

Abstract
Objective. We studied whether sonographic needle guidance affected the outcomes of intraarticular (IA) injection for inflammatory arthritis.
Methods. Joints with inflammatory arthritis (n = 244; 76% rheumatoid arthritis, 3% small joints, 51% intermediate, and 46% large) were randomized to injection by conventional palpation-guided anatomic injection (120 joints) or sonographic image-guided injection enhanced with a 1-handed reciprocating procedure device mechanical syringe (124 joints). A 1-needle, 2-syringe technique was used. After IA placement and synovial space dilation were confirmed by sonography, a syringe exchange was performed, and triamcinolone acetonide was injected with the second syringe through the indwelling IA needle. Baseline pain, procedural pain, pain at outcome (2 weeks and 6 months), responders, therapeutic duration, reinjection rates, total cost, and cost per responder were determined.
Results. Relative to conventional palpation-guided methods, sonographic guidance for injection of inflammatory arthritis resulted in an 81% reduction in injection pain (p < 0.001), 35% reduction in pain scores at outcome (p < 0.02), 38% increase in the responder rate (p < 0.003), 34% reduction in the non-responder rate (p < 0.003), 32% increase in therapeutic duration (p = 0.01), 8% reduction ($7) in cost/patient/year, and a 33% ($64) reduction in cost/responder/year for a hospital outpatient (p < 0.001).
Conclusion. Sonographic needle guidance improves the performance, clinical outcomes, and cost-effectiveness of IA injections for inflammatory arthritis. (Clinical Trial Identifier NCT00651625)
In the management of rheumatoid arthritis (RA) and other inflammatory joint diseases, intraarticular (IA) injection of corticosteroids is a useful adjunct to disease-modifying medications, biologic-response modifiers, joint protection, local measures, and the use of analgesics and antiinflammatory medications1. When performed by skilled proceduralists, the accuracy of IA placement of the needle by palpating surface anatomic landmarks ranges from 50% to 93%2,3,4,5,6,7,8. Sonographic needle guidance significantly improves IA accuracy relative to traditional palpation-guided methods; however, data regarding outcomes are limited, and cost-effectiveness analyses in particular are lacking5,9,10,11,12,13,14,15,16,17. This dearth of cost-effectiveness data has naturally provoked challenges to sonographic guidance, and has caused skepticism and resistance to integrating image-guided procedures into the musculoskeletal injection clinic18,19,20,21.
We hypothesized that sonographic guidance would improve the outcomes and cost-effectiveness of IA injection of inflammatory arthritis, including RA5,9,10,11,12,13,14,15,16,17. Our randomized controlled study addressed whether sonographic needle guidance with enhanced needle control affected the clinical outcomes and cost-effectiveness of IA injection of inflammatory arthritis.
MATERIALS AND METHODS
Subjects
This project was in compliance with the Helsinki Declaration, approved by the institutional review board, and registered at ClinicalTrials.gov (Clinical Trial Identifier NCT00651625). The Consolidated Standards of Reporting Trials study procedure is shown in Figure 1. Inclusion criteria included (1) the presence of immune-implicated inflammatory arthritis [systemic lupus erythematosus (SLE), reactive arthritis, psoriatic arthritis (PsA), or RA]21; (2) functional status I–III arthritis (individually graded as 1–3 for analysis)22; (3) persistent pain in the involved joint resulting in a referral to the injection clinic; (4) significant pain in the involved joint by 0–10 cm visual analog pain scale (VAS), where VAS score was ≥ 5 cm17,23; (5) stable doses of medications including methotrexate, oral corticosteroids, and biological-response modifiers; (6) the indications for injection, including failure of local measures, oral medications, rest, exercise, and analgesics1; and (7) the recommendation from the examining physician that the patient undergo an IA injection1,17,21,22,23,24,25. Exclusion criteria included (1) endstage joint damage (bone-on-bone)24; (2) hemorrhagic diathesis; (3) the use of warfarin or antiplatelet therapy; (4) the presence of infection; or (5) the presence of a confounding inflammatory arthritis due to gout, pseudogout, infection, or inflammatory osteoarthritis. Out of 256 consecutive subjects with an inflamed joint who were assessed for eligibility, 12 were excluded based on the above inclusion and exclusion criteria. A total of 244 joints with inflammatory arthritis were randomized between (1) palpation-guided injection (120 joints), and (2) sonographic guidance (124 joints; percentage difference +3%; 95% CI −3% to +3%, p = 0.50). Diseases among the subjects were RA (76%), with lesser proportions of SLE (9%), reactive arthritis (11%), or PsA (4%). The joints injected included 111 large joints (85 knees, 17 shoulders, 9 hips), 124 intermediate joints (76 wrists, 27 ankles, 21 elbows), and 9 small joints (4 proximal interphalangeal joints, and 5 metacarpophalangeal joints).

