitis studies, were retrieved from routine investigations done at the Infectious Diseases Clinic.
Serum anti-CCP3 was determined by manual standard ELISA (Inova Diagnostics kit, San Diego, CA, USA) on an Organon Technica plate reader. Results were evaluated as positive or negative as determined from a normal distribution curve (< 20 units: negative; 20–39 units: weak positive; 40–59 units: moderate positive; > 59 units: strong positive). IgG RF was determined by nephelometry (Beckman Coulter Image nephelometer; Beckman Coulter South Africa). Samples were considered positive if the antibody titer was > 11 IU/ml. CRP was determined by nephelometry. A value > 5 mg/l was regarded as abnormal.
Statistical methods
Prevalence was calculated and reported as a percentage. Specificity was determined by the percentage of true negatives (100 – prevalence). Fisher’s exact test was used to determine possible relationships between the HIV-infected and control groups. Differences of anti-CCP (and other continuous measurements) between the HIV and control groups were determined using 1-way ANOVA. Repeated-measures ANOVA using the mixed model approach was used to determine differences between pre-HAART and 6-month measurements. In all cases the assumptions for the ANOVA were confirmed with data that were normally distributed. In a single result, outliers were found to be a problem and a nonparametric Mann-Whitney U test was also reported. Spearman correlations were used to investigate relationships among continuous measurements to provide blanket protection against outliers. P < 0.05 was considered statistically significant. Data are displayed as mean ± SD.
RESULTS
The demographic data, CRP, and CD4 at the time of inclusion into the study and after 6 months of HAART are summarized in Table 1.
