

Abstract
Objective.To describe the evaluation of a community-based continuing health education program designed to improve the management of rheumatoid arthritis (RA) and osteoarthritis (OA), and to examine the results by discipline.
Methods.The Getting a Grip on Arthritis© program was based on clinical practice guidelines adapted for the primary care environment (best practices). The program consisted of an accredited inter-professional workshop and 6 months of activities to reinforce the learning. Analyses compared best practice scores derived from responses to 3 standardized case scenarios (early and late RA; moderate knee OA) at baseline and 6 months post-workshop using the ACREU Primary Care Survey.
Results.In total, 553 primary care providers (nurses/licensed practical nurses 30.9%, rehabilitation professionals 22.5%, physicians 22.5%, nurse practitioners 10.9%, other healthcare providers/non-clinical staff/students 13.1%) attended one of 27 workshops across Canada; 275 (49.7%) completed followup surveys. Best practice scores varied by discipline at baseline (p < 0.05) and improved for all 3 case scenarios, with nurse practitioners and rehabilitation therapists improving the most (p ≤ 0.05).
Conclusion.Results suggest that inter-professional education may be an effective method for dissemination of guidelines and has potential to improve the delivery of arthritis care, particularly when nurse practitioners and rehabilitation therapists are involved in the care of patients.
- ARTHRITIS
- PRACTICE GUIDELINES
- CONTINUING MEDICAL EDUCATION
- PRIMARY CARE
- LONGITUDINAL STUDIES
- EVIDENCE-BASED MEDICINE
Arthritis and related conditions affect over 4.4 million Canadians aged 15 years and older, and in 2005–2006 accounted for close to 9 million physician visits1. Most treatment for people with arthritis occurs at the primary care level, yet many studies have documented the need for improved arthritis management in this environment2,3. Challenges for primary healthcare providers include difficulty in diagnosing arthritis, delay in referring to specialists, and underutilization of nonpharmacological interventions4,5,6,7,8. Dissemination of clinical practice guidelines has been suggested as one method for improving care delivery; however, the literature on continuing health education interventions for the implementation of arthritis guidelines in primary care is scarce and primarily targets physicians9. Successful strategies have included educational outreach by peer educators10 and multifaceted peer-facilitated workshops11,12.
Getting a Grip on Arthritis© is a multifaceted education program targeting primary healthcare providers. The program incorporates constructs from social cognitive theory13 to support behavior change, including credible peer models (local multidisciplinary arthritis specialists), skill development, demonstration and feedback, goal setting, enhancing self-efficacy, addressing barriers, and providing reinforcement. The program, designed to disseminate arthritis best practices based on guidelines for the management of osteoarthritis (OA) and rheumatoid arthritis (RA)12, was successfully pilot tested in community health centers in Ontario, Canada, and showed improved provider confidence and satisfaction in managing arthritis, improved patient education, and increased referrals to rehabilitation specialists. Following the pilot, the program was implemented nationally14, which provided a unique opportunity (1) to evaluate whether this community-based educational program was successful in improving outcomes in a variety of primary care settings including those with fee for service providers; and (2) to examine outcomes based on the discipline of the participants. This report describes the evaluation of the national program and the lessons learned in implementation.
MATERIALS AND METHODS
The Getting a Grip on Arthritis (Grip) program consisted of an accredited inter-professional workshop on the evidence-based management of OA and RA and 6 months of reinforcement activities to support the delivery of arthritis care in the community12,14. Briefly, primary healthcare organizations were invited to register relevant healthcare providers for a Grip workshop in their community or region.
Twenty-seven one-day workshops were delivered across Canada. Faculty consisted of local multidisciplinary arthritis specialists (rheumatologists, dietitians, physical and occupational therapists, social workers, pharmacists) who received standardized training and materials. Content emphasized the early identification and differentiation of arthritis, pharmacological and nonpharmacological care, self-management support, and appropriate referral to specialists and The Arthritis Society, a national nonprofit organization providing education, resources, community linkages and support for people with arthritis in Canada. Hands-on skills were developed through a review of the musculoskeletal examination with trained patient educators15. At the end of the day, participants met in facilitated small-group sessions to discuss implementation of best practices. Participants then returned to their worksites with plans for implementing arthritis best practices and personal goals to change their practice.
