

Abstract
Objective. To compare health-related quality of life (HRQOL) of patients with antiphospholipid syndrome (APS) and systemic lupus erythematosus (SLE) with and without previous thrombovascular events (TE).
Methods. The Medical Outcomes Study Short-Form 36 (SF-36) was used to assess HRQOL in 5 patient groups: (1) primary APS (PAPS; n = 35); (2) APS associated to SLE (SAPS; n = 37); (3) SLE+TE without persistent positive antiphospholipid antibody (SLE+TE–aPL; n = 75); (4) SLE–TE+aPL (n = 71); and (5) SLE–TE–aPL (n = 608).
Results. The data on both mental component summary and physical component summary (PCS) scores showed an impaired quality of life in all patient groups. Patients in the SLE+TE–aPL group had a lower PCS score compared to patients in the SLE–TE+aPL group.
Conclusion. The combination of SLE and TE has a more negative influence on reported HRQOL, compared to having SLE or APS alone.
Health-related quality of life (HRQOL) is an important outcome in clinical care, as it measures patient’s perspective of the effects of disease. In systemic lupus erythematosus (SLE), disease activity and damage over time can be poor predictors of HRQOL1. HRQOL measures may provide information about the disease burden not revealed by traditional measures of illness2,3.
SLE is a chronic inflammatory condition that may result in damage to multiple organs, joints, and skin. Patients with SLE are comparable to individuals with other common chronic diseases such as congestive heart failure, rheumatoid arthritis, and Sjogren’s syndrome, but at an earlier age4 they report significantly worse HRQOL that persists over time5.
The antiphospholipid syndrome (APS) is defined by 2 significantly positive antiphospholipid antibody (aPL) tests, 12 weeks apart, and the presence of a clinical event, i.e., either a thrombovascular event (TE) or a defined obstetrical complication6. Studies examing patients’ HRQOL following TE, such as deep vein thrombosis with its accompanying symptoms of acute leg swelling and pain, have shown adverse influences on the HRQOL, compared to the general population7,8.
The objective of our study was to describe the HRQOL of patients with: (1) primary APS; (2) secondary APS in patients with SLE; (3) SLE and TE in the absence of aPL; (4) SLE with aPL and no TE; and (5) SLE without TE or aPL.
MATERIALS AND METHODS
Five groups of patients from the University of Toronto SLE and APS out-patient clinics, affiliated with the Centre for Prognostic Studies in the Rheumatic Diseases, were selected for study: (1) primary APS (PAPS) as defined by the revised Sydney criteria6; (2) APS associated to SLE (SAPS); (3) SLE with a previous TE without aPL (SLE+TE–aPL); (4) SLE without previous TE, but with persistently positive aPL defined as positive lupus anticoagulation and/or anticardiolipin antibody of IgG and/or IgM > 40 units, on 2 or more occasions, at least 12 weeks apart (SLE–TE+aPL); and (5) SLE without TE and without aPL (SLE–TE–aPL). All patients with SLE met at least 4 or more of the 1971 or 1982 American College of Rheumatology (ACR) classification criteria9, or 3 ACR criteria plus having a diagnostic histological lesion of SLE (on renal or skin biopsy)10.
Age, sex, and type of TE were documented. HRQOL was determined using the Medical Outcomes Study Short-Form 36 (SF-36) at the most recent visit. The SF-36 is widely used and evaluated as a generic HRQOL measurement tool, and has been recommended as the HRQOL instrument for SLE11,12. The SF-36 is a self-administered questionnaire to assess 8 subscales of HRQOL: bodily pain, general health, mental health, physical function, role-emotional, role-physical, social function, and vitality. These subscales are differently weighted to compute a mental and physical component summary score. Subscale scores range from zero to 100, higher scores representing a better QOL. Summary scores less than 48 are considered to represent impaired QOL.
Statistical analysis was performed using SPSS version 16 (SPSS Inc., Chicago, IL, USA). The mental component summary (MCS) and physical component summary (PCS) scores were normalized to Canadian age and gender means. Spearman correlations were performed between summary scores and time duration between TE and HRQOL administration. We used one-way ANOVA with Bonferroni post-hoc tests to compare HRQOL scores, across the 5 groups. Statistical significance was defined as p < 0.05.