Demographic data. Human immunodeficiency virus (HIV) helper cell counts (CD4) and C-reactive protein (CRP) levels of the HIV group at time of inclusion and after 6 months of highly active antiretroviral therapy (HAART) and control group.
Anti-CCP
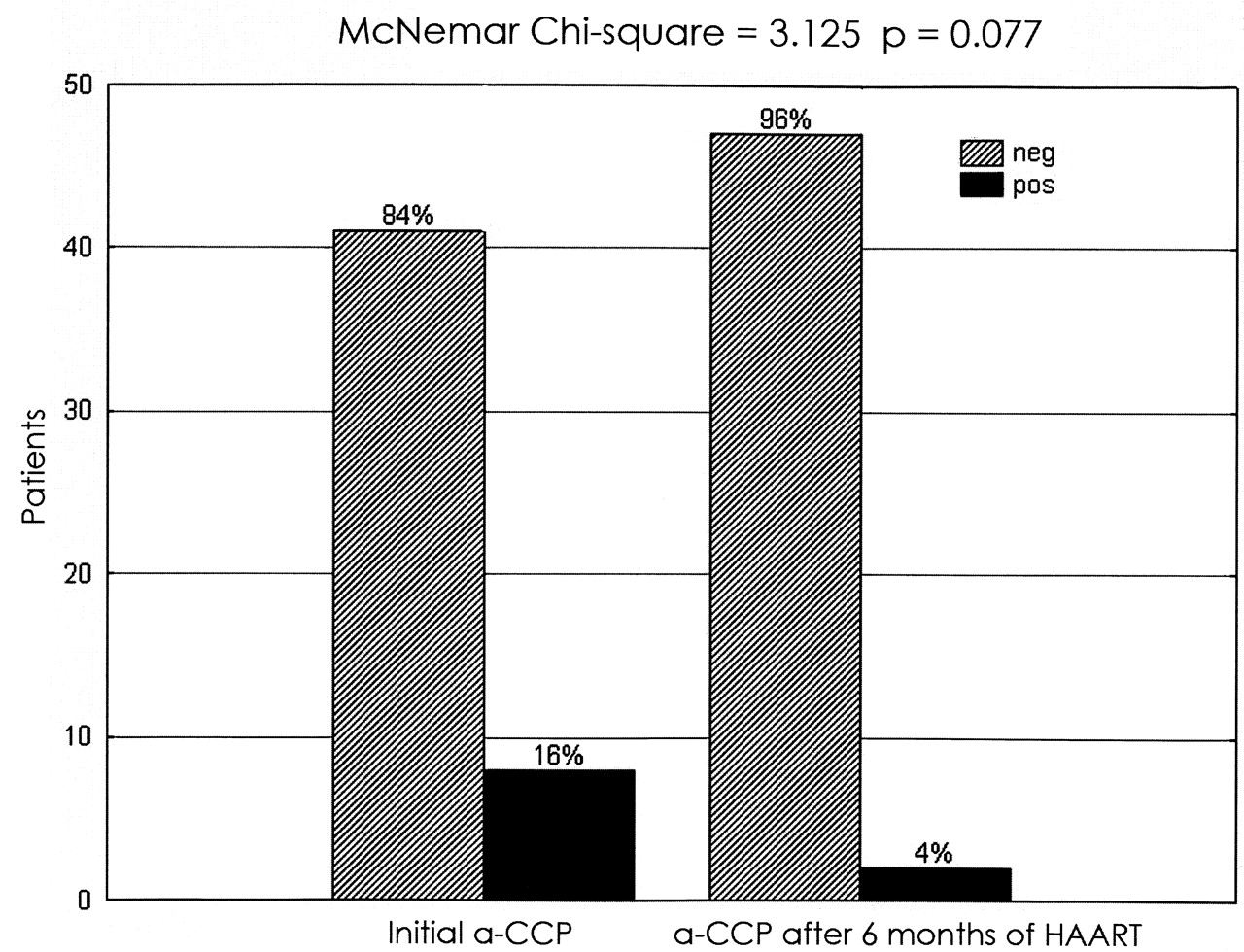
Prior to starting on HAART, patients infected with HIV had significantly higher mean (SD) levels of anti-CCP compared to the control group: respectively, 9.50 (11.41) versus 0.80 (1.32) units (p < 0.001). The mean (SD) anti-CCP levels decreased to 4.85 (8.12) after 6 months on HAART (p = 0.006). Significantly more patients infected with HIV had anti-CCP levels above the upper limit of normal compared to the control group (p = 0.031; Table 2). Of the 49 patients on which 6-month followup data were available (11 patients were lost to followup), 8 patients (16.3%) initially had anti-CCP levels above the upper limit of normal (> 20 units) compared to 2 patients (4%) after 6 months on HAART (p = 0.077; Figure 1).
