

Abstract
Objective. To report the prevalence of work disability (WD) in a cross-sectional study of a large population of patients with ankylosing spondylitis (AS) and the associated demographic and clinical characteristics, including extraspinal features, that contribute to WD.
Methods. Patients with AS registered in a hospital database were invited to participate. A total of 360 patients took part. The survey period was 1998 to 2002. During an extended outpatient visit, data were collected according to a predefined data form. Demographic data were collected and a physical examination performed.
Results. After 22.6 years of disease duration, the cumulative prevalence of WD reached 43.6%, and an additional 8.9% of patients were nonparticipants in the labor force. Significant odds ratios indicating an independent association with WD were found for history of polyarthritis (9.6), coronary heart disease (CHD; 7.8), female sex (3.4), having children with spondyloarthritis (2.9), changing profession (2.8), lower level of education (1.4), mean score of the Bath AS Functional Index (1.2), increasing age (1.05), and increasing finger-to-floor distance (1.02).
Conclusion. The longterm prevalence of WD among Norwegian patients with AS is considerably higher than in reports from other countries. Earlier polyarthritis and CHD were the strongest independent risk factors for WD.
Ankylosing spondylitis (AS) is characterized by chronic inflammation of the sacroiliac (SI) and spinal joints, and may lead to a gradual loss of spinal function as the disease progresses1. In addition, extraspinal features may further increase the burden of disease. AS primarily arises in young adults who are in the midst of establishing careers and families, and may thus severely reduce a patient’s ability to participate in the labor force and social networks over time.
Boonen, et al reported the cost of AS in 3 European countries2 and showed an increased direct financial burden for patients that varied with disease duration, severity, and education levels. Ward, et al3 demonstrated an effect on social life in AS, because patients were more likely to be unmarried, divorced, and work-disabled compared to the general population. An earlier study from Norway reported work disability (WD) in almost 50% of patients after mean disease duration of 10 years4. These data indicate that the financial and social burden of disease in AS is substantial. The introduction of an effective but costly treatment for AS with anti-tumor necrosis factor-α (TNF) therapy has underlined the necessity of identifying risk factors that will predict a more severe outcome in this group of patients. To investigate which factors predict early retirement from the labor force in a population of patients with AS, we analyzed the prevalence of early withdrawal from the labor force, and its association with demographic data, spinal function test, level of function, and the presence of comorbidities in a large regional AS population5,6.
MATERIALS AND METHODS
The University Hospital of Northern Norway is located in Tromsø, the largest city in the northern part of Norway. The Department of Rheumatology is the second-line referral unit for the 3 northernmost counties, with a total population of about 500,000, and the first-line referral unit for the 2 northernmost counties (population 240,000), and the majority of patients with AS from those 2 counties are referred to this department for an evaluation. All available patients registered in the hospital database after the foundation of the rheumatology department in 1978 were invited to participate in our study if they had a diagnosis of AS (ICD codes 720 and M45) and fulfilled the modified New York criteria for AS after evaluation of SI joint radiographs7. This included patients with AS who had been admitted to other departments in the hospital, so identifying patients was not dependent on referrals alone. The survey was carried out for the period 1998–2002. This allowed us to verify that the level of function was indeed permanently reduced, and also allowed an evaluation of disability prior to any anti-TNF therapy. During an extended outpatient visit, data were collected according to a predefined data form. Demographic data were registered, along with family history of spondyloarthropathies (SpA) and social, professional, and educational status. Patients completed questionnaires evaluating function [Bath Ankylosing Spondylitis Functional Index (BASFI)]8. A complete physical examination was performed that included modified Schober’s test (cm), occiput-wall distance (cm), finger-to-floor distance (cm), chest expansion (cm), and spinal flexion/spondylometry (degrees). Spondylometry was performed using the Dunham spondylometer, which has been shown to discriminate between patients with AS and healthy controls9. All examinations were performed by an experienced clinician.