RESULTS
At study entry, mean age was similar across groups except for a significantly younger average age (mean 42.6 ± SD 15.2 yrs) in the SLE–TE–aPL group compared to the other 4 groups (Table 1). A majority of the patients were female in all groups, except for a significantly smaller proportion of women (p < 0.05) in the PAPS group. Patients in the SAPS group had significantly less venous TE (more arterial TE) compared to those in the PAPS and SLE+TE–aPL groups (p < 0.05; Table 1).
Demographic characteristics and health-related quality of life measures; results are reported as mean ± SD or percentage. Mental component summary score (MCS) and physical component summary score (PCS) are adjusted for age and sex. A clinically relevant difference is defined as a minimum MCS or PCS difference of 513.
All patients with TE (PAPS, SAPS, and SLE+TE) had similar PCS and MCS scores compared to all those without TE (SLE–TE+aPL and SLE–TE–aPL) (p > 0.05; Table 1). There was no correlation between these summary scores and time duration from time of TE to administration of HRQOL questionnaire (p > 0.05).
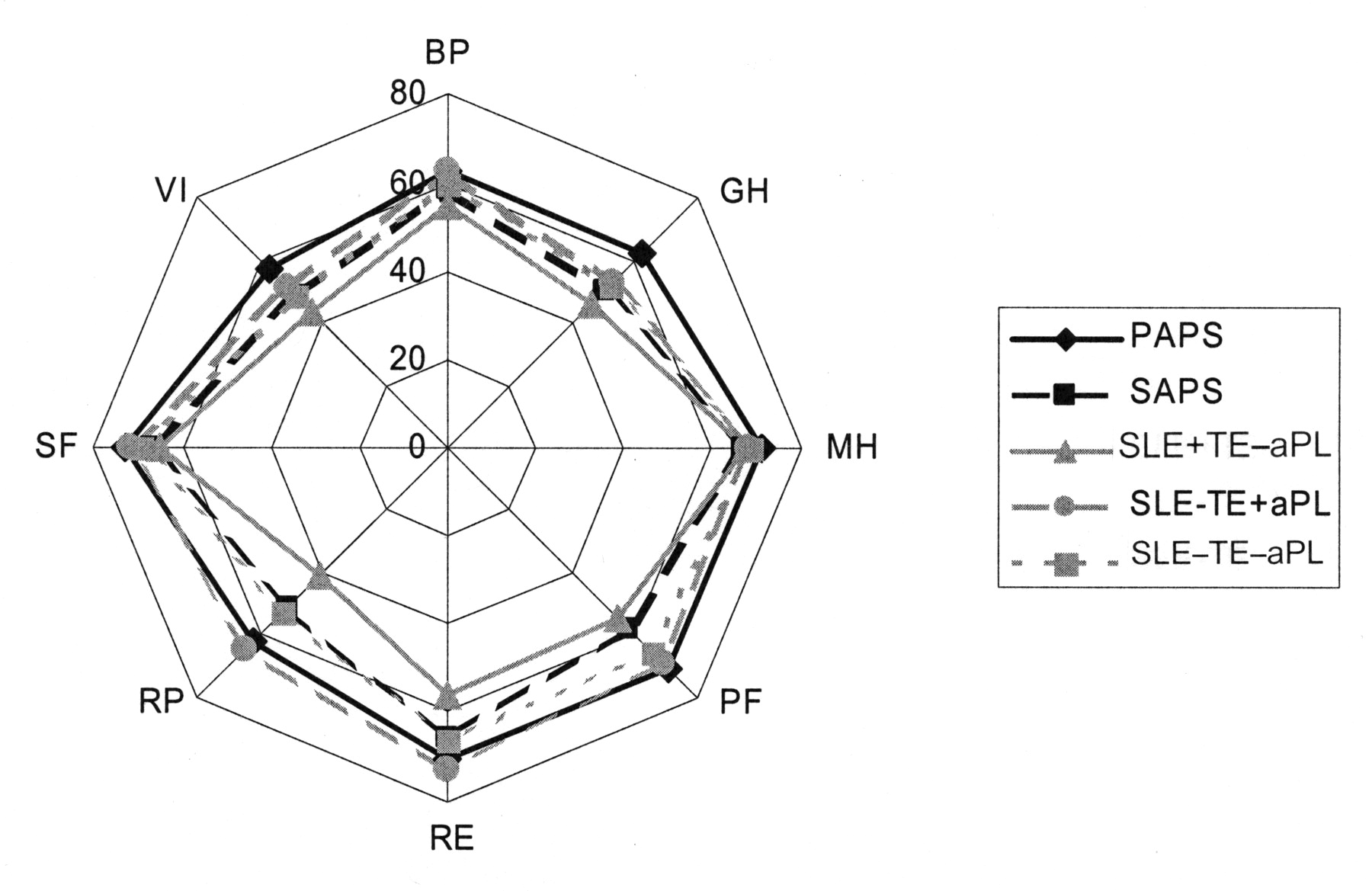
The data on both MCS and PCS scores showed an impaired QOL in all patient groups (Table 1). There was no difference in MCS scores across groups (p > 0.05). However, patients in the SLE+TE–aPL group had a lower PCS score compared to patients in the SLE–TE+aPL group (Table 1; p < 0.05). Patients in SLE+TE–aPL also scored significantly lower on a number of subscales such as general health, physical health, and physical function (Figure 1; p < 0.05).