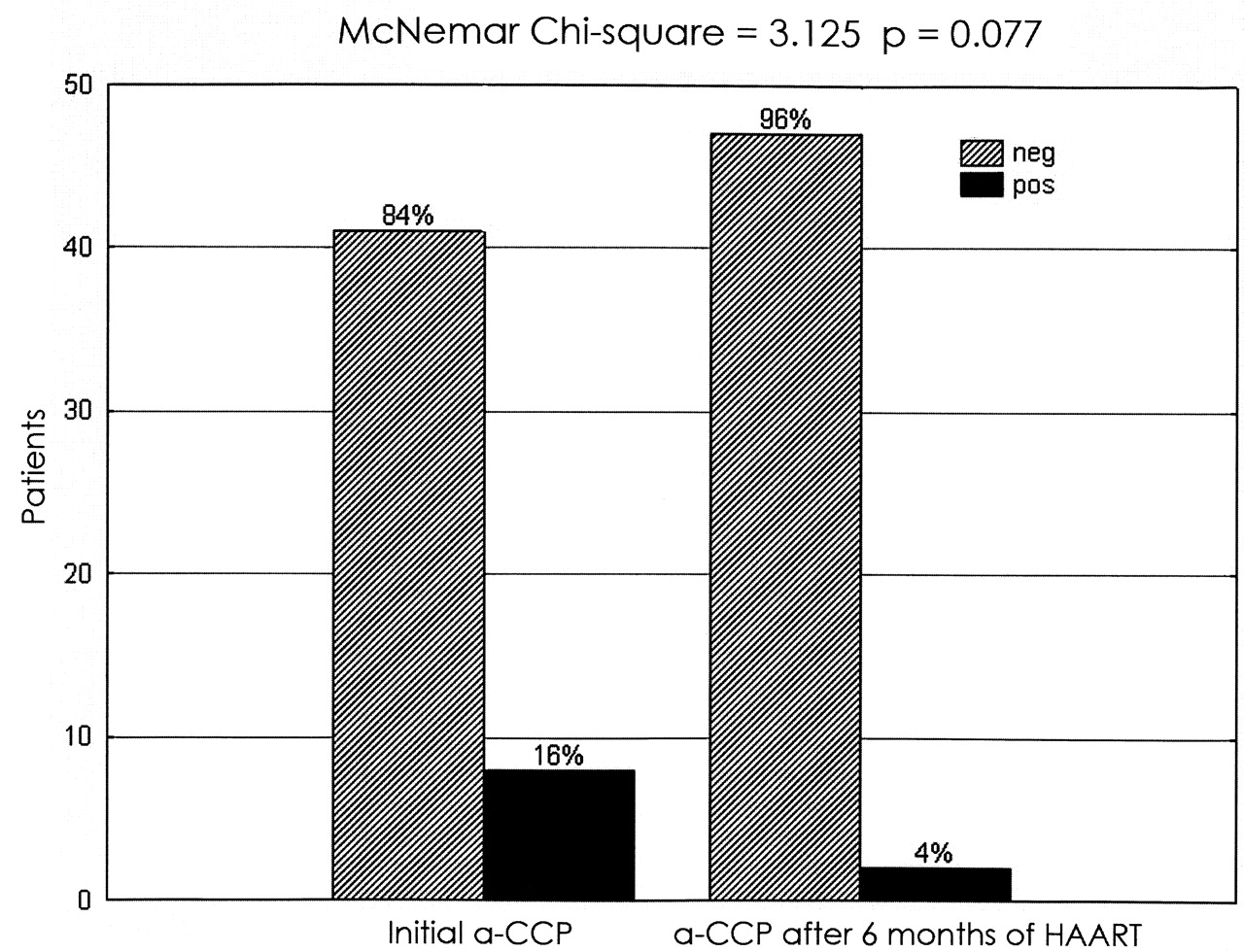
Percentage of patients with initial positive anticyclic citrullinated peptide antibodies (a-CCP; ≥ 20 units) vs after 6 months on highly active antiretroviral therapy (HAART).
Anticyclic citrullinated peptide antibodies (anti-CCP) and rheumatoid factor (RF) levels in human immunodeficiency virus (HIV)-infected patients compared to a control group.
RF measures
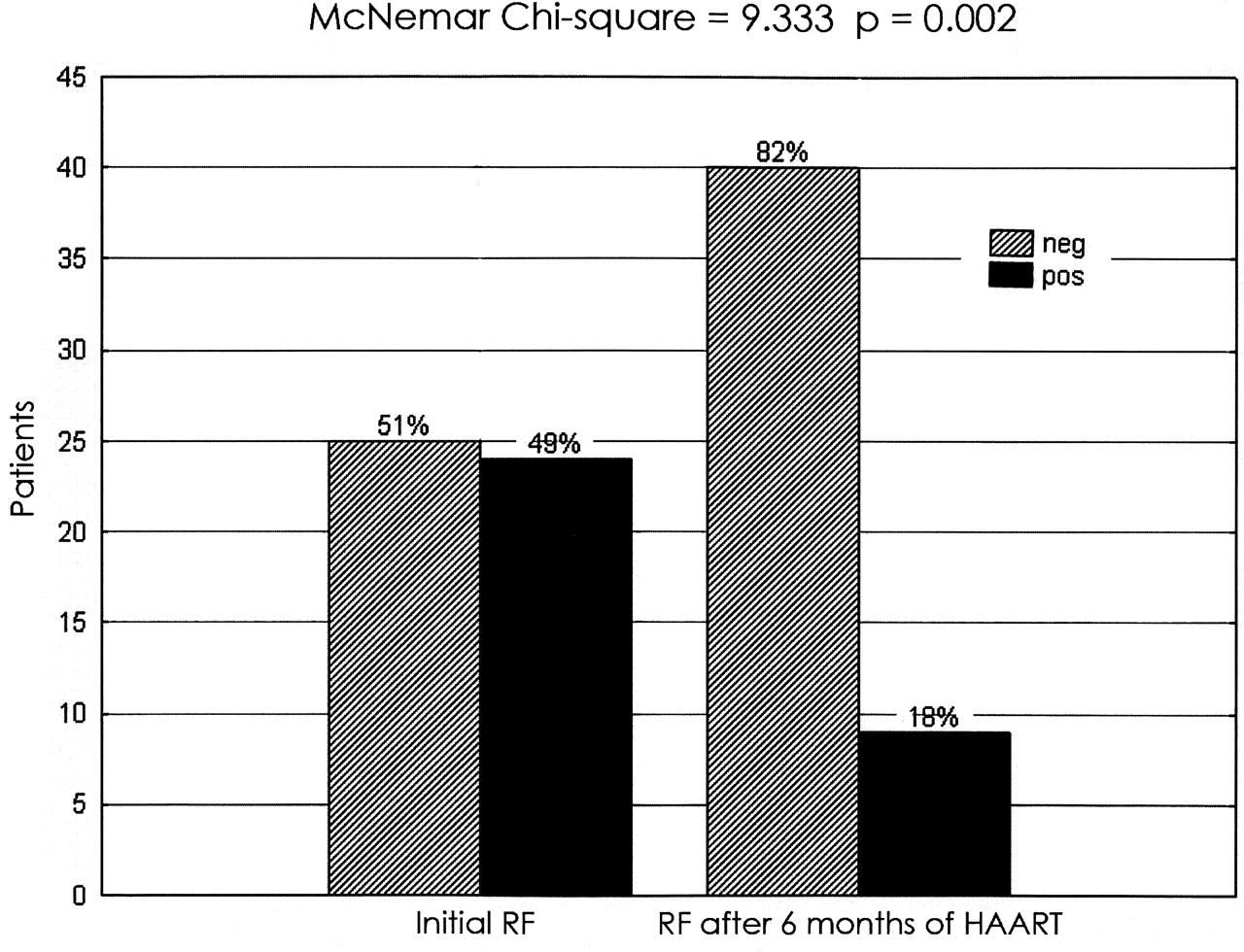
The initial mean (SD) RF was not significantly higher in the HIV patient group compared to the control group: RF 37.56 (109.86) IU versus 12.76 (9.91) IU, respectively (p = 0.26). Because of possible outliers, a nonparametric Mann-Whitney U test was also conducted that indicated a significant difference (p < 0.01). The mean value significantly decreased to 23.71 (91.13) IU after 6 months on HAART (p = 0.016). Two of the 26 controls (7.69%) had RF above the upper limit of normal (> 11 IU) compared to 28 