Formation of the study group.
Outcome measures
Patient pain was measured with the standardized and validated 10 cm VAS, where 0 cm = no pain and 10 cm = unbearable pain17,23. Significant pain was defined as a VAS score ≥ 5 cm17. Pain by VAS was determined (1) prior to the procedure (baseline pain); (2) during the insertion of the needle (procedural pain); (3) during injection of the treatment drug (injection pain); (4) 2 weeks postprocedure (pain at primary outcome); and (5) 6 months postprocedure (secondary outcome). At the time of the initial procedure, the patient was provided with a printed VAS scale to take home. The outcome inquiries at 2 weeks and 6 months were performed by telephone call — the patient looked at the printed VAS and rated pain accordingly. The inquirer was blinded to the ultrasound versus nonultrasound treatment groups. Two weeks has been demonstrated as the outcome measurement time most likely to detect maximum clinical effect of injected corticosteroid; thus, the 2-week observation was considered the primary outcome measure26,27,28,29. Responders were defined as an asymptomatic joint (VAS < 2 cm) at 2 weeks; nonresponders were defined as a symptomatic joint (VAS ≥ 2 cm) at 2 weeks16,23. Duration of therapeutic response was defined as the time interval in months when the joint became symptomatic (VAS ≥ 2 cm). If the joint remained asymptomatic at 6 months or longer, the duration was defined as 6 months. If the joint required reinjection before 6 months, the 6-month pain score was defined as the pre-injection pain score. Time to next injection or referral for surgery was determined by both chart review and patient interview at 12 months after the initial injection and expressed in months. If the next injection or referral to surgery occurred at a time greater than 12 months, the time to next injection was defined as 12 months.
Costs of the procedure in US dollars were defined as those costs reimbursed by 2010 Medicare (United States) national rates for large, intermediate, and small joint arthrocentesis, respectively, in a physician’s office ($73.01, $55.68, and $51.25 per procedure, respectively) and as a hospital outpatient ($48.67, $40.19, and $38.35 per procedure), plus 2 ml triamcinolone acetonide ($14.94/procedure) and sonographic needle guidance ($185.47/procedure) in a physician’s office, plus $2/procedure for each mechanical syringe or $0.30 for each conventional syringe30. As of 2010, Medicare provides no separate payment for sonographic needle guidance for a hospital outpatient. Yearly costs were calculated by multiplying the costs/procedure × 12 months divided by the months to reinjection or referral to surgery. Yearly cost per responder was calculated by dividing the yearly cost by the proportion of responders.
Sonographic needle guidance with enhanced needle control
The sonographic-guided injection procedure was also performed in a standardized manner using a 1-needle 2-syringe technique (Figures 2, 3, and 4)17. All sonographically guided procedures were performed by fellows-in-training directly supervised by experienced proceduralists. All conventional injections were performed by experienced proceduralists. Depending on joint size and presence of effusion, a 25 to 21-gauge, 1 to 2-inch needle (305783-BD Needle, Becton Dickinson, Franklin Lakes, NJ, USA) was mounted on a 3 ml to 25 ml reciprocating procedure device mechanical syringe (Avanca Medical Devices, Albuquerque, NM, USA). The mechanical syringe is formed around the core of a conventional syringe barrel and plunger, but has a parallel aspiration plunger and barrel to control the motion of the aspiration plunger (Figure 2A). The 2 plungers are mechanically linked by a pulley in an opposing fashion, resulting in a set of reciprocating plungers. Thus, when the aspiration plunger is depressed with the thumb, the syringe aspirates, and when the injection plunger is depressed with the thumb, the syringe injects (Figure 2B). This permits the index and middle fingers to remain in 1 position during both aspiration and injection, while the thumb only needs to move in a horizontal plane to the alternative plunger to change the direction of aspiration or injection. Mechanical syringes permit greater control when used with sonography and allow easy detection of small amounts of synovial fluid that flash back into the barrel, confirming true IA positioning17,31,32,33,34,35,36.
