

Abstract
Objective. To identify factors associated with radiographic progression at 52 weeks in patients with rheumatoid arthritis (RA) after 12 weeks of methotrexate (MTX) therapy.
Methods. The study population consisted of patients from the MTX arm of the Trial of Etanercept and Methotrexate with Radiographic Patient Outcomes (TEMPO). Logistic regression analysis was used to identify clinical and laboratory assessments performed at Week 12 of MTX therapy that might be associated with Week 52 radiographic outcome (modified total Sharp score). Classification and regression tree (CART) modeling of the Week 12 assessments was used to determine the subgroups of patients with the best and worst radiographic outcomes.
Results. A total of 169 patients were analyzed: 116 patients in the best radiographic outcome group and 53 patients in the worst radiographic outcome group. Logistic regression analysis showed that Week 12 C-reactive protein (CRP) level, erythrocyte sedimentation rate, tender joint count, swollen joint count (SJC), and Health Assessment Questionnaire scores were significantly associated with radiographic progression at Week 52 (p < 0.05 for each assessment). CART modeling showed that patients with Week 12 CRP > 0.67 mg/dl and SJC > 1 and patients with Week 12 CRP ≤ 0.67 mg/dl and SJC > 10 were likely to show the worst radiographic progression at Week 52. The CART model had a sensitivity of 85%, specificity of 60%, and overall classification accuracy of 68%.
Conclusion. In patients with RA, measures of CRP and SJC after 12 weeks of MTX therapy emerged as the factors most associated with radiographic progression at Week 52.
Rheumatoid arthritis (RA) is a chronic, inflammatory disease that leads to progressive joint damage, often at an early stage. In many patients with RA, the disease course is progressive, resulting in functional impairment and a decline in overall quality of life. Early treatment intervention appears to be important in reducing radiographic progression and retaining functional ability in patients with RA.
Radiographic progression and subsequent decline in functional status are linked to sustained disease activity in patients with severe RA1. Several studies have shown a relationship between individual markers of disease activity and radiographic progression2,3. Some of these factors include elevated levels of the acute-phase reactant C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR), swollen joint counts (SJC), and high Disease Activity Score (DAS)4,5,6.
Methotrexate (MTX) is the most commonly prescribed disease-modifying antirheumatic drug (DMARD) for patients with RA. A key challenge in managing RA is the difficulty in determining which patients receiving therapeutic doses of MTX therapy will continue to have radiographic progression. The ability to identify those patients at a higher risk for radiographic progression in the early months of MTX therapy could allow for early, informed decisions regarding optimal treatment to reduce progression and preserve functional ability.
Our objective was to find, after 12 weeks of MTX therapy, the clinical and laboratory assessments that would identify patients at the highest risk of radiographic progression at 52 weeks. We performed a retrospective analysis using patient data from the Trial of Etanercept and Methotrexate with Radiographic Patient Outcomes (TEMPO)7. We evaluated various clinical and laboratory assessments after 12 weeks of MTX therapy in patients who showed the greatest radiographic progression at 52 weeks and compared them with similar assessments in patients who showed no radiographic progression. Finally, a model was developed to evaluate the association between certain combinations of Week 12 assessments and radiographic progression at 52 weeks.
MATERIALS AND METHODS
Patients
Patient data from the MTX arm of the TEMPO trial were used in this analysis. Details regarding the TEMPO methods and patient population have been reported7. All patients provided written informed consent. The trial was conducted in accord with the Declaration of Helsinki, the US Food and Drug Administration, and the International Conference on Harmonisation Guidelines on Good Clinical Practice. An institutional review board at each study center reviewed and approved the informed consent form, the study protocol, and all protocol amendments.
Assessments
Patient assessment was based on the following measures: CRP, ESR, tender joint count (TJC), SJC, Health Assessment Questionnaire (HAQ) score, physician’s global assessment, patient’s global assessment, and patient pain assessment (visual analog scale). Radiographic outcome was assessed as modified total Sharp score (TSS)8.