Comparison of mean Short-Form 36 (SF-36) scores of patients; each spoke on the plot represents a sub-scale of the SF-36. Data points closer to the outside edge represent a better HRQOL, compared to points closer to the center. The data show that the SLE+TE–aPL group has the worst HRQOL as the triangles with solid gray lines are all closer to the center. Similarly, the SAPS group is close behind. BP: bodily pain; GH: general health; MH: mental health; PF: physical function; RE: role-emotional; RP: role-physical; SF: social function; VI: vitality.
DISCUSSION
Our study demonstrated that all patients with SLE and/or APS with and without previous TE have impaired mental and physical health affecting their HRQOL. Interestingly, patients with and without TE did not differ in their reported HRQOL. However, a combination of 2 severe conditions, such as SLE and TE, was found to have the most impact on the physical health of the affected patients, an effect that was not related to the type of TE or the age of the patients.
The findings of this study are in accord with others reporting impaired PCS and MCS scores in patients with SLE4,5 and/or in patients with TE14. However, this is the first study comparing the HRQOL of patients with primary and secondary APS and SLE in the presence and absence of previous TE.
This study had some limitations. First, more arterial events were reported in the SAPS and SLE+TE groups than in the PAPS groups, providing a possible explanation for the better reported HRQOL in our PAPS group. Second, we cannot explain why the HRQOL of the SAPS group did not differ from that of the SLE–TE groups. It may be that more patients in the SAPS group are needed to show a difference with the SLE–TE groups. Another explanation may be that the TE related to SAPS and the TE that occurred in SLE+TE–aPL group are different qualitatively and that they affect the HRQOL reporting differently, with SLE+TE–aPL reporting worse HRQOL than SAPS groups because of having had TE, with worse consequences for the patients’ HRQOL. We could not study this qualitative dimension in our patients. Third, QOL measures do not correlate well with disease activity scales such as the SLE Disease Activity Index (SLEDAI)15. It may be misperceived that more disease is associated with worse quality of life. This is not always the case.
Patients with both primary APS and SLE with and without thrombovascular events have impaired HRQOL; and the combination of SLE plus thrombovascular events has the most impact on patients’ physical health.
Footnotes
-
Supported by the Kirkland Scholar Award Program at the Hospital for Special Surgery, New York, New York; and by Rheuminations, Inc. Dr. Fortin is a Distinguished Senior Investigator of The Arthritis Society with additional support from the Arthritis Centre of Excellence, University of Toronto. A.K. Balitsky is supported by the CREMS (comprehensive research experience for medical students) program at the University of Toronto. CaNIOS is supported in part by Lupus Canada, Lupus Ontario, the Lupus Foundation of Ontario, BC Lupus, and the Arthritis and Autoimmune Research Centre Foundation. The Centre for Prognostic Studies in Rheumatic Disease – University of Toronto Lupus Clinic is supported by The Smythe Foundation, Lupus Ontario, and the Dance for the Cure, the Flare for Fashion and the Lupus Foundation of Ontario.
- Accepted for publication January 13, 2011.








{kind=link}