Disease onset was defined as the time of onset of back symptoms, and time of diagnosis was set as the time of radiographic confirmation of sacroiliitis according to the modified New York criteria7. Direct complications of AS were registered only when there was objective evidence documented in the patient’s medical records for acute anterior uveitis (AAU), inflammatory bowel disease (IBD), psoriasis, atrioventricular (AV) conduction disorder, aortic valve regurgitation, lung involvement (fibrosis), or amyloidosis. Information about additional comorbidities, obtained through questioning the patient and examining the patient’s medical records, was registered separately, i.e., gastrointestinal (GI) diseases other than IBD, heart conditions other than AV conduction disorder or valve disease, dermatologic conditions other than psoriasis, as well as any neurologic disease or cancer. This indicates that only patients with a previously recognized myocardial infarction or patients who were being treated for angina pectoris were registered as having a coronary heart disease (CHD).
The primary outcome in our study was WD at the time of investigation. In Norway, WD is granted as a benefit from the public social security network system for persons with at least a 50% reduction in earning capacity due to chronic disease. An individual with a longterm (> 3 years) ability to work only half-time or less because of disease could be granted at least a 50% WD benefit. WD is thus a general definition that does not specify the cause of the disability. Secondary outcome was nonparticipation in the labor force for other reasons, such as unemployment, longterm sick leave, or homemaking. Patients who reached the age limit for retirement without WD were censored from that point onward. At the time of the survey, the level of WD in the general adult population of Norway was 9.8% (Oslo: Statistics Norway). The regional ethics committee approved the study protocol and patients gave informed consent.
Statistical methods
Data were stored electronically (Epi Info version 6; Centers for Disease Control and Prevention, Atlanta, GA, USA) and later transferred to SPSS version 16.0 (SPSS Corp., Chicago, IL, USA) for completion and statistical analyses. Survival analyses were performed by the Kaplan-Meier method. Comparative analyses between groups were performed using chi-squared analysis for categorical data and the Mann-Whitney U test for continuous data. Clinical and demographic features associated with WD with p values < 0.2 were subsequently incorporated in a multivariate logistic regression model to determine their independence. The selection of variables to be rejected from the model was done after an evaluation of both p values and clinical relevance, such as IBD, psoriasis, and AAU10. Resulting 2-sided p values < 0.05 were considered significant. In the logistic regression analysis, a total of 104 cases had missing data in 1 or 2 variables, mostly missing values for single features in composite functional scores or years of education. Because excluding these patients would significantly affect the logistic regression model, missing values were replaced with mean or median values as recommended, depending on the degree that the data are skewed10,11.
RESULTS
Demography
Of 687 total patients registered, 53 had died and 49 no longer resided in the catchment area at the time of the research visit. Of the remaining 585 patients, 360 (62%) accepted an invitation to a study visit at our outpatient clinic. The invitation was reiterated to patients who failed to respond to the first invitation. There was no difference between the responders and nonresponders regarding sex or age distribution. Demographic data on the 360 patients with AS are presented in Table 1, together with the frequency in patients with or without WD. Almost half of all patients reported SpA in first-degree relatives (48%), but this information was not independently confirmed. There were no significant sex differences in the demographic data (data not shown).
Demographic characteristics in work-disabled (WD+) and non-work-disabled (WD–) patients with ankylosing spondylitis (AS). Data are mean values unless otherwise indicated.
Functional limitations
Median BASFI (0–10) score was 3.5. Also, 78% of patients had an abnormal modified Schober’s test (< 5.0 cm), 31% had increased occiput-wall distance, and 56% had a reduced chest expansion (< 5.0 cm; Table 2). Men scored significantly lower on spinal mobility tests, but BASFI scores did not differ between men and women (data not shown). Patients with WD scored significantly higher on all items in BASFI and had worse spinal mobility measurements (modified Schober’s, spondylometry, chest expansion, and occiput-wall distance).
