

Abstract
Objective. Reports have suggested that bone mineral density (BMD) is higher in patients with osteoarthritis (OA) of the hip than in healthy controls. Various types of OA of the hip caused by osteophyte formation were observed on radiographs during progression to the advanced degenerative stage, and the preoperative type of OA was reported to influence the results of surgical treatment. However, the mechanism underlying the development of different types of OA is still unknown. We measured BMD of patients with hip OA and determined whether higher BMD was observed in patients with osteophyte formation than in those without osteophytes.
Methods. We measured BMD of the lumbar spine, radius, and calcaneus using dual-energy x-ray absorptiometry in 88 women who were scheduled to undergo total hip arthroplasty for endstage OA. Hips were evaluated for osteophyte formation using Bombelli’s classification; 31 were graded as atrophic type, 30 as normotrophic, and 27 as hypertrophic. BMD at different skeletal sites were compared among the 3 types of OA.
Results. No significant difference in BMD of the lumbar spine, ultradistal radius, mid-radius, or calcaneus was observed among the atrophic, normotrophic, and hypertrophic types of OA.
Conclusion. Our data suggest that osteophyte formation is not related to general BMD. Factors other than general bone status, for example the morphology of the hip joint, need to be analyzed to determine the pathomechanism of osteophyte formation in the osteoarthritic hip.
Osteoarthritis (OA) and osteoporosis are age-related degenerative diseases that are common in both middle-aged and older women1,2. It is generally agreed that the incidence of osteoporosis is inversely related to that of OA3.
Various types of OA of the hip caused by osteophyte formation can be observed on radiographs during progression to the advanced degenerative stage4, and the preoperative type of OA was reported to influence the results of surgical treatment5,6. However, the mechanism underlying the development of different types of OA is still unknown.
Many reports have suggested that bone mineral density (BMD) was higher in patients with OA of the hip than in healthy controls7,8,9,10,11,12,13. However, to our knowledge, there are no reports that compare BMD among patients with different types of OA. Therefore, we measured BMD in patients with hip OA and determined whether higher BMD was observed in patients with osteophyte formation than in those without osteophytes.
MATERIALS AND METHODS
We measured BMD in patients with different types of OA of the hip. The protocol of this study was approved by the institutional review board of our university.
All male patients and women less than 45 or more than 70 years of age were excluded from matching for sex and age among patients with OA. Patients taking any medication that could affect bone metabolism, such as steroids and bisphosphonates, were also excluded.
Between 1997 and 2005, we measured BMD of patients who were scheduled to undergo total hip arthroplasty for endstage OA. We excluded patients with a history of hip osteotomy and patients with secondary hip OA because of hip fracture, inflammatory rheumatic disease, osteonecrosis, or infectious disease. We also excluded patients with severe subluxation, defined as Crowe type II–IV (more than 50% subluxation)14, because discrepancy in leg length sometimes causes scoliosis of the lumbar spine, and a different femoral head position may influence osteophyte formation. We studied 88 women with endstage OA who were scheduled for total hip arthroplasty.
All radiographs were performed with the patient in the supine position. Anteroposterior radiographs were taken with a source-to-film distance of 110 cm. The patient’s feet were internally rotated with the toes at 15° ± 5° to ensure that the radiograph beam was centered on the superior aspect of the pubic symphysis.
Clinical symptoms were evaluated using Merle d’Aubigné and Postel’s hip joint scoring system15, in which a maximum of 6 points each is assigned for these criteria: pain, mobility, and walking ability.
The severity of OA was radiologically staged from 1 to 4, as defined by the Japanese Orthopaedic Association16. In this system, patients with Stage 4 (endstage) OA show almost total disappearance of the joint space on the anteroposterior radiographs. The inclusion criterion for this study was Stage 4 (endstage) OA.
The osteoarthritic hips were classified radiographically into 3 types, basically those proposed by Bombelli4 and defined more precisely by Saito, et al5, according to the appearance of the femoral head. These types were atrophic, normotrophic, and hypertrophic. Atrophic hips showed no osteophyte formation, and in a few cases the femoral head was reduced in size (Figure 1A). The normotrophic type had an intermediate degree of osteophyte formation with an immature, beak-like capital drop (Figure 1B). The hypertrophic type showed well developed osteophytes around the femoral head with a large capital drop (Figure 1C). Two authors examined the inter-observer reproducibility of OA type using 20 randomly selected hips. The interobserver variability (κ statistic) was 0.91.