of the 60 (46.67%) patients infected with HIV (p < 0.001; Table 2). Of the 49 patients on whom 6-month followup data were available, 24 (49%) had an initial RF > 11 IU compared to 9 patients (18%) after 6 months on HAART (p = 0.002; Figure 2).
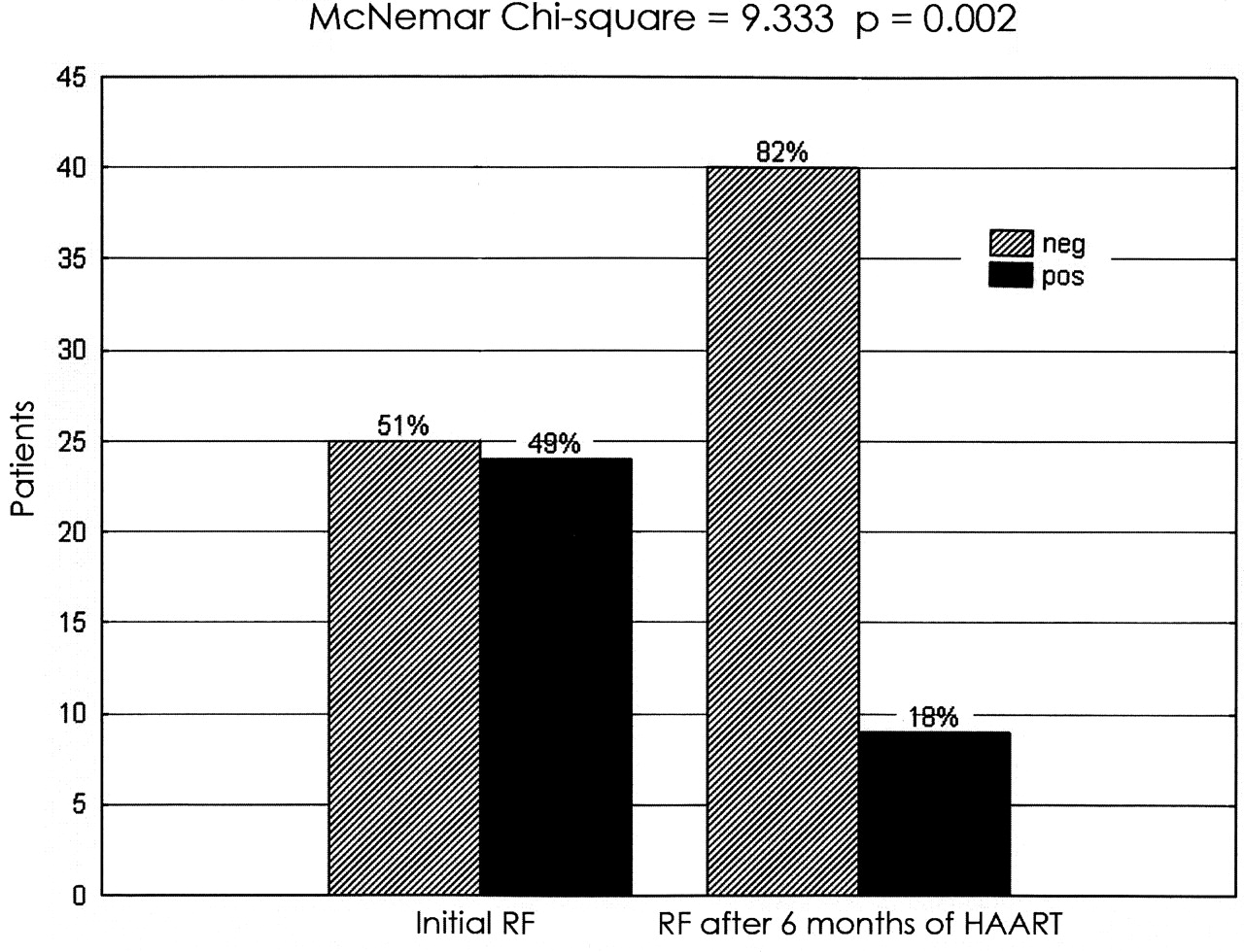
Percentage of patients with initial positive rheumatoid factor (RF; ≥ 11 IU) vs after 6 months on highly active antiretroviral therapy (HAART).
Measures of CD4
The initial mean (SD) CD4 increased significantly after 6 months of HAART: 129 (56) cells/mm3 to 278 (140) cells/mm3 (p < 0.001; Table 1). This was accompanied by significant decreases in both RF (p = 0.016) and anti-CCP (p = 0.006; Figures 3 and 4). No significant correlations were found between RF and anti-CCP, or inflammatory markers (CRP) and RF/anti-CCP.

Change in mean rheumatoid factor (RF) and CD4 levels from baseline to 6 months in patients on highly active antiretroviral therapy.