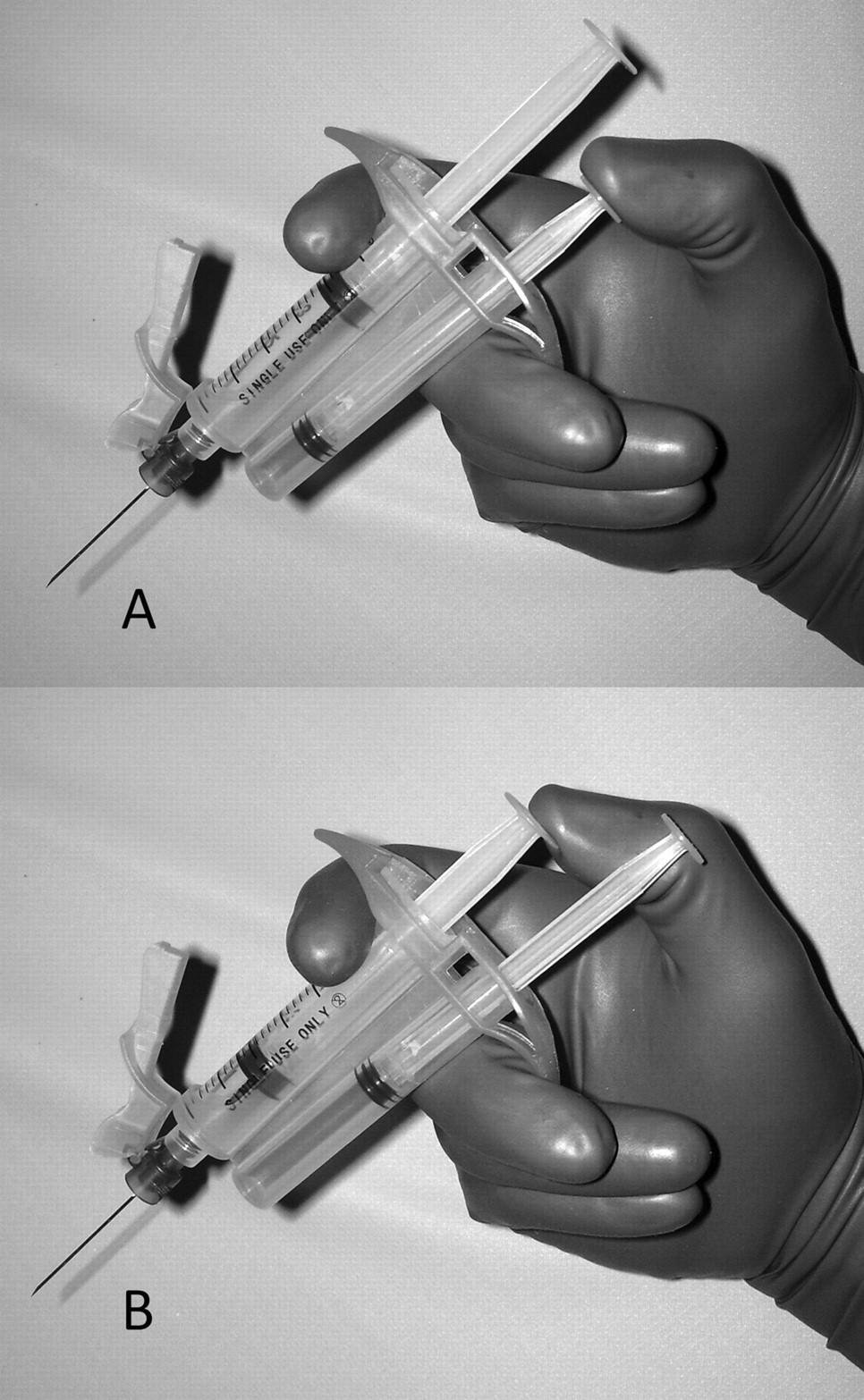
Mechanical safety syringe with safety needle. The mechanical syringe has 2 barrels and 2 plungers, an aspiration plunger and an injection plunger, that are connected by a pulley, creating reciprocating plungers. To aspirate, the thumb depresses the aspiration plunger (A), and to inject the thumb depresses the injection plunger (B).