Reinforcement activities during the 6 months post-workshop included educational materials for staff and patients (available in French and English at www.arthritis.ca/gettingagrip), posters, referral templates, community resource lists, and followup of personal goals established at the workshops. Providers could also request additional training and resources to support the delivery of arthritis best practices in their communities.
Evaluation
Evaluation of the workshop participants took place at baseline and 6 months post-workshop using a modified version of the Arthritis Community Research and Evaluation Unit (ACREU) Primary Care Survey used previously in the evaluation of primary healthcare providers4,5. The survey is available on request from the authors. The survey asked participants to indicate what interventions and referrals (best practices) they would recommend for 3 case scenarios depicting patients with typical early and late RA and moderate knee OA (primary outcome). As an example, the early RA case scenario is given in the Appendix. Open-ended responses were coded independently by 2 trained coders using a coding manual as a guide. The description and the scoring of the best practices for each of the 3 case scenarios are outlined in Table 1. One point was given for each best practice and summed for a total best practices score for each case.
Scoring of arthritis best practices for 3 case scenarios [moderate knee osteoarthritis (OA), early and late rheumatoid arthritis (RA)].
The survey also included questions on perceptions of barriers to physiotherapy, occupational therapy (OT), social work, or rheumatology (0 = no barriers; 1 = barriers, i.e., waiting time unacceptable, travel time unacceptable, no confidence in service, funding barrier, not available, not sure if available). Confidence in the management of arthritis and satisfaction with their ability to deliver arthritis care were measured on a 10 point numerical rating scale (1 = not at all confident/satisfied to 10 = extremely confident/satisfied).
The project received ethics approval from the University of Toronto, Health Canada, and relevant provincial, regional, university and hospital ethics boards across Canada.
Analysis
Descriptive statistics were used to describe organization and provider characteristics at baseline, and appropriate nonparametric and parametric tests were used to compare characteristics of the participating sites and providers to dropouts. Repeated-measures ANOVA was used to determine the within-subject change in outcomes controlling for baseline use of best practices for each case scenario. Statistical analyses were performed using SAS, version 9.1. A p value < 0.05 was considered statistically significant and an improvement over baseline ≥ 15% was considered a clinically important change16. It was not possible in this project to determine sample size a priori.
RESULTS
Organization and provider recruitment
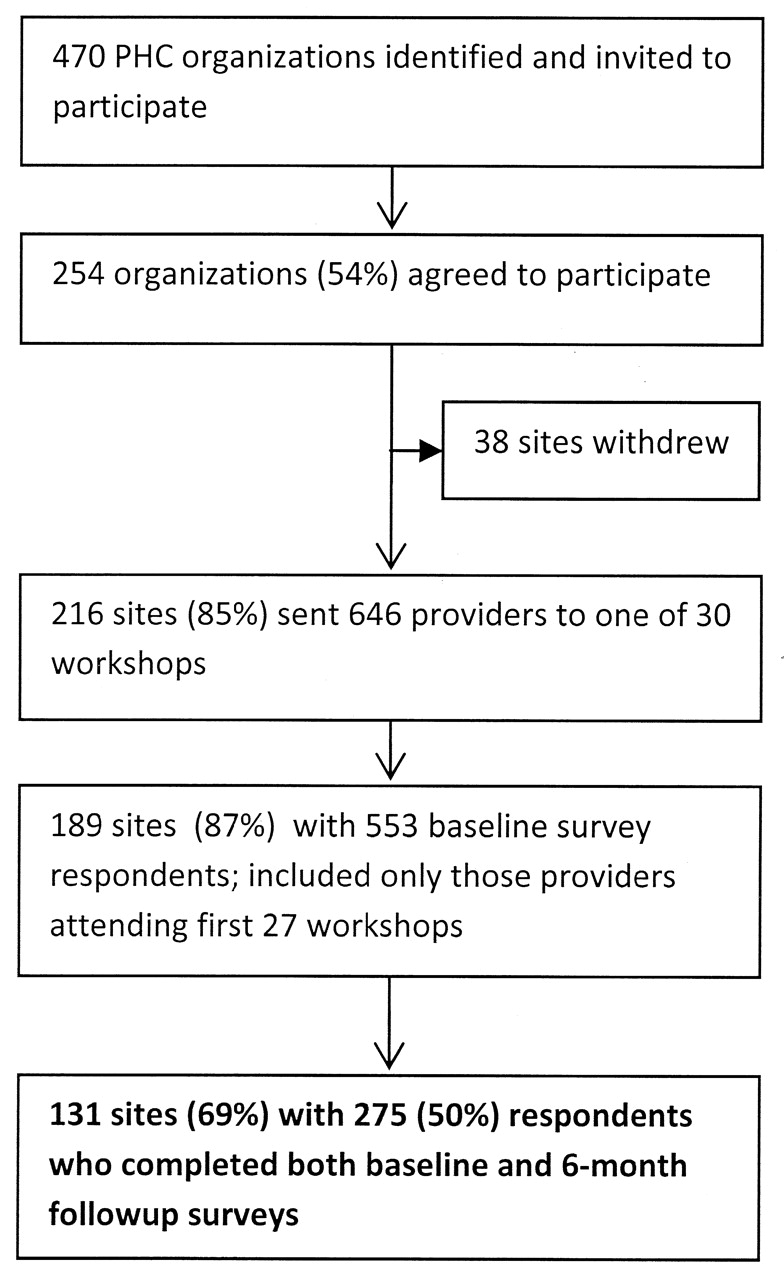