Functional score (BASFI) and spinal mobility in work-disabled (WD+) and non-work-disabled (WD–) patients with ankylosing spondylitis (mean values).
Extraspinal complications and comorbidities
A total of 55.8% of patients had experienced 1 or more extraspinal complications to AS. At least 1 episode of AAU was reported by 41.9% of the cohort, while the prevalence of peripheral arthritis, psoriasis, and IBD was 16.9%, 11.1%, and 8.1%, respectively. Cardiac involvement (AV conduction disorder or aortic insufficiency) was frequent and was identified in 6.7%, while lung involvement and amyloidosis were rare, each occurring in 0.6% of cases.
Work disability
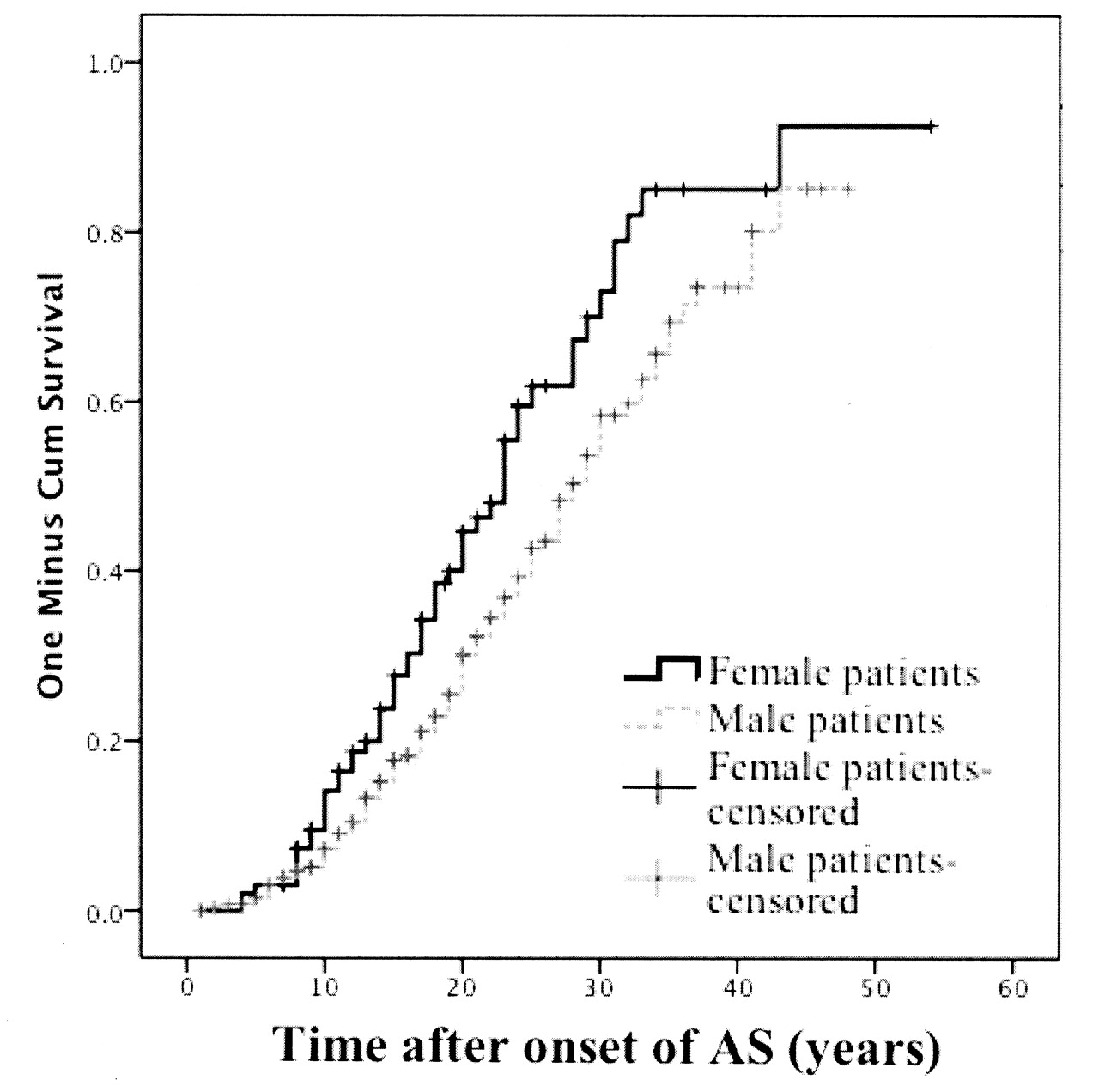
The cumulative frequency of WD was 43.6%, as 157 of the 360 patients had withdrawn from the labor force. An additional 32 patients (8.9%) were classified as nonparticipating, mostly (5.6%) because of unemployment. Twenty patients were older than the official retirement age (67 years) at the time of the followup visit, but of these, 15 had retired because of WD. The average time from onset of disease to WD was 18.7 years (SD 9.5). A Kaplan-Meier plot showed that the risk of WD increased linearly after 10 years of disease duration (Figure 1) without reaching a plateau phase.
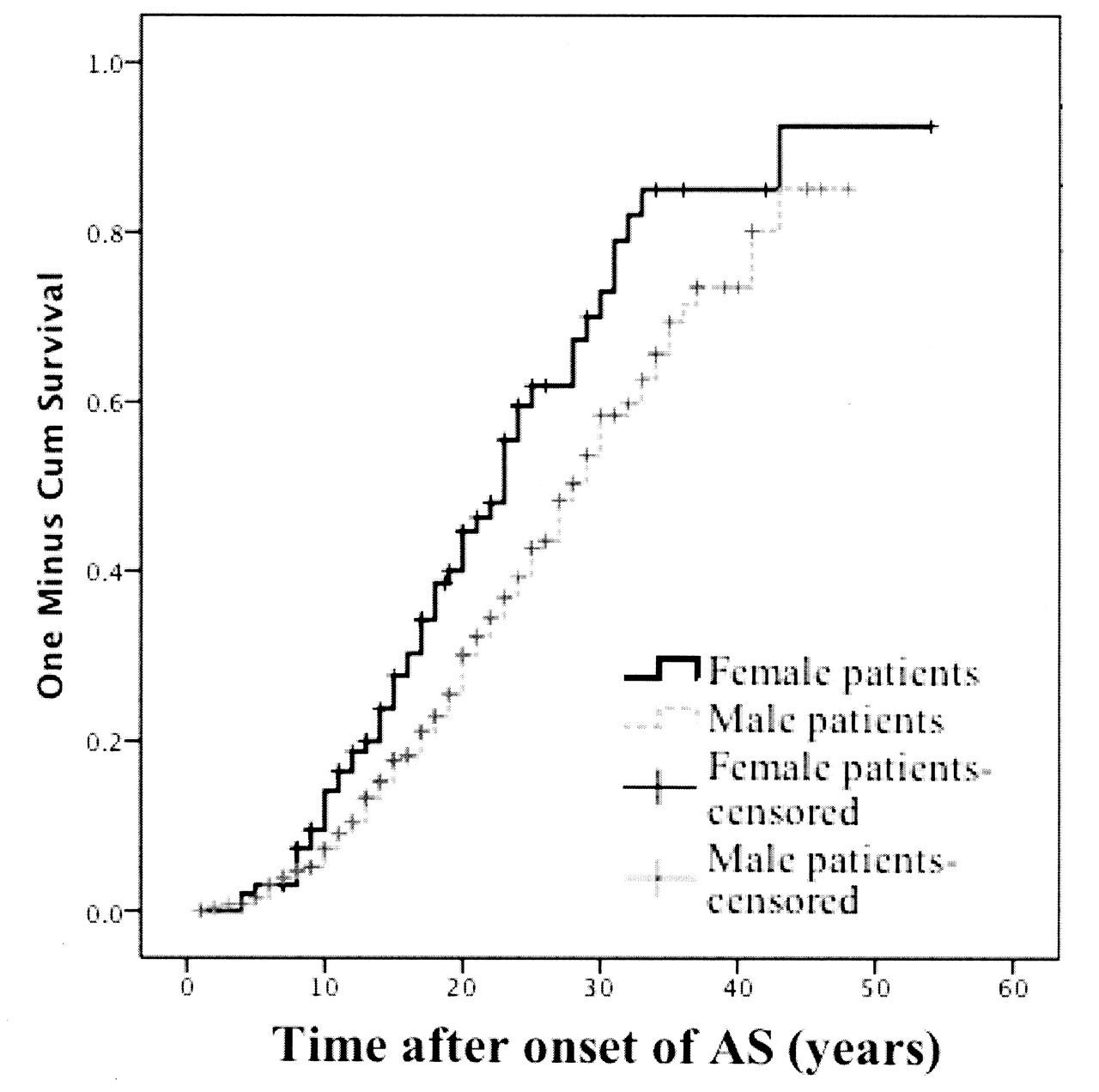
The risk of work disability increased with years of ankylosing spondylitis (AS) duration.
Variables associated with WD
By univariate analysis, the risk of WD was significantly increased for women patients (OR 1.90), while higher education (defined as college/university) reduced the risk of WD (OR 0.22; Table 3). In addition, disease duration > 25 years (OR 3.62) was significantly associated with WD. Patients who experienced WD had a significantly longer diagnostic delay (Table 1); however, the delay did not contribute to the development of