Insertion of the needle. Under direct sonographic visualization, the needle attached to a mechanical syringe is introduced under the ultrasound transducer, with the needle directed at right angles to the plane of the ultrasound beam.

Sonographic needle introduction. The needle is advanced under direct sonographic guidance until the needle tip has pierced the synovial membrane overlying the cartilage. The mechanical syringe is used to determine aspiration of fluid, and then 1% lidocaine is injected to anesthetize the structures, determine movement of fluid along the cartilage faces, and assure IA positioning.
Prior to the procedure, the mechanical syringe was filled with 1–5 ml (depending on joint size) of 1% lidocaine (Xylocaine® 1%, AstraZeneca Pharmaceuticals LP, Wilmington, DE, USA). Next, the relevant anatomic landmarks were palpated and marked. A portable ultrasound unit with a 10-5 MHz 38 mm broadband linear array transducer (Sonosite M-Turbo, SonoSite Inc., Bothell, WA, USA) was used to sonographically determine the location of the joint and needle tip. Prior to inserting the needle, the long axis of the ultrasound transducer was placed coplanar with the long axis of the needle so that the ultrasound beam would be at 90° to the long axis of the needle (Figure 3)17. After penetrating the puncture point, the needle was then directed under the transducer toward the joint until the needle tip directly penetrated the synovial membrane and the bevel was wholly within the intraarticular space (Figure 4). Lidocaine was then injected intraarticularly with needle tip positioning established by direct sonographic imaging, observation of the flow of fluid from the needle into the IA space, and the demonstration of dilation of the intraarticular space (Figure 5) or by return of synovial fluid by aspiration17. Extraarticular injection was demonstrated by observing (1) fluid movement into extraarticular tissues; (2) increased signal in the surrounding fat; and (3) lack of fluid movement into and lack of dilation of the IA space17. In the case of extraarticular positioning, the needle was manipulated by advancing and or rotating the bevel until the injection of lidocaine was truly IA, as described above. After fluid flow along the cartilage face of the joint was established by direct visualization with ultrasound, the remainder of the lidocaine was completely injected intraarticularly to lift the synovial membrane over the needle bevel, and using one hand to hold the mechanical syringe and the other hand the needle hub, the mechanical syringe was rotated off the IA needle, and a 3 ml conventional syringe prefilled with triamcinolone acetonide suspension (Kenalog® 40, Westwood-Squibb Pharmaceuticals, New York, NY, USA) was rotated onto the IA needle (20 mg for small joints, 60 mg for intermediate joints, and 80 mg for large joints). The treatment was injected under direct sonographic visualization, with IA positioning again confirmed by fluid flow along the cartilage face with simultaneous dilation of the IA space (Figure 6). The needle was then extracted, and firm pressure applied to the puncture site, followed by application of an adhesive sterile dressing. All patients were instructed to rest the injected joint for 1 week, and then only cautiously resume activity. No physical therapy or changes in medications were recommended after injections.