Figure 1 illustrates the recruitment of organizations and providers participating in the Grip program. Four hundred seventy primary healthcare organizations in 10 provinces were identified that treated adults with arthritis, and 254 (54.0%) accepted the invitation to participate in the program. The evaluation study included 553/646 (86%) healthcare providers from 189 sites who completed baseline surveys. At 6 months post-workshop, 275 providers from 131 sites completed followup surveys, a 49.7% response rate. Participating sites represented 4 different models of primary healthcare delivery, specifically community health centers/centres de santé et de services sociaux (45.0%), regional models (35.9%), physician networks (groupes de medicine de famille, family health networks, family health groups, primary care networks; 11.5%), and federally funded sites (7.6%). The latter were not a specific target of the intervention. The regional models and physician networks include fee-for-service physicians.

Recruitment of primary healthcare (PHC) organizations and providers.
Workshop participants were primarily English speaking (84.0%) and female (82.6%) and represented multiple disciplines [nurses/licensed practical nurses 30.9%, rehabilitation professionals (physiotherapists and occupational therapists) 22.5%, physicians 22.5%, nurse practitioners 10.9%, other healthcare providers/nonclinical staff/students 13.1%]. There were no statistically significant differences between participants who responded at 6 months and those who failed to respond in terms of mean age, gender, language, urban/rural status, discipline or model of care; however, the response rate was highest in the Ontario region (data not shown; p < 0.01).
All participating sites received at least one reinforcement activity following the workshop, as reported in detail14. Of the 131 sites that responded at 6 months, many requested additional support by ordering project materials for their patients (60.2%) or providers (39.8%), arthritis books and videos for donation to their local libraries (44.4%), or additional staff training or resources (14.4%).
As shown in Table 2, baseline best practice scores for all 3 case scenarios were low and varied by provider discipline (Kruskal-Wallis test, p < 0.05). There were significant improvements in total best practices scores at 6 months post-workshop, with nurse practitioners and rehabilitation therapists improving the most (p < 0.05).
Total best practices scores at baseline and 6 months post-workshop for early and late RA and moderate knee OA based on discipline (n = 275). Best possible score is 7 for early RA and 8 for late RA and moderate knee OA.
Table 3 provides the percentages of participants choosing each individual best practice for each case scenario at baseline and at 6 month followup. There were significant (p < 0.05) and clinically important (> 15%) improvements in the selection of several individual best practices for early RA (education, OT/joint protection, psychosocial support, and referral to rheumatology). Recommendations for non-steroidal antiinflammatory drugs (NSAID) decreased significantly for both early and late RA (30%). For late RA, there were also improvements in recommendations for education, OT/joint protection, psychosocial support, and disease-modifying antirheumatic drugs (DMARD). For moderate knee OA, there were improvements in recommendations for education and weight management/healthy eating. The proportion of providers recommending weight management or healthy eating more than tripled.