WD. Other factors associated with WD were the presence of CHD (OR 10.62), aortic valve insufficiency (OR 5.52), and GI disease other than IBD (OR 3.63). Previous or present polyarthritis (OR 2.3) occurred considerably more frequently among patients with WD, while oligoarthritis or monoarthritis did not. An increased risk of WD existed for patients reporting that they had a child with SpA features (OR 5.52), but the effect did not apply to any other first-degree relative with AS/SpA. Marital status had no effect on WD, but patients with WD were more likely to have made career changes (OR 1.64) than patients who did not have WD. More frequent career changes were also a significant variable in the logistic regression model. The final multivariate model retained these as independent predictors for WD: female sex, age at followup, a lower level of education, having a child with SpA, the presence of CHD, previous or present polyarthritis, higher BASFI score, and increased finger-to-floor distance (Table 3).
OR for work disability for various disease characteristics in patients with ankylosing spondylitis by univariate and subsequent multivariate analysis.
DISCUSSION
In our single-center cohort study, 44% of patients with AS became work-disabled and an additional 8.9% were not participating in the labor force after a mean disease duration of 22.6 years. The average time from onset of AS to WD was 18.7 years, but the risk for WD increased linearly over time. Interestingly, 15 of the 20 patients who had reached the age limit for retirement were also work-disabled; considering the linear increase of WD over time, the lifetime risk of WD is actually substantially higher than 44%.