Statistical analysis
This analysis focused on 2 patient groups that were identified by TSS at 52 weeks. One group consisted of patients who showed no radiographic progression (TSS ≤ 0). The second group consisted of patients who showed the worst radiographic progression, representing the top 25% of the study population. The cutoff value for the patients with worst progression turned out to be TSS = 2.5. Descriptive statistics were used to summarize patient demographics, disease characteristics, and Week 12 assessments in the no-progression and worst-progression groups. Medians and interquartile ranges were calculated for the continuous variables, and frequencies and percentages were calculated for the categorical variables. Because the data were not normally distributed, the Mann-Whitney U test was used to compare differences between the groups. Logistic regression analyses were performed to identify individual Week 12 assessments associated with progression at Week 52, after adjusting for baseline differences in disease duration and rheumatoid factor. OR and associated 95% CI were calculated. Results were considered significant at p ≤ 0.05, 2-sided.
A certain combination of clinical and laboratory variables may yield a more effective classification model than when measurements are used singly. Using the data of patients with no progression and with worst progression, a Classification and Regression Tree (CART) analysis9,10 was conducted to develop a model for identifying Week 12 assessments that characterized the 2 progression groups. The CART model relies on statistically optimum recursive splitting of the patients into smaller and smaller subgroups, based on the critical levels of the prognostic variables. In the implementation of CART, the dataset is split into the 2 subgroups that are the most different with respect to the radiographic outcome (no progression vs worst progression). The percentages of patients with no progression or worst progression were calculated for the base branches of the regression tree. The accuracy of the CART model was expressed in terms of sensitivity, specificity, and overall accuracy.
Analyses were performed with SAS STAT® system Version 9.1 (SAS Institute Inc., Cary, NC, USA) and CART® Version 6.0 (Salford Systems, San Diego, CA, USA).
RESULTS
Baseline demographics and disease characteristics
The total number of patients from the MTX arm of the TEMPO trial was 2287, of whom 212 had radiographic data at Week 52. Our analysis included 169 of those 212 patients; 116 patients were in the no radiographic progression group, and 53 patients were in the worst radiographic progression group. Baseline demographics and disease characteristics are shown in Table 1. In general, baseline disease characteristics indicated greater severity in the worst-progression group than in the no-progression group, with significant differences for TSS, CRP, ESR, SJC, and HAQ.
Baseline demographics and disease characteristics in patients with rheumatoid arthritis. Numbers are median (IQR) unless otherwise noted. The Mann-Whitney U test was used to determine statistical significance between no-progression and worst-progression groups. A p value < 0.05 was considered statistically significant. P values are for descriptive purposes. No multiple testing corrections were performed.
Individual Week 12 assessments associated with Week 52 radiographic progression
Week 12 acute-phase reactant levels, joint counts, and HAQ scores are shown in Table 2. Higher acute-phase reactant levels and joint counts after 12 weeks of MTX therapy were associated with increased radiographic progression at 52 weeks. Although patients in both the no-progression and worst-progression groups showed improvements in CRP and ESR levels at Week 12, the absolute values of these measures were significantly higher in the worst-progression group (p < 0.01 for each assessment). Patients in the worst-progression group also had higher TJC and SJC scores compared with patients in the no-progression group (p < 0.05 for each assessment). Significant differences in HAQ scores were observed between the worst-progression and no-progression groups (p < 0.05) only after adjusting for baseline differences in disease duration and rheumatoid factor.
Week 12 clinical and laboratory assessments individually associated with radiographic progression at Week 52. Mann-Whitney U test was used to determine statistical significance between no-progression and worst-progression groups and to generate p values. Logistic regression analysis was used to identify association with radiographic progression, after adjusting for baseline differences in disease duration and rheumatoid factor. A p value < 0.05 was considered statistically significant.