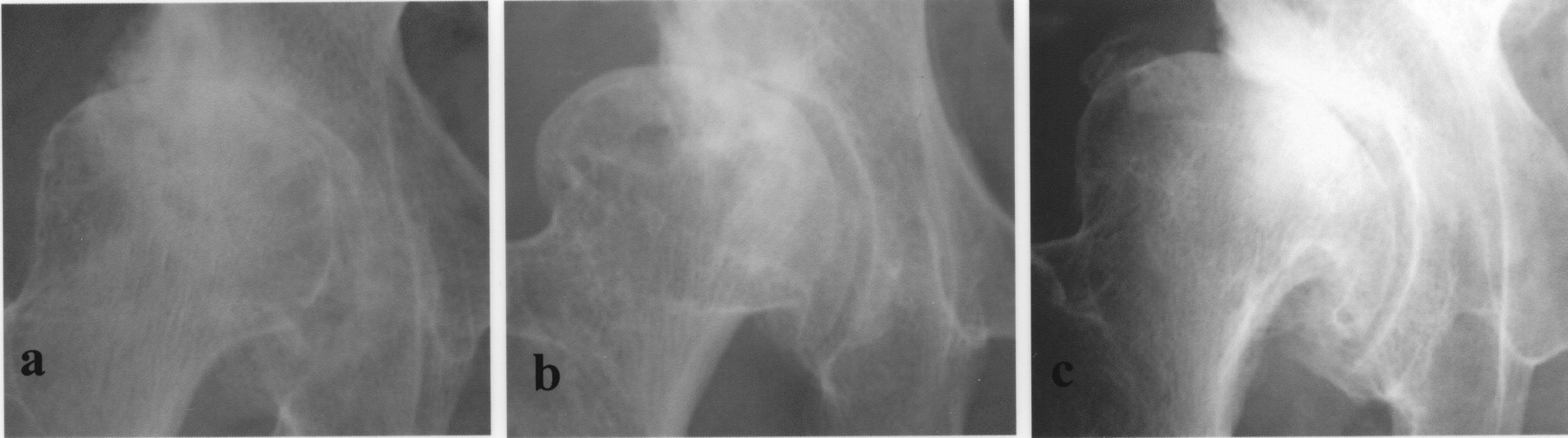
Representative radiographs of patients with different types of osteoarthritis. Hips with the atrophic type (a) showed no osteophyte formation. The normotrophic type (b) had an intermediate degree of osteophyte formation. The hypertrophic type (c) showed well developed osteophytes around the femoral head with a large capital drop.
BMD of the lumbar spine (L2–L4) in the anteroposterior projection was determined using dual-energy x-ray absorptiometry (DEXA). Fractured vertebrae were eliminated from analysis. Radial BMD was measured in a nondominant site at the ultradistal and midshaft at a point one-third of the distance from the ulnar styloid process to the olecranon process (mid-radius) using DEXA. Calcaneal lateral integral BMD on both sides was measured by DEXA. The values obtained were expressed as g/cm2 for the projected area. An EXP5000 instrument (Lunar, Madison, WI, USA) was used to measure BMD of the lumbar spine and radius, and a HeelScan DX-2000 machine (KDK, Kyoto, Japan) was used for the calcaneus. The coefficients of variation for the L2–L4, radius, and calcaneus were 1.1%, 1.8%, and 0.8%, respectively.
We assessed differences among the 3 groups (atrophic, normotrophic, and hypertrophic types of OA) using the Kruskal-Wallis test. Differences with a p < 0.05 were considered significant.
RESULTS
The 88 patients were classified into 31 with the atrophic type of OA, 30 with the normotrophic type, and 27 with the hypertrophic type. There were no significant differences in age, height, weight, body mass index, or total hip score among the 3 groups (Table 1). No significant difference in BMD of the lumbar spine, ultradistal radius, mid-radius, or calcaneus was observed among the atrophic, normotrophic, and hypertrophic groups (Table 2).
Background characteristics of age, height, weight, body mass index (BMI), and total hip score in patients with atrophic, normotrophic, and hypertrophic osteoarthritis. Values are mean ± SD (range).
Comparison of bone mineral density (BMD; g/cm2) obtained by dual-energy x-ray absorptiometry in patients with atrophic, normotrophic, and hypertrophic osteoarthritis. Values are mean ± SD (range).