Percentage (number) of providers recommending specific interventions at baseline and 6 months for 3 case scenarios (n = 275).
At baseline, participants reported moderate satisfaction and confidence with several aspects of arthritis care. Most participants reported one or more barriers to access a rheumatologist (91.6%), occupational therapy (71.7%), physiotherapy (77.5%), and social work (76.8%; Table 4). At 6 months post-workshop, there were significant improvements in satisfaction and confidence (p ≤ 0.05). Perceptions of barriers to all services decreased substantially (p < 0.01).
Comparison of providers at baseline and at 6 months followup: satisfaction, confidence, and perceived barriers.
DISCUSSION
This study was the first to evaluate a national inter-professional education program designed to improve arthritis care in the community; and showed modest improvements in adherence to recommendations for arthritis best practices. Clinically important improvements in best practice scores were seen for both the early RA and moderate knee OA cases (17% for both). This change was greater than the 10% median improvement reported by Grimshaw, et al in a large review of the effectiveness and efficiency of guideline implementation strategies17. Improvements were also seen in satisfaction and confidence in managing arthritis, which might result in more frequent use of best practices. Given the high prevalence of arthritis in primary care practices, this could result in improved outcomes at a population level18. These results also extend the generalizability of the results of the Getting a Grip on Arthritis pilot study beyond the community health centers12 to other primary care models including those that incorporate fee-for-service physicians. Inter-professional education is seen as important for supporting team-based care and influencing behavior change19,20,21,22,23, and this study adds to the literature suggesting that it may be an effective strategy for improving delivery of care24.
This was also the first Canada-wide study to examine and describe differences in the primary care management of arthritis based on discipline. Results varied by type of provider, with nurse practitioners and rehabilitation therapists improving the most. Although there was a trend, it is unclear why physicians’ recommendations for best practices did not improve significantly. Glazier, et al5, in a study of family physicians using the same survey, found that referrals tended to be low for early and late RA, and the authors suggested that physicians might wait for test results before referring. In addition, in organizations where other members of the team are available, roles may be more delineated and physicians may leave nonpharmaceutical management to others. Further studies may elucidate these issues.
The improvement in the proportion of providers recommending education for all 3 case scenarios and OT/joint protection and psychosocial support for RA is encouraging. This has potential to improve pain, functional outcomes, and coping for people with arthritis25,26,27. Surprisingly, there were no improvements in recommendations for physiotherapy/exercise for any of the case scenarios, or for occupational therapy for OA. This may have been due to providers referring to The Arthritis Society (coded as an education best practice) assuming patients would then be connected with the resources and services they needed.
The significant increase in the proportion of providers who recommended referrals to rheumatology for early RA is particularly promising, given new guidelines recommending early referral for this population, preferably within 3 months of symptom onset28,29. There was a 30% increase in referral to rheumatology for late RA as well, although this change was not significant and still remained low overall. There was also a significant and clinically important increase in recommendations for DMARD for late RA. For early RA, there may have been diagnostic uncertainty and providers may have been reluctant to initiate DMARD until a diagnosis had been confirmed. The decrease in recommendations for NSAID may have been because the case scenarios specifically indicated that a course of NSAID had been tried without success. This change, if made judiciously, has potential to reduce healthcare costs and potential patient side effects30. Referral to orthopedics, a best practice for late RA, was low. Guidelines for orthopedic referrals were not discussed in the workshops, and need to be included specifically in future interventions.
Even though the moderate knee OA scenario did not specifically indicate that the patient was overweight, there was an improvement in recommendations for weight management and healthy eating at followup. Messages around weight management and proper nutrition were discussed as important during the workshop regardless of weight, since obesity is a risk factor for onset and greater pain in knee OA31,32,33. Weight loss may be an important preventive strategy for OA and has potential to reduce disability, progression of OA, and future need for joint replacement34. We failed to find improvements in recommendations for intraarticular injections for OA. This may have been due to the mild expression of the disease in the OA case scenario and the lack of clear indication for injection. In addition, it is unclear why we failed to find improvements in recommendations for analgesics, recommended as the first-line treatment for mild to moderate OA in the workshops.