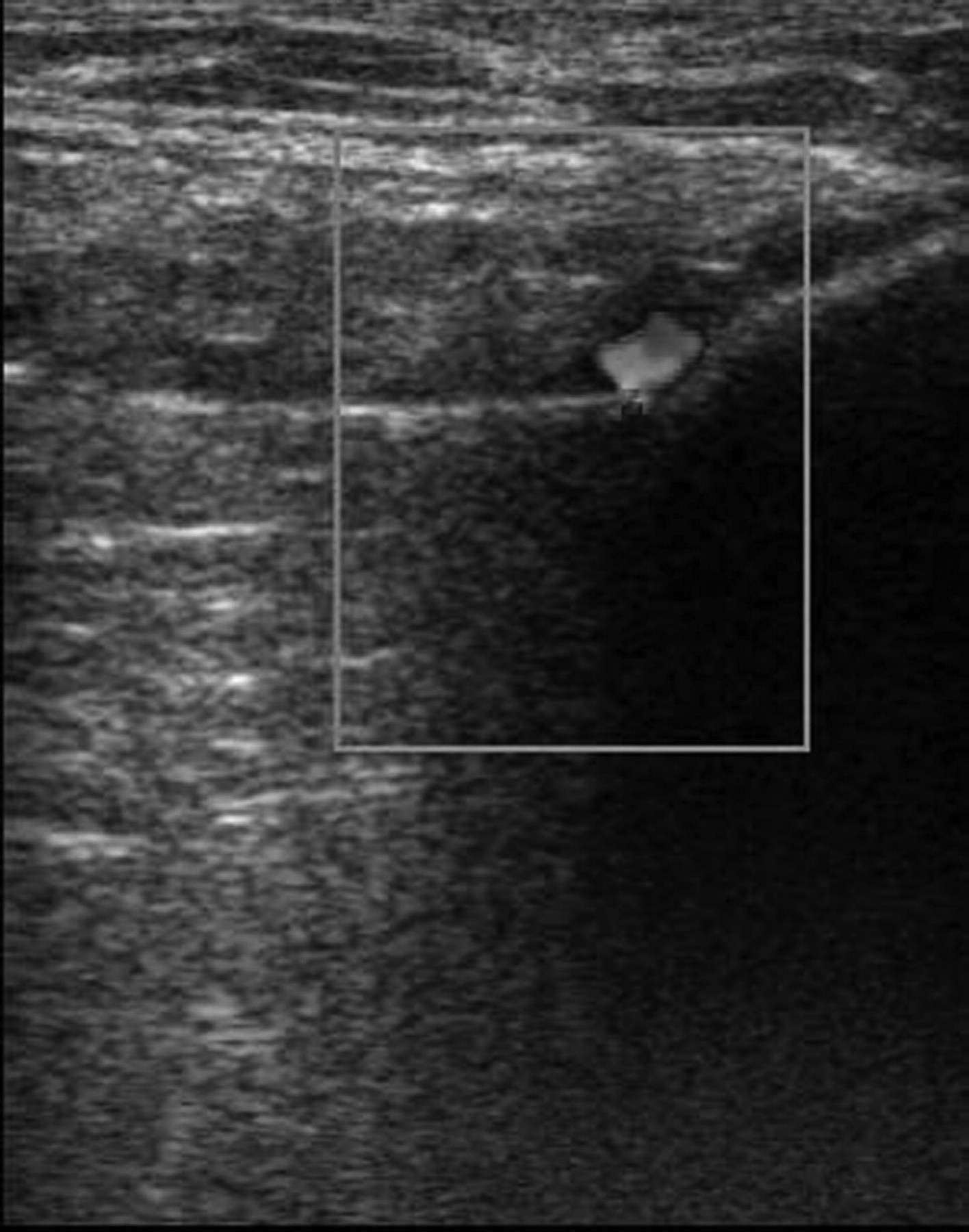
Sonographic visualization of direct IA injection. After manipulation and rotation of the bevel, the needle tip is in a completely IA position, as can be observed by the presence of sonographically visible movement of fluid within the joint (color Doppler enhancement) and dilation of the IA space of intraarticularly injected lidocaine over the articular cartilage.

Dilation of the IA space. After injection of lidocaine to dilate the IA space and assure that the bevel is completely within the synovial space, a syringe exchange is performed and triamcinolone is injected, further dilating the local IA space.
Palpation-guided injections
The palpation-guided injection procedure was also performed in a standardized manner using the 1-needle 2-syringe technique exactly as above but without sonographic guidance. A 3 ml to 20 ml conventional syringe (Ref. 309604, Becton Dickinson) as appropriate was operated with 2 hands and was used for all palpation-guided procedures.
Statistical analysis
Data were entered into Excel (Version 5, Microsoft, Seattle, WA, USA) and analyzed in SAS (SAS/STAT Software, Release 6.11, Cary, NC, USA). Differences between parametric 2-group data were determined with the t test with significance reported at the p < 0.05 level. Differences in categorical data were determined with Fisher’s exact test, while differences between multiple measurement data sets were determined with Fisher’s least significant difference method. Corrections were made for multiple comparisons. Correlations between measurement data were determined with logistic regression and between nonparametric data with Spearman’s correlation and the Kendall rank method.