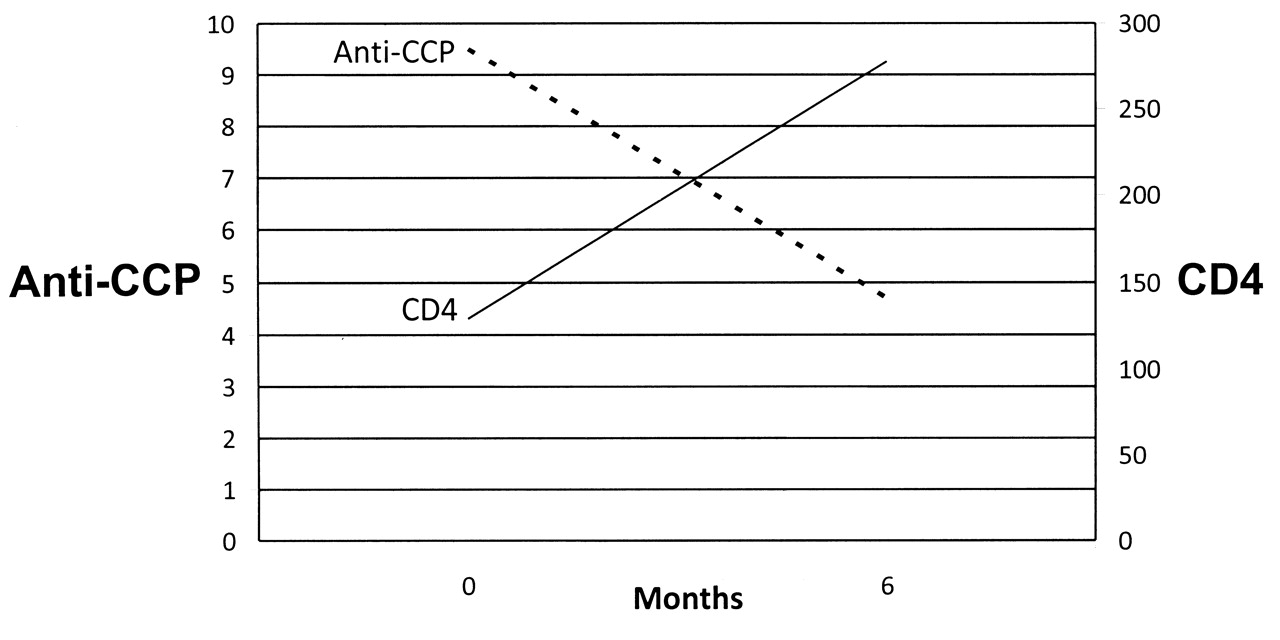
Change in mean anticyclic citrullinated peptide antibody (a-CCP) and CD4 levels from baseline to after 6 months in patients on highly active antiretroviral therapy.
Clinical correlations
Two patients in the study group developed a self-limiting oligoarthritis. Both patients had persistently negative anti-CCP levels, with one of the 2 patients developing a low-positive RF (23 IU) after 6 months on HAART.
Four patients in the study group had active hepatitis B virus infection without any associated rheumatological manifestations. All 4 patients had RF > 11 IU including the highest RF in the group (853 IU). One of the 4 patients had a positive anti-CCP level of 47 IU, also the highest documented in the group. None of the patients had hepatitis C virus infection.
There were no significant correlations between RF/anti-CCP and the type of HAART used or whether a patient had previously been treated for Mycobacterium tuberculosis. A single patient developed pulmonary TB during the followup period. This patient had a negative anti-CCP and RF of 47 IU.
DISCUSSION
To our knowledge, this is the first study to look at the prevalence and specificity of anti-CCP in the setting of advanced HIV infection. We have found that 15% of patients infected with HIV had a false-positive anti-CCP compared to none of the control group (Table 2).
After 6 months of HAART, recovery of the immune system as documented by an increase in the CD4 was associated with a decrease in anti-CCP levels (Figure 4). However, elevated anti-CCP levels did not coincide with or predict the development of RA, neither during immune reconstitution nor for the duration of the study.
The rheumatological manifestations associated with HIV infection are diverse in origin and pathogenesis. Early reports suggested that CD4-driven conditions such as RA and systemic lupus erythematosus (SLE) might go into remission in the face of advanced HIV infection4,25. In the era of HAART it is therefore not surprising to find reports of the de novo development of RA and SLE as part of an immune reconstitution syndrome26,27,28. Our study neither confirmed nor refuted those reports.
Our findings are in keeping with current knowledge of other autoantibody production due to immune dysregulation in advanced HIV infection, e.g., RF, ANA, and anticardiolipin antibodies5. The presence of autoantibodies typically occurs in the setting of lower CD4 and is associated with an increased mortality, implying prognostic significance in the context of HIV infection6. These autoantibodies, however, tend not to relate to the occurrence of rheumatic manifestations in advanced HIV infection5,6.