As reported in other studies4,5,6,12,35,36,37, perceptions of barriers to rheumatology and rehabilitation specialists were common. Improvements seen in this study may be related to providers having the opportunity to network with local specialists and to specifically discuss appropriate communication and referrals during the workshop. However, other issues may remain to be addressed, such as the overall shortage of rheumatologists and other healthcare professionals38. These are system-level barriers that no amount of education will change.
Interpretation of the results of this study must be done cautiously. There was no control group, therefore changes over time may have occurred because of changes in the Canadian healthcare environment or other unknown causes. As well, self-reported recommendations of best practices may not reflect what is done in actual practice and may be an underestimate or overestimate of performance. Jones, et al39 identified 11 articles where written case scenarios were assessed for criterion validity; they concluded that it was unclear whether written case scenarios could be used as proxies for actual performance. However, in the pilot study, case scenario responses were validated by assessing a subset of patients of providers who participated in the Grip program12. These patients reported receiving more information about arthritis, and more referrals were made to rehabilitation services in the community compared to a control group.
We were unable to determine what components of this multifaceted intervention influenced outcome. In a review of guideline dissemination and implementation studies, Grimshaw, et al reported no relationship between the number of components and the effects of multifaceted interventions17. We are now collecting specific information about which component of the intervention is perceived to be most influential in changing practice. However, the Grip program is resource-intensive and this method of guideline dissemination is only one way of influencing behavior change. There may be other more cost-effective methods of obtaining similar results.
Other limitations include the number of providers lost to followup at 6 months. It may be that this program is effective only for motivated providers from supportive organizations who participate fully in the program. The participation rate of providers was high in Ontario. This could have been because the Ontario Family Health Network was a partner in the program and directly recruited their member organizations for the study. It has also been suggested that good communications, low burden placed on providers to collect data, and financial incentives for completion of the data collection process might improve provider retention in studies40. Future studies need to explore these issues and test these strategies to successfully recruit and retain providers.
The program continues to be offered with slight modifications. The survey has been shortened and response options are provided to reduce the burden on the providers. Guidelines for referral to orthopedics have been added to the communications module and efforts are being made to attract more nurse practitioners and rehabilitation therapists to future workshops.
Results suggest that inter-professional learning may be an effective method for dissemination of guidelines and has potential to improve the delivery of arthritis care in a variety of primary care settings, particularly when nurse practitioners and rehabilitation therapists are involved in the care of patients. Future research is needed to determine which components of the intervention are most important in influencing outcomes, to establish the validity of the survey in predicting actual use of best practices, and to assess the influence of the program on patient outcomes.
Acknowledgment
The research team thank the staff of the participating primary healthcare organizations across Canada and the health professionals and patients that participated in workshop delivery. We also acknowledge the significant contributions of Jennifer Boyle, Annette Wilkins, and Paula Veinot and all the staff and students at ACREU and The Arthritis Society who participated in the implementation and evaluation of the project.
Appendix
Sample case scenario: Early RA5
A 45-year-old woman, a beauty counselor separated from her husband and responsible for the care of 3 school-age children, presents in your office with a 6 week history of pain, stiffness, and swelling of her hands and wrists. She also has some discomfort in her feet. She finds that she is worse in the morning with increased stiffness lasting about 3 hours. She has additional symptoms of fatigue and a 5 lb weight loss. She has been unable to work for the past week.
On examination, there is symmetrical swelling and tenderness of the small joints of the hands and wrists and tenderness of the metatarso-phalangeal joints. The remainder of the physical examination is normal.
There is no history of trauma. This patient has been previously well with no history of peptic ulcer disease or any other serious illness. A previous physician prescribed a 3-week course of a NSAID, without relief.
You are seeing this patient for the first time. Please list the investigations/assessments, interventions/treatments and referrals (practitioners, organizations, or resources) that you would conduct during this visit as it applies to your scope of practice.
Footnotes
-
Supported by the Primary Health Care Transition Fund, Health Canada.
- Accepted for publication December 1, 2010.








{kind=link}