Results of the logistic regression analysis are shown in Table 2. Five assessments at Week 12 (CRP, ESR, SJC, TJC, and HAQ) were individually identified as significantly associated with radiographic progression at Week 52. From a clinical perspective, these findings suggest that if a patient’s CRP level was 2 mg/dl after 12 weeks of MTX therapy, the patient had a 29% increased risk (OR 1.29) of developing radiographic progression at 52 weeks compared with a patient whose Week 12 CRP level was 1 mg/dl (p = 0.01). Similarly, the risk of developing radiographic progression was increased by 21% if the Week 12 ESR level was 20 mm/h versus 10 mm/h (p = 0.03), by 15% if the Week 12 TJC was 10 versus 5 (p = 0.04), by 27% if the Week 12 SJC was 10 versus 5 (p = 0.02), and by 73% if the Week 12 HAQ was 2 versus 1 (p = 0.03).
CART model for radiographic progression at Week 52 based on Week 12 data
Week 12 data from patients with no progression and patients with worst progression were entered into the CART model. The patients with CRP ≤ 0.67 mg/dl and SJC ≤ 10 were not likely to show radiographic progression at Week 52. The patients with CRP > 0.67 mg/dl and SJC > 1 and the patients with CRP ≤ 0.67 mg/dl and SJC > 10 were likely to show the worst progression at Week 52 (Figure 1). This CART model had a sensitivity of 85%, a specificity of 60%, and an overall accuracy of 68%.
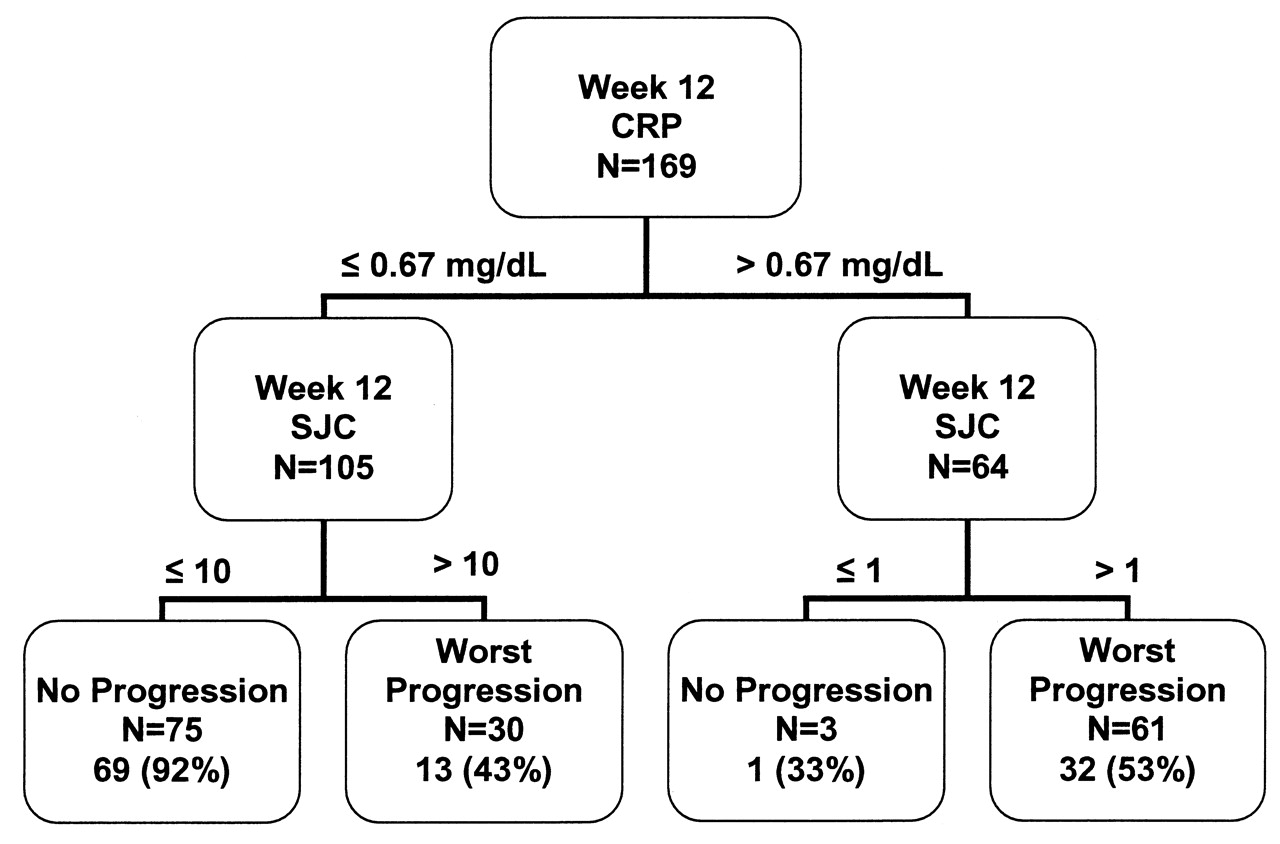
Classification and Regression Tree model for factors associated with radiographic progression. CRP: C-reactive protein; SJC: swollen joint count.
DISCUSSION
Methotrexate has become a mainstay of DMARD treatment for patients with RA and is often the first-line DMARD. Although MTX is highly effective in treating the signs and symptoms of RA and has an adequate safety profile, studies have shown that many patients receiving MTX therapy continue to have radiographic progression7,11. In this analysis, we examined clinical and laboratory assessments in patients from the TEMPO trial after 12 weeks of MTX therapy to identify factors associated with radiographic progression at 52 weeks.