While the frequency of WD among patients with AS has been reported in several other studies, there is substantial variation between different countries. A study by Ariza-Ariza, et al reported that 25% of Spanish patients with AS were permanently work-disabled, including partially disabled individuals12. In Argentina, 9.4% of patients with AS were found to be disabled, but at the same time patients with AS were 5 times more likely to be unemployed compared to healthy controls13. This is quite similar to the findings of Ward, et al3, who reported the effect of AS on work participation in the United States. They found that patients with AS were more likely to be either disabled (13.3%) or not participating in the labor force (25.1%) when compared to controls. They also found that the increased risk of WD was associated with age, female sex, and not having a college education, while male patients were less likely to participate in the work force. In a Czech study of 1008 patients with AS, Forejtová, et al14 found that 30% of the patients were or had been receiving fulltime disability pensions. The disease duration in both these studies was similar to the disease duration in our population. It should also be noted that our patient population included both mild and severe cases because our department represents the only rheumatology service in the catchment area, in contrast to Ward, et al3, who recruited patients from rheumatology clinics, and Forejtová, et al14, who based their patient selection upon membership in the national organization of patients with AS. Thus, the possibility of a selection bias exists, but because we have no other indications that there are major clinical differences among patients with AS in these countries, these differences likely reflect variations in the health benefit systems. Hence, when a patient with AS in our country is considered to have a permanently reduced earning capacity because of WD, this person is likely to be granted a WD pension rather than having to enter unemployment.