The specificity of the second-generation and third-generation anti-CCP in the diagnosis of RA has been well documented in a wide spectrum of rheumatological and nonrheumatological diseases9,12,13,14. With regard to infectious diseases, however, studies have mainly focused on hepatitis C and B as well as subacute infections such as bacterial endocarditis, where anti-CCP, in contrast to RF, continues to be a useful discriminative test15,16,17. We had a total of 4 patients with concomitant hepatitis B virus and HIV infection. Although not sufficient for any statistical conclusions, we find it interesting that all 4 patients had a positive RF and only 1 had a positive anti-CCP. Also of note is that both the highest RF and anti-CCP were documented in patients with concomitant hepatitis B infection, highlighting the problem of interpreting serology, especially RF, in the setting of chronic infections.
Elkayam and colleagues have recently shown that 32% of patients with pulmonary TB have significantly increased anti-CCP levels, prior to the initiation of antituberculous therapy23. This prompted our question regarding the specificity of anti-CCP in the setting of HIV, a common coinfection in South Africa and a disease known for the production of autoantibodies5,19.
We have subsequently demonstrated that 15% of patients with advanced HIV infection in the absence of rheumatological manifestations, specifically RA, have a false-positive anti-CCP (Table 2). Treatment with HAART and recovery of the dysregulated immune system was reflected by results (4% false-positive; Figure 1) comparable to what is seen in other chronic diseases18.
An unexpected result was the high frequency (46.67%) of false-positive IgG RF found pretreatment with HAART (Table 2). Massabki, et al reported a frequency of only 8% in a group of patients with HIV infection6. Mean CD4 (cells × 106) in this study population was 231 (SD 213) compared to 129 (cells/mm3; SD 56) in our group. The RF isotype was also not specified in this study6, making further comparison difficult. In a study by Procaccia and colleagues7, patients with advanced HIV infection (CD4 < 200) had a 25% false-positive rate of IgG RF, again much lower than our own findings. Different methodology, i.e., a variation of the ELISA versus nephelometry used in our laboratory, could in part explain the differences in results.
Our study had the following limitations: We interpreted anti-CCP levels according to a normal distribution curve. The majority of our patients (6 out of 60) had weak positive anti-CCP (20–39 units); 3 patients had a moderately positive result (40–59 units), and no patient a strongly positive result (> 59 units). Had we considered only moderately positive as significant, the specificity of anti-CCP would have been considerably higher, at 95%.
A further caveat is our relatively short followup period of 1 year. Preclinical RA studies by Nielen, et al, and Rantapää-Dahlqvist, et al, have shown that anti-CCP positivity may precede the development of RA by several years (median 5.3 years)29,30. A more recent study by Chibnik, et al also emphasized the increased sensitivity of even low titers of anti-CCP in predicting the future development of RA31. The significance of the persistently abnormal anti-CCP levels (1 low-positive and 1 moderately positive) in 2 of our patients on HAART therefore remains undetermined.
We have shown that a significant proportion of patients with advanced HIV infection have low to moderately raised titers of anti-CCP prior to treatment with HAART. Positive titers of anti-CCP occurred in the absence of an associated inflammatory arthritis and did not predict the development of RA. Although more specific than RF, our results stand in contrast to the previously documented specificity and discriminative value of anti-CCP in other viral infections such as hepatitis B and hepatitis C. Our findings have important implications for the interpretation of anti-CCP results in patients infected with advanced HIV who present with rheumatological manifestations. The determination of specificity of different titers of anti-CCP in the setting of chronic diseases such as HIV may be important in the interpretation of anti-CCP as a discriminative test.
Acknowledgment
The authors thank Prof. Martin Kidd (The Centre for Statistical Consultation, University of Stellenbosch) for his assistance with statistical analysis of study data. We also thank Noel Nel, laboratory manager, and the staff of the Immunology Laboratory, Tygerberg Hospital, for their excellent service. We thank our colleagues from the Infectious Diseases Clinic for their help with recruitment of patients and the Western Province Blood Transfusion Service for recruitment of our control group.
Footnotes
-
Supported by The Harry Crossley Foundation, Research Development and Support, Tygerberg Hospital, University of Stellenbosch, South Africa, and the K-Project Research Grant, National Health Laboratory Services, Johannesburg, South Africa.
- Accepted for publication December 8, 2010.








{kind=link}
{kind=link}
{kind=link}
{kind=link}