The association between elevated RA assessments and radiographic progression has been reported in several studies4,5,12. More recently, high levels of acute-phase reactants and high SJC scores were found to be associated with increased radiographic progression in a subset of patients with early RA treated with MTX for 14 weeks13. Although acute-phase reactant levels may be useful indicators of radiographic progression over time, laboratory values at a certain timepoint may not always be available to the physician. In this regard, joint count scores may take on greater importance as early indicators of progression. The results of our CART analysis support the value of joint counts, as we found that SJC, especially in combination with CRP, was associated with future radiographic progression. It is significant that SJC had a greater association with radiographic progression than did TJC.
Physicians often use MTX as a first-line therapy for patients with RA and evaluate treatment response after 3 to 6 months. Although MTX treatment is known to slow the process of joint destruction in patients with RA, treatment with biologics, especially when used in combination with MTX, has been shown to be more effective than MTX alone in slowing joint damage in patients with RA14. Therefore, the early identification of patients on a therapeutic dose of MTX who are at a higher risk of developing longterm radiographic progression may lead to better management of RA.
Our analysis has several limitations. The no-progression and worst-progression groups were defined based on the radiographic outcomes at Week 52 using artificial cutoffs. Therefore, the findings may not be reflective of a real-world patient population. Additionally, this was a retrospective evaluation of patient data, and retrospective analyses must be interpreted with caution. Despite these limitations, our findings may be valuable to clinicians. Further studies are warranted to better understand the association between RA assessments and radiographic progression.
Our analysis demonstrates that, after 12 weeks of MTX therapy, a simple model using Week 12 CRP and SJC may be useful in indicating Week 52 radiographic progression. Thus, early identification of patients with an increased risk of debilitating progressive joint damage may be feasible as early as 12 weeks after initiation of MTX therapy. Our findings allow an informed decision regarding which patients may or may not need more aggressive treatments after a relatively short exposure to MTX.
Acknowledgment
The authors thank Meera Kodukulla, PhD, and Michele Vivirito (Amgen Inc.) for writing assistance.
Footnotes
-
Study and analysis funded by Amgen Inc. and Pfizer Inc.
- Accepted for publication September 20, 2010.








{kind=link}