RESULTS
As can be seen in Table 1, the characteristics of the 2 treatments groups were very similar, including number of subjects (p = 0.5), age (p = 0.31), sex (p = 0.31), subjects who completed the study (p = 0.5), subjects with RA (p = 0.82), number of small joints (p = 0.87), intermediate joints (p = 0.80), and large joints (p = 0.72), and preprocedure baseline pain (p = 0.4).
Characteristics of the study populations.
Tables 2, 3, and 4 demonstrate the outcomes of IA injection of inflammatory arthritis with and without image guidance. As can be seen, IA corticosteroid injections using anatomic palpation guidance were effective in relieving pain, resulting in a 69% reduction in absolute pain scores at 2 weeks (baseline VAS 7.5 ± 1.5 cm; 2-week VAS 2.3 ± 2.7 cm; p < 0.001) with absolute responder rate of 47% as defined by an asymptomatic joint (VAS < 2 cm) at the 2-week outcome23. Duration of therapeutic effect was 3.8 ± 1.8 months, and time to reinjection was 7.7 ± 3.4 months (Table 3). Thus, as previously shown in the literature, needle guidance by anatomic palpation is effective for IA corticosteroid injections, with reductions in absolute pain scores and a reasonable therapeutic duration12,14,17. These generally acceptable results with conventional methods are an obvious barrier to overcome for sonographic image-guided needle procedures to demonstrate statistical superiority.
Short-term outcome of injection to treat inflammatory arthritis.
Intermediate outcomes of injection to treat inflammatory arthritis.
Long-term outcome of injection to treat inflammatory arthritis.
Direct comparisons between conventional palpation-guided methods and ultrasound-guided methods are shown in Tables 2, 3, and 4. There were minimal differences (3%) in preprocedure pain between the 2 treatment groups (p = 0.4). However, sonographic image-guided IA injections of joints with inflammatory arthritis were significantly less painful than the conventional palpation method, causing 33% less absolute procedural pain (needle introduction pain) and 40% fewer individuals with significant procedural pain (procedural VAS pain score ≥ 5 cm), as well as 81% less injection pain and 87% less significant injection pain (all p < 0.01).
Short-term (2-week) therapeutic responses to the 2 injection methods are shown in Table 3. In all therapeutic measures, sonographically directed procedures were superior to palpation-guided methods: absolute VAS pain scores at 2 weeks were 35% lower (p < 0.012), responder rates were 38% higher (p < 0.003), and nonresponder rates were 34% lower (p < 0.003). Longterm outcomes are shown in Table 4. With sonographic guidance, the duration of therapeutic effect was significantly increased by 32% (1.2 months; p < 0.0001), while time to next procedure was increased by 12% (0.9 months, p = 0.034).
Procedural costs for a third-party payer (US Medicare) are also shown in Table 4. The use of sonographic guidance for a hospital outpatient modestly reduced the costs per patient per year by 8% ($7) relative to palpation-guided methods. More importantly, sonographic guidance significantly reduced the cost per responder per year by 33% ($64; p < 0.0001). Thus, for a hospital outpatient, sonographic guidance improved both short-term and longterm outcomes, and did not increase the cost per year per patient, while markedly reducing costs per responder per year.
DISCUSSION
Intraarticular injections comprise 64%–90% of all outpatient musculoskeletal procedures36,37,38,39,40. Intraarticular therapies should be injected accurately into the IA space and not into extraarticular structures such as the subcutaneous fat, fascial planes, or other subsynovial tissues, to achieve the maximal potential therapeutic benefit1,37,38,39,40,41,42,43,44,45. When a large effusion is present, synovial fluid can be aspirated, confirming true IA positioning of the needle tip1,41,42,43,44,45. In the noneffusive or “dry” joint, anatomic landmarks and tactile feedback are used to position the needle tip, but unintended extraarticular injection is common1,2,3,4,5,6,7,8,9,10,11.