Women were more likely than men to experience WD due to AS, a finding consistent with the results of Ward, et al3 and Boonen, et al15. On the other hand, this finding contradicts the results of the Czech14 and Spanish studies12, which showed significantly increased WD among men compared to women. This occurred even though functional measurements such as modified Schober’s test, forward spinal flexion, and occiput-wall distance were better preserved in women patients, while there were no significant differences in composite functional scores. This might be influenced by a sex-specific difference in risk of WD, as an increased risk of WD among women compared to men has been reported (OR 1.88; Statistics Norway 2003). Hence, the observed difference in our cohort regarding sex and risk of WD might reflect a general trend in the Norwegian population.
BASFI score was also significantly associated to WD in our study, and an association between a patient’s subjective evaluation of the level of function and WD seems plausible. However, of the objective measurements of spinal mobility, only finger-to-floor distance was retained in the multivariate model. This apparently paradoxical observation would suggest that composite functional scores are reflecting other factors than mere physical limitations.
Marital status did not predict WD, a finding consistent with previous reports16. Quite a large proportion (48%) of the patients, however, reported 1 or more first-degree relatives with an SpA feature, but only patients reporting having children with SpA (10.3%) were more likely to enter WD. This suggests that in some patients a genetic predisposition increases the risk of a more severe disease course as well as the risk of AS developing in their children. However, as this questionnaire-based information was not confirmed independently, the association should be interpreted cautiously but could merit extended family studies.
The occurrence of aortic regurgitation (4.2%) and CHD (4.7%) were the only extraspinal SpA features, in addition to polyarthritis, associated with WD, while AV conduction disorders (2.5%) were not associated with WD. Moyssakis, et al17 recently published a study indicating an increased aortic stiffness and reduced myocardial performance in patients with AS, and these changes correlated to disease activity as measured by the Bath Ankylosing Spondylitis Disease Activity Index. According to Roldan, et al18, aortic root thickening occurred in 82% of patients with AS (n = 44) evaluated with transesophageal echocardiography. Valvular regurgitation was demonstrated in 45% of patients, either mitral or aortic valve prolapse in 16%, and AV conduction disorder in 4.5%. There was a correlation between valvular disease and aortic wall thickening and both were correlated to disease duration, but not disease activity. In comparison, our finding of aortic regurgitation in 4.2% is low, but we did not perform screening echocardiography and recorded only clinically established disease. Because of the lack of a control group, we were unable to calculate risk ratios for CHD, but the high CHD frequency supports evidence of an increased prevalence of CHD in patients with AS19, in agreement with findings in systemic lupus erythematosus and rheumatoid arthritis. The fact that patients with AS undergo coronary bypass grafting at an earlier age further supports this20,21,22,23. Thus, considering the significant correlation between cardiovascular disease (CVD) and WD, the increased frequency of CVD in AS merits close medical attention.