DISCUSSION
Higher BMD has been reported in patients with OA of the hip compared with healthy controls7,8,9,10,11,12,13. However, there are no previous reports comparing BMD among patients with hip OA, even though radiographs reveal various types of OA of the hip related to osteophyte formation4. Therefore, we determined whether higher BMD was observed in patients with osteophyte formation than in those without osteophytes.
Our study has limitations. We did not measure the BMD around the hip joint. Degenerative changes in the articular cartilage of the hip joint are accompanied or preceded by increased subchondral bone density, leading to radiographically observable sclerosis17. These findings suggest that increased BMD around the osteoarthritic hip joint may be a component of the disease process in hip OA. Therefore, to estimate the relationship between osteoporosis and various types of OA of the hip, BMD at sites other than the proximal femur in patients with hip OA needs to be measured. We measured BMD at the lumbar spine, radius, and calcaneus. We considered that these sites are suitable to evaluate the general bone status of patients with OA.
Several studies have reported that BMD at the femoral neck in patients with OA of the hip was higher than that in healthy controls7,8,9,10,11,12,13. However, BMD at skeletal sites other than the femoral neck was reported to be higher than7,8 or not different from11,18,19 that in controls. Differences in radiographic stages of OA and different physical activities of patients among individual studies may influence BMD measurements at different skeletal sites in patients with OA. In our study, all patients had Stage 4 (end-stage) OA, in which there was almost total disappearance of the joint space on anteroposterior radiographs (Figure 1), and there were no differences among the groups in total hip score based on the 3 criteria of pain, mobility, and walking ability (Table 1). Therefore, any secondary effect on BMD at different skeletal sites caused by reduced physical activity as a result of hip pain must have been small in the study groups.
Bombelli classified the osteoblastic response in hip OA into 3 categories according to osteophyte formation on radiographs: hypertrophic, normotrophic, and atrophic4. Previous studies reported that patients with preoperative osteophyte formation in the hip have a low rate of loosening of total hip arthroplasty5 and good results of joint-preserving operations6, and suggested that the osteoblastic response in OA might influence the results of surgical treatment. Recently, bisphosphonates were reported to have a significant effect in preserving acetabular and femoral bone mass after total hip arthroplasty20. Estrogen also appears to be protective against OA; in 1 report, women who were currently using oral estrogen had a significantly reduced risk of OA in the hip21. These reports suggest that a drug for osteoporosis should have the ability to reduce the progression of OA or to improve the results of surgical treatment for patients with OA of the hip. These clinical reports encouraged us to examine the relationship between osteophyte formation and general BMD in patients with hip OA. However, we observed no differences.
There is some evidence for an inverse relation between osteophyte formation in OA and osteoporosis. In a study of patients with OA of the knee, BMD in the proximal femur in women with osteophytosis of the knee was higher than in women with no osteophytes22. The authors concluded that subjects with higher BMD were “bone formers” and thus had an increased tendency toward osteophytosis compared with subjects with lower BMD. In a study of patients with OA of the hand, there were increased levels of insulin-like growth factor-1 (IGF-1) and IGF-2 and transforming growth factor-ß, and it was suggested that these may reflect increased activity of osteoblasts23. Further support for this is the observation that decreased levels of IGF-1 were reported in women with osteoporosis24. A study of hip OA from South Africa examined the bone histomorphometry of the iliac crest and the prevalence of spinal fracture in primary OA of the hip, and suggested that the prevalence of generalized osteoporosis is higher in patients with the atrophic type of OA than in those with hypertrophic OA25. In a Japanese population, primary OA accounted for only 0.65% of 2000 consecutive cases, and most patients had OA secondary to developmental dysplasia of the hip (DDH)26. Analyses of the morphology of OA secondary to DDH using plain radiographs and computed tomography showed a wide range in the values of anatomic measurements of the acetabulum and proximal femur compared with healthy controls27,28. In OA secondary to DDH, factors other than generalized bone status, such as the morphology of the hip joint, might influence osteophyte formation.
We found no significant difference in the BMD of the lumbar spine, radius, or calcaneus among patients with the atrophic, normotrophic, and hypertrophic types of hip OA. Our data suggest that osteophyte formation is not related to BMD at sites other than the hip. Factors other than general bone status, such as the morphology of the hip joint, should be analyzed to determine the pathomechanism of osteophyte formation.
- Accepted for publication September 21, 2010.








{kind=link}