However, injection accuracy is highly dependent on both approach and technique. Toda and Tsukimura reported that palpation-guided injection accuracy was 55% to 100%, depending on anatomic approach3. Lopes, et al reported 100% accuracy in injection rates4, while Im, et al reported only 76.3% injection success5. Jones, et al demonstrated that only 66% of palpation-guided injections were truly IA, while Bliddal reported 91% accuracy2,3,4,5,6,7,8. In a cadaver study, Esenyel, et al demonstrated a 56% to 85% IA injection accuracy depending on anatomic approach6. Jackson, et al demonstrated that palpation-guided injections were 71% to 93% accurate depending on anatomic approach8.
A number of studies have demonstrated that sonographic guidance provides greater accuracy and improved the outcomes9,10,11,12,13,14,15,16,17. Kane, et al found that ultrasound was better than clinical examination in determining the presence of joint effusions9, and Delaunoy, et al determined the volume sensitivity of sonography for articular effusion10. Balint, et al reported that sonography improved successful joint aspiration from 32% to 97%11. Qvistgaard, et al demonstrated that sonography improves injection accuracy12, and Pendleton, et al that sonography can predict the response to corticosteroid injection13. Raza, et al and Im, et al found that ultrasound-guided needle placement resulted in significantly greater accuracy than palpation-guided injection of joints5,14. Eustace, et al reported that patients whose injections had been accurately placed improved to a greater degree in the short term than those whose injections had been less accurately placed15. Naredo, et al reported significantly improved accuracy and outcomes of sonographic-guided IA injection procedures16. Cunnington, et al demonstrated that sonographic guidance was significantly more accurate than palpation guidance46. Sibbitt, et al reported that integration of sonographic guidance into a joint injection clinic significantly improved overall short-term outcomes and responder rates relative to palpation-guided injections17. Thus, the literature indicates that sonographic guidance improves the accuracy of IA injections, but improvement in outcomes and cost-effectiveness has not been demonstrated to the satisfaction of many experts18,19,20,21,22,46.
In our study, sonographically directed IA injections were superior to palpation-guided methods in all therapeutic measures: absolute VAS pain scores for injection pain were 81% less, responder rates were increased by 38%, and non-responder rates were reduced by 34% (Tables 2 and 3). Thus, sonographic image guidance is superior to palpation-guided injection for inflammatory arthritis. The cause of improved outcomes is uncertain, but certainly increased accuracy of placement of the IA therapy is likely the major cause of improved outcomes9,10,11,12,13,14,15,16,17. However, several other factors may all have contributed to improved outcomes: less needle trauma to synovial membrane during the procedure, less IA hemorrhage, more complete dilation of the IA space with lidocaine prior to injecting the corticosteroid, and an enhanced ability to aspirate synovial fluid to prove IA placement and to decompress the joint17,47.
Our study also demonstrates that the sonographic image-guided IA injections for inflammatory arthritis were significantly less painful than palpation-guided methods, causing 48% less absolute procedural pain and 58% less significant pain (Table 2). Although the causes of reduced procedural pain are uncertain, better control and direction of the needle tip away from pain-sensitive structures is a likely explanation17,31,32,33,34,35,36,47. An alternative explanation is that the cooling effect of ultrasound gel, the pressure from the ultrasound transducer, and the patient observing the sonographic image may have distracting effects at the neurocognitive level, significantly reducing pain and anxiety17,48,49.
In our study, there is a potential bias in that the palpation-guided procedures were performed by experienced proceduralists while the sonographic injections were performed by less experienced fellows; thus, the differences between palpation and sonographic-guided groups might be even greater if both arms had been performed by experienced proceduralists. Other variables could also have been studied, including specific anatomic portals, direct 1-step injection, different or no local anesthetics, operators with different experience levels, patients with RA alone, and various degrees of effusion, but these variables were beyond the scope of our study.