AAU has been reported to affect around 16%–36% of patients with AS4,24. In contrast, we found that 41.9% of the patients had ever been diagnosed with AAU and 28.8% had recurrent AAU. These are among the highest rates reported and one may wonder if this is related to a high frequency of HLA-B27 in this region25,26. While previous studies concluded that the occurrence of AAU implies a more severe disease24, we found no increased risk of WD due to AAU or other noncardiac comorbidities. We did observe a trend toward increased risk for WD in patients with > 1 episode of AAU (p = 0.063) or with > 1 comorbidity (p = 0.082; data not shown). While patients with IBD were not at increased risk for WD, disabled patients were more likely to have other GI disorders, mainly ventricular or duodenal ulcers, by univariate analyses. However, this was not retained in the multivariate model, but this could indicate an increased use of nonsteroidal antiinflammatory drugs in patients with more severe disease. Other comorbidities, such as previous cancer, pulmonary disease, dermatologic disease other than psoriasis, or neurological disease, did not occur more often in patients with WD. Only 2 patients (0.6%) had developed amyloidosis and both subsequently underwent renal transplantation. As most of these observations were done in the pre-TNF-inhibitor era, one would perhaps expect a larger proportion of the patients to be affected by amyloidosis, because previous systematic surveys of patients with AS regarding amyloidosis have shown a prevalence of 5%–6%. However, these studies have based the diagnosis of amyloidosis on subclinical fat tissue amyloid deposits, while we registered only clinically overt disease27,28. Lung involvement has been considered very rare in AS, but it has been shown that radiographically detectable disease is more common than previously recognized29. Our finding of 0.6% with pulmonary involvement must therefore be considered a conservative estimate. Thus, while extraspinal features in AS are frequent, our data indicate that only cardiac and peripheral joint involvement increase the risk of WD significantly.
Lower levels of education have been shown to be an important risk factor for WD in AS4. Our study supports those findings, because education below college levels was an independent WD predictor, and patients with WD were more likely to have made career changes over time. These findings might be related to a lower flexibility and ability to compete in the job market as a consequence of lower education combined with physical impairment, which in the end increases the risk of withdrawal from the labor force. The finding in the univariate analyses that patients with late-onset disease had a worse outcome is consistent with this, because those patients may not have had the same incentives to pursue higher education as patients with earlier disease onset.
Diagnostic delay was also evaluated as a possible factor associated with WD, but although disabled patients certainly had an increased delay compared to the nondisabled, there was not a significant contribution to the model from this variable. There did, however, seem to be an association if the delay was longer than 12 years (data not shown).
There are several limitations to our study. We were not able to reexamine every patient registered in our cohort, with a response rate of 62%. This may have biased our data, because we cannot disregard the possibility of differences in the levels of individual variables between respondents and nonrespondents. However, the lack of differences in terms of sex or age among study participants and patients not included may to some extent indicate that the participants were representative of the total AS population. The conclusions in this study would, however, have been more compelling if a healthy control group had been included for comparison of WD prevalence as opposed to the general population. Because of the retrospective design of the study, we have identified factors associated to WD rather than predictors of WD. We considered only whether the individual patient was disabled according to the definition used by the public social security network system, and did not evaluate AS as the specific cause of WD. However, this allowed us to consider WD caused by both AS and any possible complications to AS, such as IBD and CHD. Further, we did not include characteristics of profession and psychological factors such as differences in coping strategies in our analyses. It is also important to point out that these data are relevant for the Norwegian population and cannot be directly applied to regions with different social security structures. Finally, while data in our study were collected by 4 different physicians, all were experienced in AS management and used predefined collection forms, which reduces the potential for biased evaluation of the patients.
Considerable WD occurs among Norwegian patients with AS. Carried out in a pre-TNF-inhibitor cohort, this study indicates that conservative measures such as patient counseling and education in order to maintain or improve function through exercises and lifestyle are often inadequate in the prevention of WD in AS. As a disease that primarily affects people from a young age, this loss of earning capacity has substantial implications for individual patients and society. Female sex, older age, low levels of education, having a child with SpA, reduced level of function, polyarthritis, and CHD independently identify patients at increased risk for WD.
- Accepted for publication November 23, 2010.








{kind=link}