Cost-effectiveness for IA injections is highly dependent on reimbursement rates, and requires balancing the increased costs of sonographic guidance against a greater responder rate and a reduced use of other healthcare resources, in this case, reducing the costs of reinjection or referral for surgery (Table 4)50,51,52,53,54. Sonographically directed procedures were superior in performance, patient outcomes, and cost-effectiveness (Tables 2, 3, and 4) in a hospital outpatient setting due in part to a longer therapeutic duration and thus a longer time to next injection, both of which contribute to fewer costs per year (Table 4). However, if outcome data for a hospital outpatient are used to calculate costs for a physician office, although better outcomes are obtained, sonographic image guidance is not cost-effective because of the markedly increased costs ($183 per procedure) for ultrasound guidance in a physician’s office compared with the much lower cost of the basic injection procedure ($51–$73; Table 4)18. That being noted, calculations of cost-effectiveness for sonographic image guidance performed in a physician’s office were unreliable, as our study was performed only in a hospital outpatient environment. Thus, because of differences in access to medical care and the utilization of healthcare resources, real physician’s office data are required to come to meaningful conclusions. The cost-effectiveness of sonographic guidance for injection for inflammatory arthritis treatment performed in a physician’s office remains to be determined but is anticipated to be highly dependent on reimbursement rates18,30.
For a hospital outpatient, sonographic guidance was shown to be less costly and more cost-effective than conventional injection. Medicare bundles the costs of image guidance into the generally higher reimbursement of hospital-based care, thus reducing the cost of sonography for an individual procedure30,50. Therefore, the use of sonographic guidance for a hospital outpatient reduces the costs per patient per year by 8% ($7) and reduces the cost per responder per year by 33% ($64) relative to palpation-guided methods (Table 4). Clearly, sonographic image guidance for injection of inflammatory arthritis in a hospital outpatient is cost-effective because it provides both substantially better outcomes and lower costs.
There are certain limitations to these cost-effectiveness analyses. First, the analysis concerning inflammatory arthritis does not apply to the osteoarthritic joint as the synovial target. Both synovial fluid and hypertrophied synovial tissue mass in the inflammatory or rheumatoid joint are much larger than the synovial target in the noneffusive osteoarthritic joints, thus palpation-guided injections to treat inflammatory arthritis are more likely to be consistently intraarticular or intrasynovial4. This would have the effect of converging the palpation and image-guided groups. Further, inflammatory arthritis due to gout, calcium pyrophosphate deposition disease, or other forms of acute inflammatory arthritis could not be addressed because our study specifically excluded these other forms of arthritis and included only chronic autoimmune inflammatory arthritis. The increased responder rate with sonographic guidance may be of societal value beyond costs to a third-party payer (better quality of life, less lost work, and fewer disability payments), thus, since outcomes are better, there may be a justification for using sonographic guidance for injection of inflammatory arthritis regardless of increased procedural costs50,51,52,53,54,55,56.
Physician or institutional costs including the expense of acquisition and maintenance of the ultrasound machine, image storage and sonographic supplies, and the increased operator setup and procedure time were not included in this analysis, but generally do not directly affect the cost to a third-party payer. Those expenses and time do affect the profit or loss for the proceduralist or institution. Importantly, reimbursement rates vary from year to year and from country to country; thus cost-effectiveness estimates will always be different in each country and state, and will always be changing, a definite limitation to our study30,50,51,52,53,54.
In our analysis, reinjection rate and referral for surgery were additional costs to the third-party payer; there may have been other cost savings of sonographic guidance related to fewer consults, fewer clinic visits, fewer major surgical and reconstructive procedures, and less use of and complications from oral corticosteroids, nonsteroidal antiinflammatory drugs and pain medications50,51,52,53,54. These actual costs were difficult to calculate due to patients having multiple physicians, confounding conditions, taking medications for other conditions, the restricted study time (1 year), and the complexity and heterogeneity of the third-party payer mix with different reimbursement rates. The rounding down of both therapeutic duration to a maximum of 6 months and the time to next injection to 12 months would have the effect of reducing the cost-effectiveness estimate, thus actual cost-effectiveness may be more favorable for sonographic guidance than our analysis reflects.
Diagnostic ultrasound and sonographic guidance are increasingly being integrated into the mainstream of musculoskeletal medicine; outcome and cost-effectiveness studies are important to justify this potentially expensive practice transformation20,30,55,56,57. Our research provides additional data on outcome, and is one of the first studies examining costs and cost-effectiveness of sonographic guidance for injection to treat inflammatory arthritis with relevance for both the clinician and the design of clinical trials. Our study demonstrates that IA injections of inflammatory arthritis performed with sonographic image guidance significantly and meaningfully improve outcomes and enhance cost-effectiveness.
- Accepted for publication September 27, 2010.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}